
Abstract
Introduction
Auricular reconstruction of congenital or acquired ear defects can provide a realistic good-looking ear and functional cephaloauricular sulcus especially for those who wear eyeglasses. Over the past few years, refinements in the techniques of elevating the buried ear framework in the second stage of ear reconstruction have shifted from simple skin grafting to the use of flaps and cartilage blocks for creation of the cephaloauricular sulcus.
Objective
The aim of the study was to describe useful simple modification using bilateral triangular flaps and full thickness skin graft to create adequately functional cephalo-auricular sulcus especially for patients wearing eyeglasses during the second stage ear reconstruction.
The study design
The described technique was carried out between June 2010 and January 2014, for 37 patients (24 patients with congenital microtia grade III, 7 patients with post-burn ear deformity, and 6 patients with post-traumatic ear defects). During the second stage of total ear reconstruction, the ear framework is separated substantially from the side of the head and positioned at the desired angle by means of a block of cartilage covered with a fascial flap. Then, two local triangular flaps from the adjacent non-hairy skin are created (one is superiorly based and the other is inferiorly based) and inset into the created cephaloauricular sulcus. The rest of the post-auricular defect is covered with a full thickness graft.
Results
The technique was simple and effective with no post-operative complication regarding flaps viability. Patients requiring glasses have worn frames soon after the tie-over was removed and no sulcus problems have resulted.
1 Introduction
Total ear reconstruction using autologous cartilage is usually performed in two stages.Citation1–Citation4 Creation of cephalo-auricular sulcus is the hallmark of the second stage, and in this stage every effort should be done to produce good-looking ear, normally positioned with sufficient cephalo-auricular sulcus to allow skin care and wearing eyeglasses.
Figure 5 Oblique view of the same patient nine months after the second stage of ear reconstruction.

Figure 6 Male patient, 46 years old presented with near traumatic total loss of the left ear.

Figure 7 Oblique view of the same patient 8 months after the second stage of ear reconstruction.

Figure 8 Lateral view of the same patients 8 months after the second stage of ear reconstruction.

Figure 9 Female patient, 19 years old presented with third stage microtia of the left ear.

Over the past two decades, the modifications and refinements in ear reconstruction were focused on creating stable elevation of the reconstructed auricle. The technique of elevation has evolved from simple skin graftingCitation5 to the use of pedicled flaps and cartilage blocks.Citation4, Citation6–Citation8
The article presents our clinical experience with a simple and reliable technique for creating a smooth cephalo-auricular sulcus in second stage ear reconstruction.
2 Patients and methods
Between June 2010 and January 2014, the authors performed staged subtotal and total auricular reconstructions, adopting the Nagata technique with modification in the second stage using two triangular skin flaps.
37 patients were included in the study; the patients were 23 males and 14 females. Their ages ranged between 5 and 42 years (mean, 17.22 years) at the time of reconstruction.
Twenty-four (64.86%) cases were grade III microtia (right: 12 cases, left: 8 cases, Bilateral: 4 cases), 7 cases were post-burn deformation, and 6 cases were traumatic amputation of the auricle due to RTA.
The follow-up period ranged from 16 months to 46 months with mean of 36.84 month follow-up.
3 Operative technique
We followed the Nagata principlesCitation1–Citation4 of total ear reconstruction, which are refined by FirminCitation9, SiegertCitation10, and others.Citation11–Citation13
For the first stage, the lobule was transposed by W-M skin incision, the remnant cartilage was removed, and a cartilage framework was fabricated from the ipsilateral 6, 7, 8 and 9 costal cartilages and placed in a subcutaneous pocket.
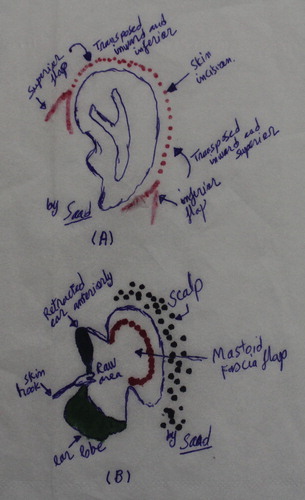
At the second stage, we started the operation by marking of the skin incision half to one cm away from the palpable edge of the cartilage construct, and the incision line was not clear curved line around the construct; instead, we added 2 Y-incision; one at the end (A).
Figure 1 (A) Schematic picture of marking of the triangular skin flaps and skin incision around the reconstructed auricle. (B) Schematic picture of the transposition and the in-sitting of both triangular flaps while retracting the reconstructed auricle.
Local injection of Xylocaine with Adrenaline 1:200,000 was done after marking.
The ear construct was elevated by delicate meticulous dissection just underneath the capsule surrounding the cartilage framework, and the construct was kept elevated by placement of a crescent shaped cartilage block, which was covered with an anteriorly based mastoid fascial flap or a posteriorly based periosteal flap (B).
The bilateral (superior and inferior) triangular flaps were carefully incised and dissected, and these flaps were transposed inward and fixed in place by Vicryl 4/0 to create the beginning of the new cephalo-auricular sulcus and interrupt the continuity of the graft behind the reconstructed auricle ( and ).
Figure 2 Elevation of the reconstructed auricle in 23 years old male patient with grade III microtia of the left ear by delicate meticulous dissection just underneath the capsule surrounding the cartilage framework.

Figure 3 Dissection and transposition of the flap to create the beginning of the new cephalo-auricular sulcus.

The posterior surface of the ear and cephalo-auricular sulcus was covered by a full thickness skin graft (the graft is interrupted by the triangular flap at both ends), and the graft was harvested from the skin just beneath the chest scar that was closed directly after adequate undermining.
4 Results
Thirty-seven patients were treated with the above-mentioned technique. The survival of the triangular flaps was 100%.
Complications were relatively few (13.51%). Two cases of chest seroma, both seromas were treated conservatively by aspiration under complete aseptic technique. Two cases of skin graft losses (one patient was re-grafted 14 days later, and the other one had partial loss of the graft that healed conservatively), and one case of wound dehiscence of the chest wound were due to un-recognized hematoma, which was closed by secondary sutures after draining the hematoma.
Representative cases are shown in –.
Figure 4 Male patient, 23 years old presented with grade III microtia of the left ear.

Figure 10 Oblique view of the same patient 14 months after the second stage of ear reconstruction.

5 Discussion
Optimal aesthetic construction of the auricle is not only constructing a proper framework, but also placing it into the correct natural position.
Besides its correct vertical and sagittal position, normal elevation and inclination are of utmost importance because these define a normal ear from the common anterior view in interpersonal communication (see ).
Figure 11 Lateral view of the same patients 14 months after the second stage of ear reconstruction.

Many techniquesCitation5–Citation8 have been described to create cephalo-auricular sulcus and stabilize the new auricle in an elevated position. Some are simple like split thickness skin grafts, which usually contract leading to blunting of the sulcus and webbing at both ends. OthersCitation14 are bulky pedicled flaps (covered with skin grafts), which frequently end with shallow sulcus.
NagataCitation4 used a costal cartilage block combined with a temporoparietal fascial flap and full-thickness skin graft. But this technique usually leaves visible scalp scar and also sacrifices an important reconstructive tool, the temporoparietal fascial flap, which can be very useful in treating any complication.
The use of fascial flaps to cover the cartilage block, whether innominate fascial flap as described by NagataCitation15, anteriorly based as described by Yoshimura et alCitation6, or posteriorly based combined fascial and periosteal flap as described by Siegert et al.Citation16, provides vascularity to the transplanted framework so that it can accept skin grafts.
The advantages of the fascial flaps are mainly to avoid a scar on the temporal hair-bearing area, and to preserve the superficial temporoparietal fascial flap as a live boat to save the construct in case of complications. Yet, the bulkiness of the flaps and the contraction of the overlying skin graft frequently result in blunting of the cephalo-auricular sulcus.
We have developed a new simple modification in the second stage of total ear reconstruction in which we used in addition the full thickness skin graft, two triangular flaps from the non-Hairy skin to interrupt the continuity of the graft at both ends and reduce the incidence of future contracture which is the main cause of blunting of the cephalo-auricular sulcus in cases of total ear reconstruction. The aim is to interrupt the pulling forces of fibrosis along one direction and keep the sulcus deep and suitable for wearing eyeglasses.
Those triangular flaps are easily and safely harvested, and their viability is guaranteed through their wide bases.
6 Conclusion
The described technique is simple, effective, and reliable method for creation of an adequately functional cephalo-auricular sulcus that can support eyeglasses very soon after the operation.
Funding
None.
Conflict of interest
None of the authors has a financial interest in any of the products, devices, or drugs mentioned in this manuscript that might create a conflict of interest with information presented in any part of the submitted manuscript.
Notes
The idea was presented at the 7th IFFPSS Congress “Nose, Face World” in Rome May 9th–12th, 2012, Rome, Italy.
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 16 March 2016
References
- S.NagataA new method of total reconstruction of the auricle for microtiaPlast Reconstr Surg921993187201
- S.NagataModification of the stages in total reconstruction of the auricle: Part II. Grafting the three-dimensional costal cartilage framework for concha-type microtiaPlast Reconstr Surg931994231242
- S.NagataModification of the stages in total reconstruction of the auricle: Part III. Grafting the three-dimensional costal cartilage framework for small concha-type microtiaPlast Reconstr Surg931994243253
- S.NagataModification of the stages in total reconstruction of the auricle: Part IV. Ear elevation for the constructed auriclePlast Reconstr Surg931994254266
- B.BrentReconstruction of the earJ.W.SmithS.J.AstonGrabb and Smith’s plastic surgery4th ed.1991Little, Brown and CompanyBoston463490
- K.YoshimuraH.AsatoT.NakatsukaElevation of a constructed auricle using the anteriorly based mastoid fascial flapBr J Plast Surg521999530533
- L.F.OuR.S.YanY.W.TangFirm elevation of the auricle in reconstruction of microtia with a retroauricular fascial flap wrapping an autogenous cartilage wedgeBr J Plast Surg542001573580
- P.L.GibelliS.GrappoliniA.VeronesiReconstruction of the retroauricular fold: a personal techniqueBr J Plast Surg542001201204
- E.FirminEar reconstruction in cases of typical microtia. Personal experience based on 352 microtic ear correctionsScand J Plast Reconstr Hand Surg3219983547
- R.SiegertThe combined reconstruction of congenital auricular atresia and severe microtiaLaryngoscope113200320212029
- C.ParkT.J.LeeK.S.ShinA single-stage two-flap method of total ear reconstructionPlast Reconstr Surg881991404412
- C.ParkModification of two-flap method and framework construction for reconstruction of atypical congenital auricular deformitiesPlast Reconstr Surg99199718461857
- K.YoshimuraT.NakatsukaS.IchiokaOne-stage reconstruction of an upper part defect of the auricleAesthetic Plast Surg221998352355
- G.AlexanderN.RajacicM.K.IbrahimThe combined posterior temporoparietal and galeal fascial flap: a new flap in the elevation of the constructed auricleBr J Plast Surg552002582584
- S.NagataSecondary reconstruction for unfavorable microtia results utilizing temporoparietal and innominate fascia flapsPlast Reconstr Surg941994254265
- R.SiegertS.IbrahiemR.MagritzPeriosteal flap technique for elevation of the pinna in microtiaJAMA Facial Plast Surg2015 (July, online first)