
Abstract
The fast of Ramadan is a dilemma for diabetic patients due to the complexity of the management of diabetes during this holy month and the multiple risks they face (hypoglycemia, etc.).
Objectives
Evaluate the impact of a structured protocol of therapeutic education in a sample of type 2 diabetes, who were authorized by their doctors to fast, on metabolic and anthropometric profiles.
Methods
This prospective study was conducted among 54 type 2 diabetic patients (28 men and 26 women) aged 36–65 years, recruited from National Nutrition Institute. Patients were divided into two groups: the first group (n = 26) received an education session one to two weeks before the month of Ramadan; the second group (n = 28) did not have appropriate therapeutic education except therapeutic adjustments. All our diabetic patients benefited from anthropometric measurements, determination of body composition and metabolic assessment (HbA1c, cholesterol, triglycerides, etc.) before and after the month of Ramadan.
Results
The fast was completed without complications in 25 diabetic patients educated group and 22 control patients.
We found that weight loss was greater among educated diabetic patients (−1.05 kg) than in controls (−0.58 kg), but without statistical significance. Body composition has not undergone significant changes in both diabetic groups.
Therapeutic education has led to a decline of 0.27% in HbA1c in the educated group while glycemic control in diabetic patients uneducated remained stable. Furthermore, we observed a better lipid profile in diabetic patients educated than those who did not have education.
Conclusion
Our results justify the interest of patient education centered on the month of Ramadan in all type 2 diabetic patients observing the fast of the holy month. This education should be continued during Ramadan in order to fulfill this religious rite safely.
1 Introduction
Fasting during Ramadan is one of the five pillars of Islam. It is mandatory for all adult Muslims in good health. Diabetic patients who fast are exposed to several risks related on the one hand to the period of fasting and on the other to changes of rhythm and eating habits that characterize the month of Ramadan i.e. the consumption of meals rich in saturated fats and carbohydrates with high glycemic index.Citation1 Despite the ban on the practice of fasting by their doctors, some diabetic patients insist to fast. According to the study “EPIDIAR”Citation2, conducted in 2003 in 13 Islamic countries, 79% of type 2 diabetic patients observe the fast of Ramadan. So in order to prevent or reduce the risk of complications in diabetic patients who fast, recommendations have been drawnCitation1,Citation3,Citation4 and it shows that therapeutic education focused on the month of Ramadan, including dietary adjustments and while insisting on glycemic self-monitoring is crucial. These observations led to carry out this study, whose main objective is to assess the effectiveness of a structured therapeutic education protocol before the month of Ramadan with a sample of type 2 diabetic patients, identified as low or medium risk of complications, which were allowed to fast.
2 Methods
This is a prospective study which involved 54 type 2 diabetic patients, recruited two weeks before Ramadan at the service “ A ” of the Tunis National Institute of Nutrition, which have been authorized by their doctors to fast the month of Ramadan. In 2013, this month took place from July 9 to August 7. All patients were treated with ADO (oral antidiabetics) and had an HbA1c ⩽ 9% (glycosylated hemoglobin). Patients who have experienced severe hypoglycemia in the three months preceding the month of Ramadan or with macrovascular complications including ischemic heart disease, renal impairment and pregnant and lactating women were excluded from the study. The recruited patients were divided into two groups ().
Figure 1 Design of the study.
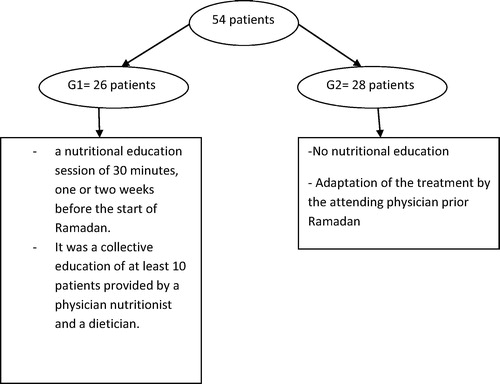
The objective of this education was to enable patients to acquire knowledge and self-care skills to better manage their disease during the month of Ramadan, namely:
| – | Ensure a balanced food intake in both qualitative and quantitative terms (limiting fatty and fried foods and products with high glycemic index). | ||||
| – | Prevent dehydration by ensuring adequate fluid intake during periods of non-fasting. | ||||
| – | Recognize the clinical manifestations of hypoglycemia, hyperglycemia and learn what to do when they occurred. | ||||
| – | Ensure proper therapeutic compliance by following adaptations of treatment established by the physician. | ||||
Emphasize the importance of SMBG, particularly during the period of fasting, for screening hypoglycemia (<0.7 g/l) and hyperglycemia (>3 g/l) which are indications to interrupt fasting.
All patients underwent a search of degenerative complications and anthropometric measures including the calculation of body mass index (BMI) and the measure of fat mass by impedance and a complete lipid and glycemic assessment. These measurements were performed fifteen days to a month before Ramadan (t1) and were done one or two weeks after the end of the holy month (t2). Statistical analyzes were performed using EPI INFO software using the chi-square test (χ2) for the comparison of qualitative variables. As for the comparison of means, it is based on the Student’s t-test or Kruskal–Wallis if the conditions are required. A difference is considered statistically significant if the p value is less than 0.05.
3 Results
The general characteristics of the population are summarized in , and both groups were fair for the different parameters with a p value that was not significant.
Table 1 Sociodemographic, clinical and biological characteristics of the patients.
The impact of patient education on different parameters before and after Ramadan is summarized in .
Table 2 Evolution of clinical and biological parameters before and after Ramadan.
During the month of Ramadan, the average blood glucose levels measured at 11 am were 1.33 ± 0.2 g/l in the educated group and 1.41 ± 0.4 g/l in the control group. The difference was not statistically significant and the mean capillary blood glucose measured two hours after breaking the fast (iftar) in educated diabetics (1.9 ± 0.5 g/l) was comparable to that of non-educated group (2 ± 0.6 g/l).
Among our patients, 47 subjects had fasted the whole month of Ramadan (29 days). Almost all educated diabetics (96%) fasted all the holy month, while 22% of non educated diabetics had interrupted their fast. Educated diabetics fasted for a longer period (28.5 days) than non-educated patients (25.5 days). One patient from each group presented hypoglycemia requiring breaking the fast, but no severe hypoglycemia was reported. One diabetic enjoyed a therapeutic education and two uneducated patients had to break their fast for other reasons such as fatigue and heat. The fasting-related complications occurring are summarized in . The frequency of minor hypoglycemia decreased before and during Ramadan in both groups from 15% to 4% for G1 and 18 to 11% for G2.
Table 3 Different complications made during Ramadan.
4 Discussion
We have not noted an efficiency of our education program on weight, BMI and fat mass which could be explained by the lack of monitoring during the month of Ramadan, changing both quantity and quality of food as well as low level of physical activity. The study READ (Ramadan Education and Awareness in Diabetes)Citation5 which was conducted in England in 2010 with 111 type 2 diabetics treated with ADO showed an average weight loss of 0.7 kg in patients group that received educational support vs 0.6 kg in the control group. The study of SmaouiCitation6and MustafaCitation7 showed a weight gain. The overweight type 2 diabetic patients often tend, as in the general population, to loose a little weight during Ramadan. Indeed, the study of northern AlgeriaCitation8 showed a statistically significant weight loss in diabetic obese patients during Ramadan. The authors of this study noted a resumption of weight a month after Ramadan. A Jordanian studyCitation9 showed an average weight loss of 1.57 kg between the beginning and the end of Ramadan. This weight loss was only significant in overweight patients. In a recent study conducted during Ramadan 2014, the authors found a greater improvement of weight after educational program.Citation10
The decrease in HbA1C may be secondary to the decrease in the number of daily meals, which is accompanied by a reduction in hyperglycemic peaks. In the literature, the results are controversial as to the change in HbA1c. Indeed, a significant decrease was noted by some authorsCitation6–Citation8,Citation10,Citation11 ranging from 0.11% to 1.94%, a stability of HbA1c has been noted by othersCitation12–Citation14 and some have even noted a deterioration in glycemic control.Citation15,Citation16 In diabetic patients, blood glucose variations depend on the quantity and quality of diet, possible excessive consumption during Iftar, the drug compliance and changes in physical activity.
It appears that the therapeutic education centered on Ramadan has a beneficial effect on reducing the risk of hypoglycemia. Our consistent results with the results of the study READCitation5 showed a significant decrease in the number of hypoglycemic episodes from 9 to 5 in the group that received education. The epidemiological study, “Epidemiology of Diabetes and Ramadan” (EPIDIAR), gathering the data from nearly 12,000 patients with diabetes during Ramadan in 13 different countriesCitation2, found an increase in the relative risk of severe hypoglycemia of 7.5 in type 2 diabetics. It should be noted that this study did not take into account the severe hypoglycemia requiring hospitalization and excluded those that required the intervention of a third party without hospitalization as well as nonsevere hypoglycemia. The incidence of these is probably underestimated. In type 2 diabetic patients, increasing the frequency of hypoglycemia during that month is not systematically recovered. The hypoglycemia could be favored by a bad adaptation of hypoglycemic therapy and the jump of meal sehour (the last meal before the beginning of fast and which often occurs early in the morning). The observational study of Uysal et al.Citation16 found an increase in symptomatic hypoglycemia, while other studiesCitation17,Citation18 did not find an increase of hypoglycemia in patients treated with oral antidiabetic agents or insulin. This divergence of results in the risk of hypoglycemia, can be explained by the unfolding of Ramadan in different seasons with a variable duration of the period of daytime fasting. Thus, the risk of hypoglycemia can vary from year to year. In addition, hypoglycemia is more common in diabetics treated with drugs with high hypoglycemic power. Finally, the small number of studies diminishes the power of statistical tests.
As regards the risk of hyperglycemia, EPIDIAR studyCitation2 showed a 5-fold increase in the incidence of episodes of severe hyperglycemia (requiring hospitalization) in patients with type 2 diabetes and a factor of 3 incidence of hyperglycemia episodes with or without ketoacidosis in type 1 diabetes requiring hospitalization. The risk of hyperglycemia is attributed to the reduction of excessive doses of antihyperglycemic drugs (in order to prevent hypoglycemia) and excessive consumption of foods with high glycemic index. As for hypoglycemia, the incidence of non-severe hyperglycemia was not assessed in the study EPIDIAR. McEwenCitation10 found severe hypoglycemic events in the control group who did not receive an individualized education.
It appears from all these results that the practice of fasting of Ramadan by many diabetic patients is not without risk of complications (hypoglycemia, hyperglycemia, etc.). This finding justifies the imperative of therapeutic management of diabetes in Ramadan adapted to allow diabetic patients to fast with the lowest risk of complications.
Changes in lipid parameters were marked by a stability of triglyceride levels in both groups of patients. In the literature, study results are somewhat discordant not to conclude formally the effect of fasting on lipid parameters. Some authors showed improvement to an antiatherogenic profile.Citation7,Citation16 By contrast, some authors found an altered lipid profile in people with type 2 diabetes. Indeed, the study of Khatib and ShafagojCitation9, performed in 44 Jordanians, reported a decrease in triglycerides during Ramadan with a slight increase in LDL cholesterol and total cholesterol. The study of Khaled et al. Citation8 in 80 Algerian women with type 2 diabetes and obesity showed a significant increase of approximately 14% of total cholesterol, 17% of triglycerides and 22% of LDL and a decrease in HDL-cholesterol. A Tunisian studyCitation15 showed no significant differences between total cholesterol and triglycerides before and at the end of Ramadan, while the rate of LDL increased and the rate of HDL declined. These changes disappeared 20 days after the end of fasting. These alterations were attributed to changes in eating habits during the period of Ramadan, and more specifically, to the consumption of meals high in saturated fats.
5 Conclusion
The month of Ramadan is a dilemma for diabetics, who value fast, while avoiding the risk of complications (severe hypoglycemia, hyperglycemia, ketoacidosis, etc.) they may face. These findings justify the interest of a structured therapeutic education program adapted to the month of Ramadan which is characterized by profound changes in lifestyle and eating habits.
The observation of this holy month of fasting is a real challenge for the diabetic himself and his doctor. Therapeutic education should therefore have an important place in the management of recommendations of diabetes during Ramadan in order to complete fasting safely. It should be strengthened among diabetic who choose to fast despite the medical and religious exemptions. Ramadan is a good time to acquire knowledge on diabetes management as well as during this month throughout the year.
Conflict of interest
The authors declare that there are no conflict of interests.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 28 January 2016
References
- M.Al-AroujS.Assaad-KhalilJ.BuseI.FahdilM.FahmyS.HafezRecommendations for management of diabetes during Ramadan: update 2010Diabetes Care338201018951902 [Aug]
- I.SaltiE.BénardB.DetournayM.Bianchi-BiscayC.Le BrigandC.VoinetA population-based study of diabetes and its characteristics during the fasting month of Ramadan in 13 countries: results of the epidemiology of diabetes and Ramadan 1422/2001 (EPIDIAR) studyDiabetes Care2710200423062311 [Oct]
- E.HuiV.BravisM.HassaneinW.HanifR.MalikT.A.ChowdhuryManagement of people with diabetes wanting to fast during RamadanBMJ3402010c3053
- International meeting on diabetes and Ramadan recommendations: edition of the Hassan II Foundation for Scientific and Medical Research on Ramadan 1995.
- V.BravisE.HuiS.SalihS.MeharM.HassaneinD.DevendraRamadan education and awareness in diabetes (READ) programme for Muslims with type 2 diabetes who fast during RamadanDiabet Med J Br Diabet Assoc2732010327331 [Mar]
- N.SmaouiP.BöhmeJ.F.CollinDiabète et Ramadan: représentations et pratiques de santé des patients et des soignants et intérêts de l’éducation thérapeutique du patientDiab Metab3822012A47A48
- H.MustafaT.HashimA.Beshyah SalemTargeted diabetes education and glycemic control during Ramadan fasting: an exploratory studyIbnosina J Med Biomed Sci462012242248
- B.M.KhaledS.BelbraouetEffect of Ramadan fasting on anthropometric parameters and food consumption in 276 type 2 diabetic obese womenInt J Diab Dev Countries29220096268
- F.A.KhatibY.A.ShafagojMetabolic alterations as a result of Ramadan fasting in non-insulin-dependent diabetes mellitus patients in relation to food intakeSaudi Med J2512200418581863
- L.N.McEwenM.IbrahimN.M.AliS.H.Assaad-KhalilH.R.TantawiG.NasrImpact of an individualized type 2 diabetes education program on clinical outcomes during RamadanBMJ Open Diab Res Care312015e000111
- M.MaislosY.Abou-RabiahI.ZuiliImproved diabetes control after prolonged fasting the Ramadan modelPract Diab Int1852001149151
- J.BelkhadirH.el GhomariN.KlöckerA.MikouM.NasciriM.SabriMuslims with non-insulin dependent diabetes fasting during Ramadan: treatment with glibenclamideBMJ30768991993292295
- R.BouguerraA.BelkadhiJ.JabraneJ.HamzaouiC.MaâtkiM.C.Ben RayanaMetabolic effects of the month of Ramadan fasting on type 2 diabetesEast Mediterr Health J Rev Santé Méditerranée Orient Al-Majallah Al-Ṣiḥḥīyah Li-Sharq Al-Mutawassiṭ95–6200310991108
- M.A.LaajamRamadan fasting and non-insulin-dependent diabetes: effect on metabolic controlEast Afr Med J67101990732736
- R.BouguerraJ.JabraneC.MaâtkiL.Ben SalemJ.HamzaouiA.El KadhiRamadan fasting in type 2 diabetes mellitusAnn Endocrinol67120065459
- A.R.UysalM.F.ErdoğanG.SahinN.KamelG.ErdoğanClinical and metabolic effects of fasting in 41 type 2 diabetic patients during RamadanDiab Care2111199820332034
- O.BakinerM.E.ErtorerE.BozkirliN.B.TutuncuN.G.DemiragRepaglinide plus single-dose insulin glargine: a safe regimen for low-risk type 2 diabetic patients who insist on fasting in RamadanActa Diabetol46120096365
- M.CesurD.CorapciogluA.GursoyS.GonenM.OzdumanR.EmralA comparison of glycemic effects of glimepiride, repaglinide, and insulin glargine in type 2 diabetes mellitus during Ramadan fastingDiab Res Clin Pract7522007141147