
Abstract
Background
The nose is a prime esthetic focus of the human face and it is a common site for nonmelanoma skin cancers. Esthetic reconstruction of nasal skin after tumor resection remains a problem. Beside conservative surgical excision of the skin tumor, this article presents a tactic for decreasing the size of the skin defect and optimizing its shape to facilitate reconstruction.
Methods
Throughout a period of seven years, thirty-five patients with nonmelanoma cancer of nasal skin were managed by a one stage surgical operation, which entails conservative tumor resection followed by performing an esthetic rhinoplasty that remodels the nasal skeleton in order to shrink the skin defect; making it more amenable to reconstruction by adjacent skin.
Results
Results were satisfactory for all patients in terms of adequate tumor resection and pleasant appearance of their noses.
Conclusions
Esthetic rhinoplasty is a useful adjunctive technique in nasal oncoplastic surgery.
1 Introduction
Facial features play an important role in human interaction. The nose; being the center point of the face, is a major contributor to the shape of the human face. The integrity of the nasal shape is a basic need for social interaction and an esthetically pleasing nose is a booster for self-esteem.
Figure 5 Example (2) for adjunctive esthetic rhinoplasty in nasal oncoplastic surgery. (a) Pre-operative views of a nose harboring squamous cell carcinoma at the tip. (b) Post-operative views after tumor excision, esthetic rhinoplasty, and reconstruction by axial frontonasal flap.

The skin of the nose is the commonest site of facial non-melanoma skin cancer; namely basal cell carcinoma and squamous cell carcinoma.Citation1–Citation4 Considering the complex topographic anatomy of the nose and the limited laxity of its skin, nasal defects that arise from surgical excision of those tumors are usually a challenge to esthetic reconstruction.Citation5–Citation7
This article advocates performing esthetic rhinoplasty as an adjunctive surgical step that optimizes the condition of nasal defects for favorable esthetic reconstruction.
2 Patients and methods
The tactic of adjunctive esthetic rhinoplasty was adopted in 35 patients referred for excision of non-melanoma skin cancer of the nose, from December 2007 to December 2014.
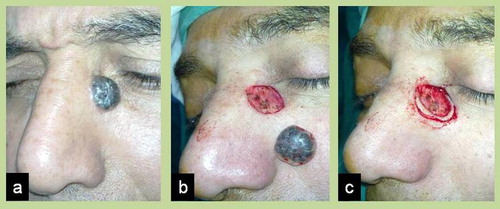
Surgery was performed under general anesthesia, with local infiltration of the perimeter of the surgical field with 1:10,000 norepinephrine. Excision of the tumor was carried out using loupe magnification and frozen sections histopathology to achieve minimal yet tumor-free surgical resection ().
Figure 1 Conservative resection of nasal skin tumor. (a) Basal cell carcinoma on lateral side of nose. (b) Excised tumor with 1 mm safety margin. (c) Additional rim excision dictated by frozen section histopathology.
After adequate excision of the tumor, and through the same wound of tumor excision or through the extra exposure provided by dissecting the flap that is planned for reconstruction, the nasal skeleton was remodeled using the necessary technique that suits each particular case, e.g. hump resection, L-shaped excision of cartilaginous septum, cephalic trim of lower lateral cartilages, lobular alar cartilage incision and overlay, lateral crural steal or overlay, and inter-domal tip refining sutures ( and ).
Figure 2 Remodeling of nasal skeleton. (a) Exposure of nasal skeleton through the wound of tumor excision. (b) During resection of nasal dorsal hump.
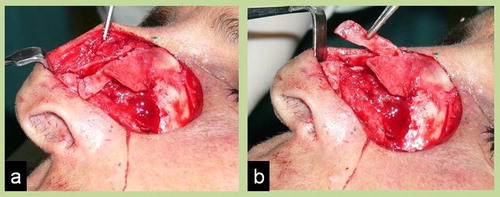
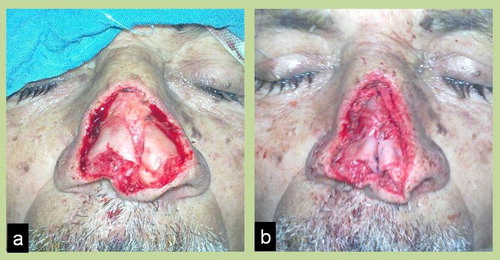
Figure 3 Remodeling of nasal tip. (a) Skin defect before tip modification. (b) Skin defect after tip modification by cephalic trim of alar cartilages, lobular cartilage incision and overlay, lateral crural steal, and inter-domal sutures.
Skin flaps that were used for skin resurfacing of the nose included bi-lobed flaps,Citation8–Citation10 nasolabial transposition flaps,Citation11,Citation12 Propeller facial artery perforator flaps,Citation13 and axial frontonasal flaps.Citation14,Citation15
3 Results
Out of the 35 patients treated by the abovementioned methods, 26 patients (74.3%) had basal cell carcinoma and 9 patients (25.7%) had squamous cell carcinoma. They were 21 male and 14 female patients. The age of patients ranged from 47 to 82 years and the mean age at the time of surgery was 59.9 years.
The flaps used for nasal skin reconstruction in these 35 patients were 7 bi-lobed flaps, 6 nasolabial transposition flaps, 5 Propeller facial artery perforator flaps, 13 axial frontonasal flaps, and 4 combined axial frontonasal and Propeller facial artery perforator flaps ().
Table 1 Distribution of flaps used for nasal reconstruction in the thirty-five cases.
Co-morbid conditions included hypertension, diabetes mellitus, smoking, and previous history of nasal skin cancer surgery.
Minor complications occurred in 4 patients in the form of minimal tip necrosis of the axial frontonasal flap, which healed well by secondary intention without any need for scar revision.
Results of esthetic rhinoplasty were totally satisfactory to most patients, i.e. they accepted the new shape of their noses very well.
Throughout the follow-up period that ranged from 6 months to 7 years (mean 41.5 months), there was no recurrence of the tumors.
– depict examples of the outcome of esthetic rhinoplasty as an adjunctive technique in nasal skin cancer surgery.
Figure 4 Example (1) for adjunctive esthetic rhinoplasty in nasal oncoplastic surgery. (a) Pre-operative views of a nose harboring basal cell carcinoma at the left side. (b) Post-operative views after tumor excision, esthetic rhinoplasty, and reconstruction by transposition nasolabial flap.
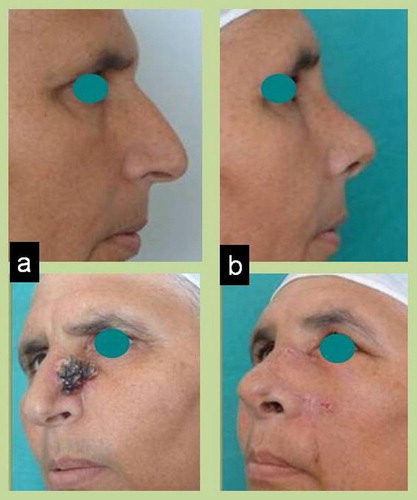
Figure 6 Example (3) for adjunctive esthetic rhinoplasty in nasal oncoplastic surgery. (a) Pre-operative views of a large central nasal defect after multiple recurrences of basal cell carcinoma. (b) Post-operative views after tumor excision, esthetic rhinoplasty, and reconstruction by axial frontonasal and propeller facial artery perforator flaps.

4 Discussion
The fact that the nose is a major esthetic focus of the face poses a great challenge to the plastic surgeon during reconstruction of skin defects resulting from excision of nasal skin cancer.Citation6,Citation7,Citation16,Citation17 Many studies discussed the parameters, methods, and complications of surgical treatment of non-melanoma skin cancers.Citation18–Citation25 Several factors are involved in preoperative analysis and planning of the surgical strategy. These factors include availability, color, texture, and contour of the adjacent skin, the topographic nasal subunit principle of Burget and Menick,Citation26 the general co-morbid conditions, and the patient expectations. Yet the pivotal factor that governs the choice of the reconstructive modality is usually the size of the defect. The larger is the defect the less the likelihood of perfect esthetic reconstruction will be.
A known strategy to limit the size of tumor resection is the use of frozen section histopathology during surgery.Citation27,Citation28 By virtue of the frozen section technique that was used for all the 30 patients enrolled in this paper, it was possible to cut down the safety margin of tumor resection to an average of 2.5 mm, with no recurrence at all throughout a mean follow-up period of 41.5 months. Besides, accuracy of frozen section histopathology was proved in all cases by standard hematoxylin and eosine (H&E stained sections) histopathology that revealed free resection margins and depths in all cases.
The aim of our work was to present another tactic for an extra diminution of the size of the defect by performing esthetic rhinoplasty as an adjunctive step after conservative tumor resection. This technique does not add any extra incisions to the nose (trans-columellar or infra-cartilaginous), but makes use of the exposure provided by tumor resection and by dissecting the flap(s) that would be used in reconstruction. Remodeling of the nasal skeleton does not only diminish the size of the skin defect but also optimize its shape and orientation for the best possible esthetic reconstruction.
The larger and broader is the nasal skeleton the more benefit this technique can yield, i.e. this technique works best for patients with large noses, not only in terms of the amount of shrinkage of the skin defect but also in the significant reduction to the overall size of their noses. Those patients get the benefit of esthetic reconstruction of the cancer defect plus a “bonus” esthetic rhinoplasty.
5 Conclusions
Esthetic rhinoplasty as an adjunctive step during resection of nasal skin cancers is a useful technique, which optimizes the condition of the skin defect for favorable reconstruction and optimizes the overall esthetic appearance of the nose, especially in patients with large noses.
Conflict of interests
The author declares that he has no conflict of interest, and has not received any financial or material support.
All procedures performed in the study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 15 January 2016
References
- A.C.SalgarelliP.BelliniA.MultinuReconstruction of nasal skin cancer defects with local flapsJ Skin Cancer201110.1155/2011/181093
- D.T.NetscherM.SpiraBasal cell carcinoma: an overview of tumor biology and treatmentPlast Reconstr Surg1135200474E94E
- N.N.GeJ.F.McguireS.DysonD.CharkNon-melanoma skin cancer of the head and neck II: surgical treatment and reconstructionAm J Otolaryngol3032009181192
- A.S.BoydY.ShyrL.E.KingBasal cell carcinoma in young women: an evaluation of tanning bed use and smokingJ Am Acad Dermatol4652002706709
- R.MeyerAesthetic aspects in reconstructive surgery of the noseAesth Plast Surg1241988195201
- D.K.HoasjoeF.J.StuckerR.F.AarstadAesthetic and anatomic considerations for nasal reconstructionFacial Plast Surg1041994317321
- S.R.BakerPrinciples of nasal reconstruction2nd ed.2011SpringerNY, USA
- J.A.ZitelliThe bilobed flap for nasal reconstructionArch. Dermatol.12571989957959
- M.ChoD.W.KimModification of the Zitelli bilobed flap: a comparison of flap dynamics in human cadaversArch Facial Plast Surg862006404409
- C.Y.XueL.LiL.L.GuoJ.H.LiX.XingThe bilobed flap for reconstruction of distal nasal defect in AsiansAesth Plast Surg3342009600604
- H.SteenfosP.TarnowG.BlomqvistExperience with the modified nasolabial transposition flap in nasal reconstructionScand J Plast Reconstr Hand Surg29119955152
- H.BiX.XingJ.LiNasolabial-alar crease: a natural line to facilitate transposition of the nasolabial flap for lower nasal reconstructionAnn Plast Surg7352014520524
- A.Ruiz-MoyaA.Lagares-BorregoP.Infante-CossioPropeller facial artery perforator flap as first reconstructive option for nasolabial and perinasal complex defectsJ Plast Reconstr Aesth Surg6842015457463
- D.MarchacB.TothThe axial frontonasal flap revisitedPlast Reconstr Surg7651985686694
- S.De FontaineM.KlaassenD.S.SoutarRefinements in the axial frontonasal flapBr J Plast Surg4651993371374
- P.KanofaosS.AlvarezJ.E.McKinnieR.D.WallaceNasal reconstruction: a simplified approach based on 419 operated casesAesth Plast Surg3920159199
- G.EskiizmirS.BakerC.CingiNonmelanoma skin cancer of the head and neck: reconstructionFacial Plast Surg Clin North Am2042012493513
- D.G.BrodlandJ.A.ZitelliSurgical margins for excision of primary cutaneous squamous cell carcinomaJ Am Acad Dermatol27211992241248
- D.J.WolfJ.A.ZitelliSurgical margins for basal cell carcinomaArch Dermatol12331987340344
- C.C.HuangS.M.BoyceSurgical margins of excision for basal cell carcinoma and squamous cell carcinomaSemin Cutan Med Surg2332004167173
- S.FernandesV.C.MaciasJ.CardosoEffect of positive surgical margins after initial resection of basal cell carcinomaDermatol Surg39112013139140
- S.Rodriguez-CampsNasal reconstruction after epitheliomaAesth Plast Surg2542001273277
- J.RustemeyerL.GuntherA.BremerichComplications after nasal skin repair with local flaps and full-thickness skin grafts and implications of patients’ contentmentOral Maxillofac Surg13120091519
- V.D.De PochatN.AlonsoE.B.RibeiroNasal reconstruction with the paramedian forehead flap using the aesthetic subunits principleJ Craniofac Surg256201420702073
- H.FischerNasal reconstruction with the paramedian forehead flap: details of successFacial Plast Surg3032014318331
- G.C.BurgetF.J.MenickThe subunit principle in nasal reconstructionPlast Reconstr Surg7621985239247
- T.J.MintonContemporary Mohs surgery applicationsCurr Opin Otolaryngol Head Neck Surg1642008376380
- F.LevinM.KhalilS.A.McCormickD.Della RoccaE.MaherR.C.Della RoccaExcision of periocular basal cell carcinoma with stereoscopic microdissection of surgical margins for frozen-section control: report of 200 casesArch Ophthalmol1278200910111015