
Abstract
46XY complete gonadal dysgenesis (SWYER SYNDROME) is a rare type of Disorder of Sex Development. Herein we report a 15 years-old child, reared as female, presented with complaints of primary amenorrhoea, without short stature or Turner’s stigmata. Secondary sexual development was normal. Biochemically, luteinizing hormone (LH) was 23.29 mIU/ml and follicle stimulating hormone (FSH) was 54.94 mIU/ml. Serum estradiol level was 15.33 pg/ml (21–51), and Testosterone was 14.04 ng/dl. USG abdomen revealed a small uterus with thinned endometrium. MRI Abdomen showed hypoplastic uterus with non-visualized B/L ovaries (? Complete/pure gonadal dysgenesis). Patient had withdrawal bleeding with estrogen progesterone challenge test. Karyotype analysis revealed 46XY with no evidence of mosaicism. Based on these results a diagnosis of Swyer Syndrome (complete gonadal dysgenesis: Disorder of Sexual Development) was suspected. Patient was managed with a multidisciplinary approach and various issues were discussed.
1 Introduction
46XY complete gonadal dysgenesis (SWYER SYNDROME) is a rare type of Disorder of Sex Development (DSD) first described by Gim Swyer in 1955 where a 46-XY subject presents with internal and external female genitalia, normal or little mammary development and primary amenorrhoea, without clinical stigmata for Turner syndrome. It can be sporadic or familial.Citation1 We herein report a case of SWYER SYNDROME.
2 Case report
A 15 years old child, reared as female, born of non-consanguineous marriage, presented to our Out-patient Department with primary amenorrhoea (). The subject had female sexual identity, with normal height and appropriate secondary sexual characters for her age. Past medical, family, and developmental histories were not contributory. General and systemic examinations were within normal limits; the subject had no stigmata of Turner’s syndrome. Breast development was appropriate for age (Tanner stage III).Citation2 External genitalia were normal; there was no evidence of ambiguity. Pubic hair growth was Tanner’s stage III, and axillary hair development was normal. Anthropometric measurements were appropriate for age.
Figure 1 Patient’s social photograph.

3 Investigations
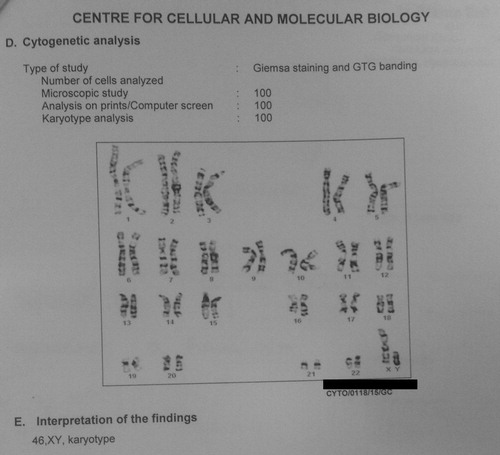
Routine biochemical and haematological investigations were within normal limits. Karyotype analysis revealed 46XY, without mosaicism. A repeat karyotype over 100 cells showed the same result (). Hormonal evaluations were consistent with primary gonadal failure: [TSH 1.59 mIU/L, Prolactin 4.49 ng/dl, LH 23.29 IU/L, FSH 54.94 mIU/ml, Testosterone 14.04 ng/dl, Oestrogen 15.33 pg/ml]. X-ray of both hands suggested a bone-age of 14 years. USG abdomen revealed a small uterus with thinned endometrium. MRI Abdomen revealed a hypoplastic uterus; gonads were not visible bilaterally (Pure gonadal dysgenesis).
Figure 2 Cytogenetic analysis showing 46XY Karyotype.
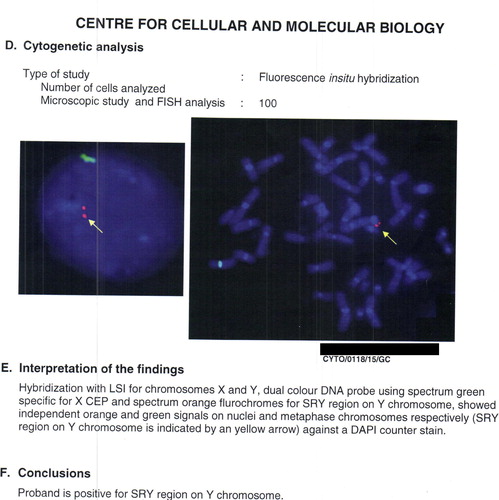
A FISH study revealed that the proband was positive for SRY region on Y-chromosome ().
Figure 3 FISH analysis showing proband positive for SRY region on Y chromosome.
4 Management
At this point, we had a 15-year old phenotypic female subject, with primary amenorrhoea, normal external genitalia and Mullerian structures present on imaging, with spontaneous Tanner stage III.Citation2
The subject failed to bleed to a progesterone challenge. Subsequently, she was started on low-dose continuous oestrogen priming, following which she had breakthrough bleeding. She was then prescribed combination of oestrogens and progestogen to induce cycling bleeding. Diagnosis of DSD was disclosed to the parents with the help of our psychological counsellor. Parents were thoroughly educated and counselled about DSD including Swyer syndrome in accordance with clinical guidelines for the management of disorders of sex development in childhood.Citation3 Multiple counselling sessions were held to slowly alleviate the initial shock and bring about acceptance of the condition. Parents were counselled about the risk of gonadal tumour and were advised gonadectomy but they refused for the same. We are following the subject every 3–6 months in our Out-Patient Department and continue to counsel the parents. They were counselled in detail about future fertility, which might be achieved with donated egg or embryo as she cannot produce eggs.
5 Discussion
This 15-year old normotensive child reared as a girl came with complaints of primary amenorrhoea and on work-up was found to have 46XY DSD. She was positive for a functional SRY region on her Y-chromosome on FISH study.
DSD-s are congenital conditions in which chromosomal, gonadal, and genital sex of the subjects are not coincident.Citation1 According to classification of DSD,Citation1 our patient falls in Class B [Abnormal Gonadal Differentiation (Dysgenetic DSD)]; sub class B.I [46XY complete gonadal dysgenesis (Swyer syndrome)]. The most common condition leading to an XY female is complete androgen insensitivity syndrome (CAIS) and is also the main differential diagnosis. Phenotypically, CAIS presents with normal breast development but minimal pubic and axillary hair. Because AMH is normally secreted by the functional testes, there are no mullerian structures and the vagina is hypoplastic.Citation1 However, our patient had normal mullerian structures, and so CAIS was excluded.
Swyer syndrome is a rare cause of DSD, with incidence of 1:80,000. This syndrome, first described by Swyer in 1955, is caused by an error in sex determination during the course of embryogenesis. Patients with Swyer syndrome present with an incomplete or absent masculinization due to abnormalities in the production of testosterone and Müllerian-inhibiting factor.Citation6
Molecular and genetic abnormalities associated with Swyer syndrome include mutations in the ARX, ATRX, CBX2, DHH, DMRT1, GATA4, MAMLD1, MAP3K1, NR0B1, NR5A1, SOX9, WNT4, WT1, WWOX, SRY, and WNT4 genes. The SRY gene is deleted in approximately 10–15%, and mutated in an additional 10–15%, of patients.Citation4,Citation5 Most patients first seek medical attention in adolescence for primary amenorrhoea and/or the absence of secondary sex characteristics.Citation7 This is consistent in our patient, too, who presented with primary amenorrhoea. Swyer syndrome patients are normal-to-tall, present with small or undeveloped breasts, with normal axillary and pubic hair development. The external genitalia are typical of females. Upper part of the vagina and tubes are normal or reduced, and the uterus is small or rudimentary. The gonads are dysgenetic strips composed of only fibrous tissue; they do not exhibit hormonal function and gametogenesis. The gonads are at high risk for gonadal tumours, which are typically gonadoblastomas and/or dysgerminomas.Citation5,Citation7 Immunohistochemical staining, including octamer binding transcription factor (OCT) 3/4, placental-like alkaline phosphatase (PLAP), β-catenin, alpha-fetoprotein (AFP), and stem cell factor receptor CD117 (c-KIT) helps in predicting the risk of gonadal tumours. OCT 3/4 is the most reliable marker for the risk of malignancy. So consideration of these immunohistochemical markers carefully can prevent unnecessary gonadectomy. Expression of three markers OCT 3/4, PLAP, and CD117 strongly suggests for gonadectomy, even in the absence of overt germ cell malignancy.Citation8
In patients suspected of having Swyer syndrome, laboratory tests for electrolytes, FSH, LH, prolactin, TSH, free T4, SHBG, androstenedione, estradiol, and testosteroneCitation5 help in diagnostic confirmation. In our case, FSH and LH levels were elevated and estradiol levels were low, suggestive of hypergonadotropic hypogonadism, a condition consistent with Swyer syndrome. As a rule, Swyer syndrome patients exhibit low androgen levels and a non-mosaic karyotype of 46XY. In addition, patients can be tested for levels of anti-Müllerian hormone and inhibin, although these tests are not mandatory.Citation4
6 Summary
This case report is relevant as it calls attention to exclude rare DSD like Swyer syndrome in a subject with primary amenorrhoea, as accurate and early diagnosis would allow for conservative treatment and appropriate psychological counselling, which may ensure the preservation of fertility, reduce emotional trauma, and improve patient survival.Citation4
7 Limitation
Parents were asked to allow for the gonadectomy of intra-abdominal gonads with 46XY chromosome with proper counselling, but parents refused for procedure, as they were satisfied after withdrawal bleeding. Estimation of immunohistochemical markers was not done due to cost constraints.
Conflict of interest
Declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
Funding
This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 11 June 2016
References
- A.R.ReyN.JossoDiagnosis and treatment of disorder of sexual development7th ed.L.J.De GrootJ.L.JamesonEndocrinology adult and pediatricvol. 22010Elseviers SaunderPhiladelphia20862118 [chapter 119]
- A.R.RasmussenC.Wohlfahrt-VejeK.Tefre de Renzy-MartinValidity of self-assessment of pubertal maturationPediatrics135120158693
- Consortium on the Management of Disorders of Sex DifferentiationClinical guidelines for the management of disorders of sex development in childhood2006Intersex Society of North AmericaRohnert Park
- T.F.J.KingG.S.ConwaySwyer syndromeCurr Opin Endocrinol Diabetes Obes212014504510
- M.V.N.LipayB.BiancoI.T.N.VerreschiGonadal dysgenesis and tumors: genetic and clinical featuresArq Bras Endocrinol Metabol4920056070 [in Portuguese]
- Rios S.Da SilvaI.C.M.MonteiroL.G.Braz dos SantosA case of Swyer syndrome associated with advanced gonadal dysgerminoma involving long survivalCase Rep Oncol812015179184
- G.Y.MutluH.KırmızıbekmezH.AydınH.CetinerS.MoralıoğluA.C.CelayirPure gonadal dysgenesis (Swyer syndrome) due to microdeletion in the SRY gene: a case reportJ Pediatr Endocrinol Metab282015207210
- B.McCann-CrosbyS.GunnE.O.SmithL.KaravitiM.J.HicksAssociation of immunohistochemical markers with premalignancy in Gonadal DysgenesisInt J Pediatr Endocrinol20151201514