
Abstract
Autologous fat transfer is a century-old method for both aesthetic and reconstructive purposes. It is considered by many plastic surgeons the ideal body filler. The only disadvantage is its variable degree of resorption, which ranged from 45% to 80%. Various groups have studied the effects of cryo-preservation for fat storage, the advantage being that fat harvesting need only be performed once, and thereafter fat injections can be performed using stored fat as an outpatient service. This a clinical study carried out to test the aesthetic outcome of serial injection of the cryo-preserved fat cells for both aesthetic and reconstructive purposes.
Methods
Clinical evaluation was performed under standardized condition for serial lipofilling between October 2003 and May 2012, and 364 autologous fat transfers were performed in 104 patients ranging in age from 18 to 69 years (mean age 34 years).
Results
The postoperative clinical results favored the use of serial fat transfer because the aesthetic and structural results were stable up to 90% of the initial volume more than a year after initial transfer.
Conclusion
Our data suggest that serial transfer of the cryo-preserved fat leads to better cosmetic results on the basis of outpatient service without increasing the financial burden for our patients.
Keywords:
1 Introduction
Structural fat graft, a term was introduced and popularized by Coleman decade ago, now is considered by many plastic surgeons a valuable tool for soft tissue augmentation in both aesthetic surgery and reconstructive surgery.Citation1
However, one of the main disadvantages of this technique to achieve long-term aesthetic results is the variable rate of fat resorption, and studies reported resorption rate ranges from 45% to 80% of the initial injected volume.Citation2–Citation5
Two mechanisms were suggested to explain this volume reduction: first, a direct reduction in the number of viable adipocytes occurs, followed by further volume loss with resorption of oil cysts from non-viable adipocytes.Citation6
Many plastic surgeons believe that throwing the excess lipoaspirate is great loss that makes preservation of the excess fat as a strong desire of both the plastic surgeon and the patient for future application.
It is our hypothesis that lipoaspirate obtained from conventional liposuction could be preserved and stored at low temperature (below −18 °C), and then serial (repeated) injections of small amounts of fat to overcome the fat resorption occur with single injection of fresh fat grafts.
We think that repeated transfers of small fat grafts ensure maximal take, and subsequently enhance the aesthetic results.
The purpose of the current study was to develop a novel approach to effectively preserve the aesthetic result obtained by autologous fat through serial injection of the cryo-preserved lipo-aspirates.
2 Patients and methods
The present study was performed according to the Guidelines of Good Clinical Practice and Scientific Committee of the School of Medicine. Written informed consent was obtained from all the patients, and pre-operative photographs for documentation also were obtained.
We explained our protocol to the patients, the protocol entailed 3–4 injections, and the first injection would be done using the fresh fat, then 2–3 injections would be done using the excess cryo-preserved fat, and the spaces between injections would be 3–4 weeks (the advantages of this monthly spaces were many, there was sufficient time for edema resolution, better judgment of the augmentation and there would be enough time for the patient to adapt her/his new figure for better psychological adjustment).
Between October 2003 and May 2012, we performed 364 autologous fat transfers in 104 patients ranging in age from 18 to 69 years (mean age 34 years).
The indications were the following:
66 Facial rejuvenations
17 Leg augmentations
6 Hand rejuvenations
4 Buttock augmentations
2 cases of post-burn scarring, one affecting the hand and the other involving the face.
2 cases for correction of post-liposuction irregularities
2 cases of labium majora augmentation
One case of correction of chest irregularities after gynecomastia surgery.
Fat injection volume ranged from 3 mL for facial rejuvenation to 350 mL in cases of buttock augmentation.
The mean volume infiltrated for facial augmentation was 7 mL; for extremities, it was 22 mL; for buttock augmentation 325 mL. Follow-up lasted 12–133 months (mean 39 months).
As a rule, we performed all facial and hand rejuvenation with the use of local anesthesia, with/without IV sedation. We performed the buttock augmentation and other correction (post-liposuction and post-gynecomastia surgery irregularities), with spinal anesthesia and less frequently general anesthesia.
The techniques started by marking of both the donor sites, which were usually the abdomen and less frequently the inner thighs and the recipient site after consultation with the patient.
Two small punctures were carefully placed in the groin crease, and a mixed solution (500 mL of Ringer lactate solution added with 20 mL of 2% lignocaine and 0.5 mL of 1:200,000 epinephrine) was infiltrated into the lower abdominal donor site using a blunt Lamis infiltrator (Byron Medical Inc., Tucson, AZ).
The infiltration solution was introduced very slowly to avoid rapid expansion that may cause pain to the patient in cases of using local anesthesia.
The lipoaspirate was harvested through the same incisions made previously: 2.1 mm diameters, 23 cm length with a blunt tip cannula (Tulip cannula (Tulip Medical, San Diego, CA) which was connected to a 60 mL tulip syringe (A).
Figure 1 (A and B) Both figures show different types of syringes used in both fat harvesting and transferring of fat graft.
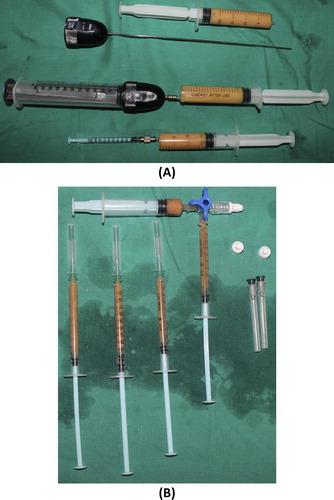
We have found that it was faster and more practical to use 60-mL syringes.
The processing of fat was done by simple sedimentation for 30 min.
After filling the syringe with harvested fat, the cannula was removed from the syringe. The harvested fat was divided into 10 cc syringes by connecting the 60-mL syringe to the 10 cc syringes by tulip connector (B).
The first injection was done using the fresh fat.
The excess lipoaspirate was cryopreserved in −18° for future application.
During the follow-up sessions, which were 3–4 sessions with 3–4 weeks intervals, under local anesthesia, we used the cryopreserved fat after slow rewarming for under correction by injecting small amounts of the re-warmed fat, and we injected one side of the face and let the patient to have a look and confirm that this side was satisfactory to her/him and then mimic the results to the other side.
We advised the patient to do massage of the injected area using warm compresses applying local antibiotic ointment and anti-edematous cream for three days post-injection.
3 Results
At the end of the first year following the fourth planned injection, both the patient (Patient satisfaction questionnaires) and the operating surgeon (s) did clinical evaluation of the aesthetic results, and the analysis of the data showed a tendency for better stable results especially that of the face.
95 autologous fat transfer (91.35%) resulted in significant aesthetic improvement, described as “good” or “very good” in postoperative checkups after 12 months after the last injection, comparison by surgeon and patients of pre- and postoperative control photographs showed the aesthetic and structural results to be stable up to 91% of the initial volume (–).
Figure 2 (A). This 27-year-old patient who requested facial contour rejuvenation by autologous fat transplantation is shown in A. She was treated by a total facial fat grafting in the naso-jugal fold, the malar and buccal fat pads, the nasolabial fold, the lips, and the check, three sessions were done, 7 mL per session, a total of 21 mL of both fresh and stored fat were used. (B) The postoperative result is shown 1.5 years after the procedure.

Figure 3 (A) This 23-year-old patient who complained of left hemifacial microsomia, requested reconstruction of the left side of the face is shown in A. She was treated with autogenous fat grafting in the left nasolabial, left check, and the angle of the mandible, three sessions were done, 8 mL per session, a total of 24 mL of both fresh and stored fat were used. (B) The postoperative result is shown 5 years after the procedure.

Figure 4 (A) This 32-year-old patient who requested facial contour rejuvenation by autologous fat transplantation is shown in A. She was treated by autologous fat grafting in the naso-jugal fold, the malar and buccal fat pads, the nasolabial fold, and the check, four sessions were done, 9 mL per session, a total of 36 mL of both fresh and stored fat were used. (B) The postoperative result is shown 4 years after the procedure.
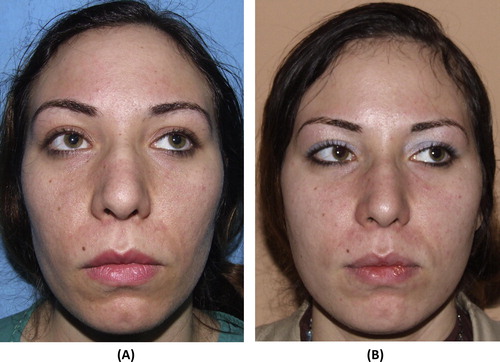
Figure 5 (A) This 29-year-old patient who requested facial contour rejuvenation by autologous fat transplantation and Botox for the forehead is shown in A. She was treated by a facial fat grafting in the naso-jugal fold, the malar and buccal fat pads, the nasolabial fold, and the check, three sessions were done, 7 mL per session, a total of 21 mL of both fresh and stored fat were used. The lips augmentation was done using Juvederm. (B) The postoperative result is shown 1.5 years after the procedure.

Figure 6 (A) This 53-year-old patient who requested facial contour rejuvenation by autologous fat transplantation and Botox for the forehead is shown in A. She was treated by total facial fat grafting in the naso-jugal fold, the malar and buccal fat pads, the nasolabial fold, the outer two third of eye brows and the check, four sessions were done, 12 mL per session, a total of 48 mL of both fresh and stored fat were used. (B) The postoperative result is shown 4 years after the procedure.

Nine transfers (8.65%) did not yield good outcomes. In these cases further injections were done using the cryopreserved fat after re-warming it.
The least favorable results were that of the leg and lip augmentation, shortly after injection less than quarter of the initial volume stayed and most of the injected fat disappeared.
The following complications were observed:
Swelling and edema were the most common complain of most of the patients at the first injection using fresh fat but many surgeons considered edema is not a complication rather than part of the technique.
9 cases of infection were encountered in the study, 4 cases of facial rejuvenation, 4 cases of leg augmentation and one case of hand rejuvenation, and all of them were treated conservatively except 2 cases were drained under local anesthesia.
Seven cases showed formation of multiple tiny firm nodules (like bead chain), which resolved spontaneously after 3 months of watchful expectation.
3 cases of hematoma (2 cases at the infraorbital region and one hematoma at the nasolabial fold), all the three cases respond well to conservative treatment using hot compresses and local heparin cream.
3 cases of traumatic fat necrosis which were proved using the fine needle aspiration cytology, all of them affect the inner aspect of the infraorbital region and the upper part of the nasolabial fold.
4 Discussion
Structural fat grafting is extensively used in plastic surgery. In spite of the great potential of the technique, there is paucity of the scientific studies that document the technique.
For a decade, fat is widely used for both aesthetic and reconstructive purposes, and many plastic surgeons believe that fat is too close to be considered the ideal filler.Citation7
It is readily available and inexpensive; it is autologous and therefore lacks a host immune response; it is safe and non-carcinogenic; and it is easily acquired with a minimally invasive procedure.
Neuber did the first free fat graft in humans. He stressed on the importance of small grafts to have more predictable results.Citation8
In 1950, Peer documented that autologous fat grafts lost approximately 45% of their weight and mass per year, or more, following transplantation in humans.Citation2
Due to the subsequent decrease in graft size after implantation many recommend overcorrection to overcome the loss in filling volume.Citation9
Several studies were done to explain the behavior of the fat graft after injection, and initially graft survival is due to direct diffusion of nutrients from plasma, because of the higher surface of the smaller grafts, as a greater proportion of the graft is in contact with the graft bed. Actual revascularization occurs in the first 48 h post-transplantation. On the other hand large grafts exhibit higher rates of resorption due to liquefaction and cyst formation.Citation2,Citation10,Citation11
These studies support the results of our study, that injecting small amount of fat gives the best durable aesthetic outcomes, due to higher surface area of the fat graft, better contact, less edema and gradual injection ensure better judgment of the patient for the needed augmenting volume.
Gatti recommended a minimum of 3 fat grafting sessions for an appreciable augmentation, but, he used fresh fat for each injection in which the patient was exposed to another operative intervention with extra cost.Citation12
ColemanCitation13 has found that “fat placed stably maintains its shape and consistency over time and has every indication of permanence.” But this is not the rule as shown by many studies.
Whatever the technique is adopted by the plastic surgeon, most surgeons agree that implanting high percentage of viable fat cells improves permanence in fat grafting.
We believe that injecting small amount of fat ensures better survival of the fat cells due to better contact with the plasma, large exposed surface area for the neo-vascularization, all of these will result in excellent long standing and stable aesthetic results.
Conflict of interest
None of the authors has a financial interest in any of the products, devices, or drugs mentioned in this manuscript that might create a conflict of interest with information presented in any part of the submitted manuscript.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
The paper was presented at the 7th IFFPSS Congress “Nose & Face World” in Rome May 9th–12th, 2012, Rome, Italy.
Available online 1 February 2016
References
- S.R.ColemanFacial recontouring with lipostructureClin Plast Surg241997347367
- L.A.PeerLoss of weight and volume in human fat grafts: with postulation of a “cell survival theory”Plast Reconstr Surg51950217
- A.ChajchirFat injection: long-term follow-upAesthetic Plast Surg201996291296
- I.NiechajevO.SevcukLong-term results of fat transplantation: clinical and histologic studiesPlast Reconstr Surg941994496506
- J.L.MikusJ.A.KoufmanS.E.KilpatrickFate of liposuctioned and purified autologous fat injections in the canine vocal foldLaryngoscope10519951722
- J.SmahelExperimental implantation of adipose tissue fragmentsBr J Plast Surg421989207211
- L.H.PereiraB.NicarettaY.C.IllouzClinical applications of autologous fat transplantatY.G.IllouzA.SterodimasAdipose stem cells and regenerative medicine7th ed.2011Springer-VerlagBerlin Heidelberg5765
- F.NeuberFettransplantationChir Kongr Verhandl Dsch Gesellch Chir22189366
- L.PuX.CuiB.F.FinkLong-term preservation of adipose aspirates after conventional lipoplastyAesthetic Surg J2004536541
- D.FagrellS.EnestromA.BerggrenFat cylinder transplantation: an experimental comparative study of three different kinds of fat transplantsPlast Reconstr Surg9819969096
- R.MosconaO.ShoshaniH.LichtigViability of adipose tissue injected and treated by different methods: an experimental study in the ratAnn Plast Surg331994500506
- J.E.GattiPermanent lip augmentation with serial fat graftingAnn Plast Surg421999376380
- S.R.ColemanStructural fat grafts: the ideal filler?Clinic Plast Surg282001111119