
Abstract
The knee PLC injuries are frequently seen, with other major knee injuries, such as ACL and PCL. Objective: This article aimed to clarify PLC injuries that could be diagnosed by MRI, and may have an impact on the management of the associated major knee injuries. Patient and methods: It was conducted through retrospective MRI revision of 1000 patients who were presented with post-traumatic knee complaints, from January 2011 to March 2016. Results: ITB band injuries were seen in 113 patients (11.3%), biceps tendon injury in 59 patients (5.9%), FCL injuries in 223 patients (22.3%), popliteus muscle injury in 53 patients (5.3%), PFL in 17 (1.7%), arcuate ligament injury in 38 patients (3.8%) and arcuate bone fracture (fibular styloid fracture) in 22 patients (2.2%). Overall PLC injuries recorded 283 patients, either as separate or combined PLC items. Of these 283 patients, 96 patients had associated ACL tear (33.9%), 19 had PCL tear (6.7%), 73 had medial corner injury (25.7%), 55 combined injuries (19.4%) and 40 isolated PLC injuries (14.1%). Conclusion: Different types of PLC injuries may occur in association with other major knee sectorial injuries that may require repair before the associated injured major sector correction, in an attempt to avoid early ACL or PCL graft failure.
Abbreviations:
- ACL
- anterior cruciate ligament
- ITB
- iliotibial band
- Fat Sat.
- fat saturation
- FCL
- fibular collateral ligament
- FFL
- fabellofibular ligament
- Fig.
- figure
- LCL
- lateral collateral ligament
- MCL
- medial collateral ligament
- PACS
- picture achieving and communicating system
- PCL
- posterior cruciate ligament
- PFL
- popliteofibular ligament
- PM
- popliteus muscle
- PLC
- posterolateral corner
- PHLM
- posterior horn of lateral meniscus
1 Introduction
MRI is a merit as a good informative imaging modality for evaluation of a traumatized knee. It has been considered a cornerstone imaging tool for the knee orthopedic practice because of its higher sensitivity and specificity in identification of different knee structures’ injuries. Posterolateral corner (PLC) is a major resistor of rotational and translational stress, particularly in extension. PLC is a multi-compartmental complex sector, formed by the interaction of overlapping multiple structures. Recognition of injuries to these structures is crucial in post-traumatic MR imaging evaluation, as missed uncorrected injuries of this corner - which are not uncommon - can lead to long term debilitating consequences.Citation1,Citation2
Such PLC injuries are usually not isolated and frequently occur in combination with other knee compartments’ injuries, most commonly the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL). ACL and/or PCL reconstruction, without correction of known or missed concomitant PLC injuries, is commonly associated with early graft failure due to persistent unbalanced varus stress over the graft. Understanding the detailed radiological anatomy of the posterolateral corner is crucial for the diagnosis of these troublesome PCL injuries, facilitating appropriate early repair.Citation2,Citation3
The structures forming the PLC are anatomically arranged in three layers. The superficial layer is formed from the iliotibial band (ITB) anteriorly and biceps femoris tendon posteriorly. The intermediate layer is formed of the lateral patellar retinaculum (LPR) and patellofemoral ligament (PFL). The deepest layer consists of the popliteus muscle and its tendon passing through the popliteus hiatus, popliteofibular ligament (PFL), lateral joint capsule, arcuate ligament, fabellofibular ligament (FFL) and FCL (FCL). These PLC stabilizing structures could also be divided into static and dynamic supporting structures. The most important static stabilizers of the posterolateral knee are the FCL, popliteus tendon, and popliteofibular ligament (PFL) ( and ).Citation1, Citation4–Citation7
Figure 1 (A) Anatomic graph of PLC structures, (5) (B) 3D rendering of PLC with the biceps removed demonstrates the Y-shaped arcuate ligament composed of the medial (blue) and lateral (red) limbs attached (green) to the fibular styloid process. FCL, FFL, PFL, and PM are shown.
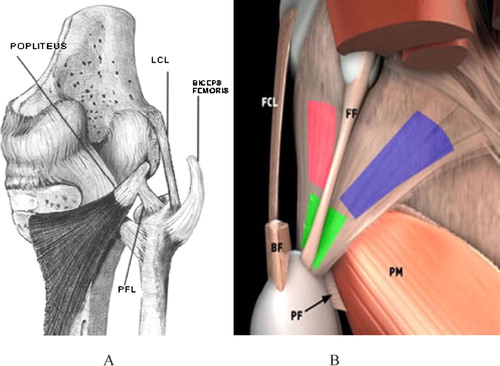
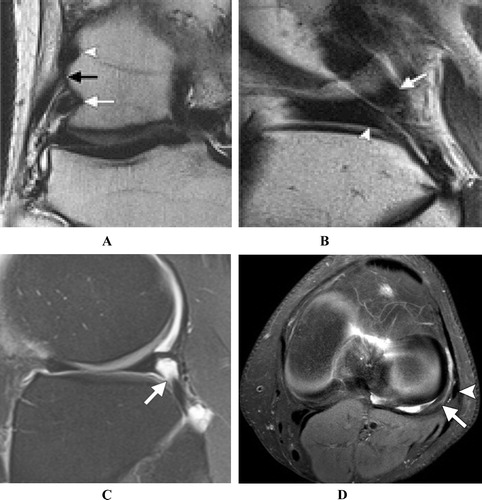
Figure 2 MRI anatomy of knee PLC: (A) Coronal T2-weighted image shows the origin of the lateral gastrocnemius head (arrowhead), femoral attachment of the FCL black arrow), and insertion of the popliteus tendon (white arrow). (B) Sagittal T2-weighted image shows the popliteus tendon (arrow) adjacent to the PHLM (arrowhead) with synovial fluid between them as the popliteus tendon passes through the popliteal hiatus, (C) within popliteomeniscal fascicles (arrow). (D) Axial T2w image: The popliteus tendon (long arrow) posterior to the PHLM, with FCL superficial to it (short arrowhead).Citation4
Injury of these different components of the posterolateral corner can be identified on MRI, as abnormal thickening, interrupted contour and/or abnormal high signal intensity. Thickening and hyperintensity signal changes of FCL, the popliteus muscle, PFL, FFL or the arcuate ligament is defined as a sprain. Tear should be described only when the structure is discontinuous with a visible gap. Some authors recommend the coronal oblique fat saturated sequences to improve the visualization of some of the fine, obliquely oriented structures of PLC, although this has not become routine. Also, one of the important signs of imaging of knee injuries is fracture or edematous marrow signal changes in the related articulating bony surfaces.Citation6,Citation7
2 Subjects and methods
2.1 Objective
The objective of this article was to delineate the different types of posterolateral corner injuries of the knee that may have impact on the management of associated major injuries, such as ACL or PCL tears.
2.2 Patients population
This is a retrospective study, which had been conducted through revision of the PACS achieved knee MRI images of 1000 patients of different age groups that were referred to the radiology department of Al-Mana General Hospital, Eastern Province, Saudi Arabia, with posttraumatic knee injuries, from January 2011 to March 2016 (). The study protocol was approved by the scientific and ethics committee in Al-Mana General Hospital.
Table 1 Age groups of the patients.
2.3 Methods
After careful meticulous revision of these archived knee images, the different types of posterolateral corner injuries, if found, were recorded. For knowing the incidences of these PLK injuries, a percentage of each Item occurrence was estimated (). All examinations were conducted through MRI Philips Intera 1.5 T, Closed Magnet, Philips Medical Systems, 5656 AE Eindhoven, the Netherlands.
Table 2 Incidence of the different types of PLC structure injuries.
3 Results
Revisions of the study candidates’ knee images revealed different combination of PLC items injuries of the study candidates, in association with other major knee structures injuries (ACL, PCL and Menisci). These PLC injured items were recorded separately as follows: ITB band injuries in 113 patients (11.3%), biceps tendon injury in 59 patients (5.9%), FCL injuries in 223 patients (22.3%), popliteus muscle injury in 53 patients (5.3%), PFL in 17 (1.7%), arcuate ligament injury in 38 patients (3.8%) and arcuate bony fracture (fibular styloid fracture) in 22 patients (2.2%). Overall PLC injuries recorded 283 patients (28.3%), either as separate or combined PLC items. Of these 283 patients, 96 (33.9%) patients had associated ACL tear, 19 (6.7%) had PCL tear, 73 (25.7%) had medial corner tear, 55(19.4%) combined injuries and 40 (14.1%) isolated PLC injuries .
Table 3 Incidence of associated other major compartmental injuries with PLC injury.
4 Discussion
The different knee PLC structures’ injuries are not uncommonly seen, in association with other knee sector injuries. We have revised and expressed the different types of knee PLC injuries in detail, in an attempt to clarify these subtle regional injuries that may affect the management and squeal of other knee major injuries correction, if they were missed in preoperative MRI reports.
4.1 ITB injuries
ITB injuries are infrequent injuries that may occasionally be seen in association with other knee sector injuries; the incidence in this study was 11.3%. The ITB is a continuation of the fascia lata, located at the anterolateral aspect of the knee joint and attached to the anterolateral aspect of the proximal tibia. It is considered one of the lateral stabilizing factors of the knee joint. Regardless, it is not truly posterolateral corner structure, but its isolated injury is extremely rare and usually occurs as a continuation of PLC structures’ injuries. As in all tendinous injuries, ITB injury is classified into three grades: grade I: peritendinous edema with normal ITB girth, grade II: focal or diffuse band thickening and grade III: interrupted or avulsed band. Its role in the lateral knee stability compels identification and correction of its injury which may associate with another major knee structural injury (e.g. ACL) .Citation8,Citation9
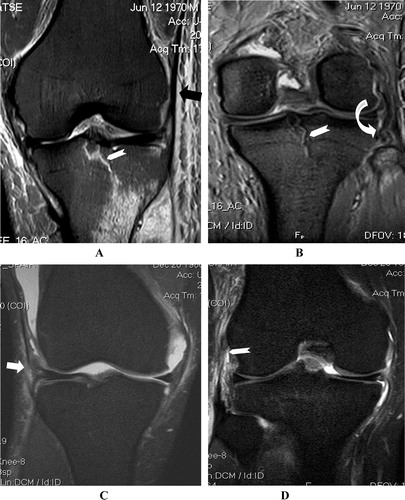
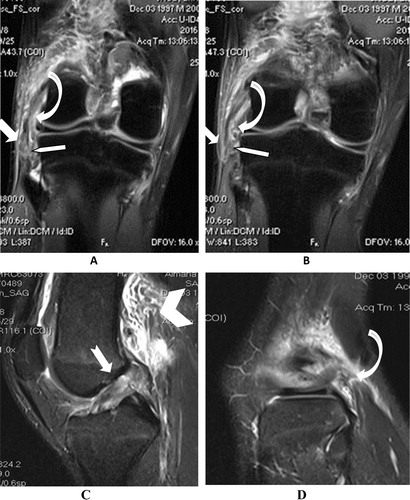
Figure 3 Coronal STIR images showing: (A & B) ITB grade I injury with peri-ligamentous soft tissue edema (Arrow) and intra-articular tibial plateau fracture (Chevron), in association with FCL tear (Curved arrow). (C & D) Another patient with ITB tear (Arrow) associating FCL tear (Chevron).
4.2 Biceps femoris tendon tears
Biceps femoris tendon tear was recorded in 5.9% of the candidates. Both heads of the biceps femoris muscle join just above the knee and then unite with FCL to form a conjoined tendon which inserts onto the fibular head, anterior and distal to the tip of the fibular styloid process. On MRI, the tendon is normally seen as a cord-like structure with low MRI signal intensity, in all pulse sequences. The biceps femoris muscle is the most common injured muscle from the hamstring group, which consists of biceps femoris, semitendinosus and semimembranosus muscles. These muscles are used to flex the knee and extend the hip. Biceps injuries commonly occur secondary to accelerating and decelerating overactivities. Injuries could occur at the myotendinous junction above the knee or at the middle of the tendon, or as avulsion from the fibular head, with or without bony fragments. Biceps tendon injuries are best shown on long TR fat saturation images. As usual in myotendinous injuries, biceps femoris injuries could be classified into three degrees .Citation9,Citation10
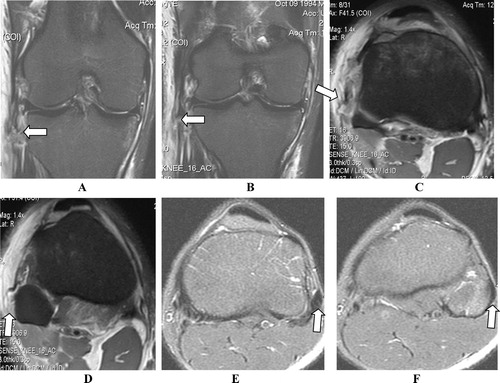
Figure 4 (A & B) Coronal STIR images, (C & D) Axial PD Fat Sat. images, showing aggressive PLC trauma, with avulsed conjoined tendon (biceps and FCL) tear. (E & F) Comparative normal knee: Consecutive axial fat-sat FSE T2 images show normal appearance of the distal bicep tendon joined with FCL to form conjoined tendon, which inserts on lateral aspect of fibular head (Arrows).Citation9
4.3 FCL injuries
FCL injuries are the most common posterolateral corner injuries that were encountered in the study (22.3%). FCL is another extracapsular cord-like structure with no meniscus attachment, as it is located lateral to popliteus tendon. It descends from its proximal attachment at the external tuberosity of the lateral femoral condyle to a level just above the fibular head, where it merges with the posteriorly located biceps tendon to be inserted as a conjoined tendon into the anterolateral aspect of fibular head. This gives the characteristic V-shaped tendinous configuration, in sagittal MRI images, representing the conjoined tendon fibular insertion, which is just anteriorly located to the styloid process.Citation3,Citation4
FCL injury could be clearly diagnosed on coronal and sagittal fat saturation sequences and to some extent in axial T2-weighted images, especially if there is complete tear. FCL injuries could vary from just ligamentous sprain to partial or complete tear. Tendinous sprains are usually seen as localized or diffuse ligamentous thickening, sometimes with T2w hyperintense signal, commonly with periligamentous edema. The FCL is a major knee posterolateral corner stabilizing structure, as it is the primary restraint to varus rotation from 0° to 30° of knee flexion. Consequently, it also helps to resist internal rotational forces of the tibia. FCL tears are subclassified - as all tendinous injuries - into three grades: grade 1: sprain, grade 2: partial or intrasubstance tears and grade 3: complete tear or avulsion. Management of grades 1 and 2 is usually conservative through rest, analgesics and knee immobilizer braces, while grade 3 requires surgical repair to restore stabilizing function of FCL –.Citation10–Citation13
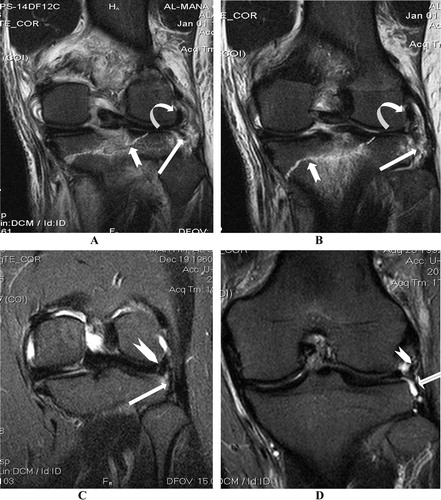
Figure 5 (A & B) Coronal PD-FS (C & D) Sagittal PD-FS images showing torn FCL (Arrow), torn popliteus muscle tendon (Curved arrow), lacerated FPL (Pentagon in A & B) and ACL tear (Notched arrow), together with expected capsular injury seen as extraarticular extravasated synovium (Chevrons).
4.4 Popliteus muscle injury
The popliteus muscle injury was detected in 53 (5.3%) of these study candidates. Popliteus muscle is one of the major static and dynamic stabilizing structures of the knee PLC. It has a tendinous origin from the lateral surface of the lateral femoral condyle (anterior and inferior to FCL attachment) and has a weaker support from the fibular head (PFL). An additional more slender support from the lateral meniscus could be seen in a small percentage of patients. The popliteus tendon courses deeper to FCL and descends into the popliteus hiatus, then passes under the arcuate ligament to have a short extraarticular component before joining the muscle belly. It has a broad fan like insertion on the posterior surface of the tibia above the popliteal (soleal) line.Citation14
Its primary function is internal rotation of the tibia on the femur in the non-weight-bearing status, as well as external rotation of the femur on the leg in the weight-bearing status. It helps with posterior stability of the knee in preventing posterior translation of the tibia on the femur and prevents excessive external and varus rotation of the tibia during knee flexion. Injuries of the popliteus are infrequent and rarely isolated (less than 10%). They usually occur as part of a PLC injury, frequently associated with injury of the ACL or PCL. Being one of the main lateral stabilizing structures of the knee PLC, it is important not to overlook popliteus muscle injury in the presence of an ACL or PCL injury, as the reconstructed cruciate ligament will likely show rapid graft failure without its repair. Also, unrepaired popliteus injuries can lead to severe knee disability due to instability and early meniscus degeneration.Citation15,Citation16
MRI of popliteus injuries may show different stages, according to the level and grade of its damage. It may appear as an avulsion of the popliteus tendon from its femoral attachment, or as an irregular contour of the tendon at the popliteal hiatus, or as swelling and high-signal-intensity changes within the popliteus muscle belly. A complete popliteus tendon tear may be seen as an interruption and possibly a retraction of the muscle belly, which may look like periarticular soft tissue swelling surrounded by fluid. The majority of popliteus tears were involving the muscular or myotendinous portion; in this study 33/38: 86.8%, while only five cases had femoral tendon avulsion. All cases were seen in association with ACL or, less commonly, PCL tear and .Citation4,Citation15,Citation16
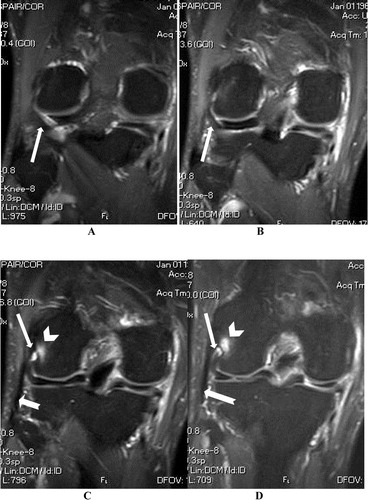
Figure 6 (A–D) Coronal STIR images from posterior to anterior showing partially avulsed popliteal tendon (Arrows) form its femoral attachment, which shows localized marrow edema (Chevrons), with normal FCL (Notched Arrows).
4.5 Popliteofibular ligament (PFL)
PFL tears are usually seen in combination with other PLC components’ injuries, while its isolated injuries are quiet rare. PFL is a short cord like structure, which extends from popliteus musculotendinous junction to the fibular styloid process. This ligament plays an important role in maintenance of the knee posterolateral corner static stability. When present, it is usually seen in T1w and T2w sequences as a hypointense linear structure. However, it is not a constant anatomical structure, and sometimes it could be developmentally missing. It is better visualized in oblique coronal images that can show injury of PFL as increased signal within the ligament, discontinuity, or avulsion of the fibular styloid process, as seen in 17 (1.7%) cases of this study and .Citation16–Citation18
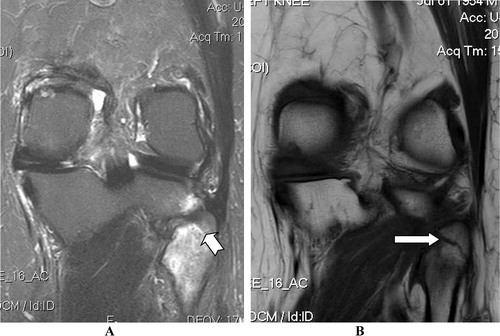
Figure 7 STIR images showing: (A&B) Torn fibular attachment of PFL in RTA patient (Arrows), with intact its popliteus attachment (Curved arrow) and fractured tibial plateau (Notched arrow), in comparison with another normal knee (C & D) which shows intact PFL (Arrows) joining the popliteus tendon (Chevrons).
4.6 The arcuate ligament
It is a Y-shaped thickening of the posterolateral joint capsule, attached distally to the fibular styloid process just anterior to the fabellofibular ligament. It is not constantly present; however, it was reported to be seen only in 50% of normal human beings. It has two limbs, the lateral limb extends superiorly along the joint capsule to the lateral femoral condyle, and the medial limb extends superomedially, over the popliteus muscle to join with the oblique popliteal ligament. It could be visualized as a Y-shaped linear hypointense capsular thickening on sagittal MRI, above the popliteal hiatus. Also, it could be seen on axial images as a low-signal linear structure at the posterolateral joint capsule, at the joint line of the tibiofemoral articulation. Disruption of this ligament (3.8% in the study) could be seen as localized posterolateral capsular distortion and loss of linear continuity at its assumed location. Its disruption is expected to be associated with extraarticular synovial fluid extravasation, seen in para-articular soft tissues .Citation19,Citation20
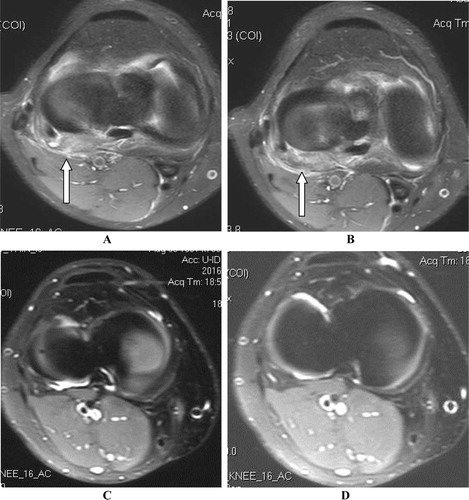
Figure 8 (A & B) axial PD Fat Sat images showing torn arcuate ligament and interrupted PLC joint capsule (Arrows) with posterolateral peri-articular soft tissue edema and lack of joint fluid due to extravasation. (C & D) Another knee showing intact arcuate ligament bordering the joint fluid (Arrows).
4.7 Fibular styloid process fracture
It has been detected in 2.2% of cases, as an avulsed fracture at the attachment site of PFL, FFL, and arcuate ligament. This fracture could be missed by MRI, especially if it is not displaced; hence, the importance of doing complementary X ray or, sometimes, CT scan images to be done along guides with the MRI findings, in traumatized patients. MRI is the only imaging modality, which can diagnose bone marrow contusion, which could be clearly diagnosed in MRI fat saturation fluid-sensitive sequences, e.g. STIR sequence. The bone injury is generally expected to occur secondary to a traumatic hyperextension varus knee stress .Citation21
Figure 9 (A) Coronal STIR image showing severe upper fibular marrow edema (Notched arrow). (B) Coronal T1w image of the same patient showing fractured fibular styloid process (Arrow).
5 Conclusion
| • | PLC injuries occur usually in association with other major knee injuries…e.g. ACL or PCL. | ||||
| • | PLC structures are important stabilizing parts that require repair before ACL or PCL injury repair. | ||||
| • | Different types of PLC injuries could be encountered in practice, and could be trustfully diagnosed with careful MRI revision. | ||||
| • | Missing of these subtle structural injuries in preoperative MRI report, will lead to unopposed stress on the ACL or PCL grafts significantly shortening its half life. | ||||
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 23 September 2016
References
- H.DaviesA.UnwinP.AichrothThe posterolateral corner of the knee: anatomy, biomechanics, and management of injuriesInjury3520046875
- C.D.HarnerT.M.VogrinJ.HoherC.B.MaS.L.WooBiomechanical analysis of a posterior cruciate ligament reconstruction: deficiency of the posterolateral structures as a cause of graft failureAm J Sports Med2820003239
- B.CrespoE.W.JamesL.MetsavahtbR.LaPradeInjuries to posterolateral corner of the knee: a comprehensive review from anatomy to surgical treatmentRev Bras Ortopedia5042015363370 (English Edition)
- S.JadhavS.MoreR.RiascosD.LemosL.SwischukComprehensive review of the anatomy, function, and imaging of the popliteus and associated pathologic conditionsRadiographics3422014496513
- A.AllenV.LopezAcute repair of the posterolateral structures of the knee results in superior clinical methods of reconstructionR.WilliamsD.JohnsonControversies in Knee Surgery2004Oxford University PressNew York255256
- C.P.HelitoM.K.Demange the kneeM.B.BonadioL.E.P.TíricoR.G.GobbiJ.R.PécoraAnatomy and histology of anterolateral ligamentOrthop J Sports Med17201316
- O.RaheemJ.PhilpottW.RyanM.O’BrienAnatomical variations in the anatomy of the posterolateral corner of the kneeKnee Surg Sports Traumatol Arthrosc1572007895900
- R.MansourP.YoongD.McKeanJ.TehThe iliotibial band in acute knee trauma: patterns of injury on MR imagingSkeletal Radiol4320141369137510.1007/s00256-014-1918-2
- A.H.HaimsM.J.MedveckyR.PavlovichJrKatz LD.MR imaging of the anatomy of and injuries to the lateral and posterolateral aspects of the kneeAJR Am J Roentgenol18032003647653
- M.BonadioC.HelitoL.GuryM.DemangeJ.PécoraF.AngeliniCorrelation between magnetic resonance imaging and physical exam in assessment of injuries to posterolateral corner of the kneeActa Ortop Bras223201412412610.1590/1413-78522014220300928
- N.BologJ.HodlerMR imaging of the posterolateral corner of the kneeSkeletal Radiol3682007 Aug715728
- R.F.LaPradeT.V.LyF.A.WentorfL.EngebretsenThe posterolateral attachments of the knee: a qualitative and quantitative morphologic analysis of the fibular collateral ligament, popliteus tendon, popliteofibular ligament, and lateral gastrocnemius tendonAm J Sports Med.3162003854860
- T.HashSports healthMag Resonance Imaging Knee5120137810710.1177/1941738112468416
- R.LasmarA.MarquesJ.SerbinoR.MotaA.HernandezImportance of the different posterolateral knee static stabilizers: a biomechanical studyClinics6542010433440
- R.F.LapradeS.JohansenJ.AgeM.RisbergH.MoksnesL.EngebretsenOutcomes of an anatomic posterolateral knee reconstructionJ Bone Joint Surg Am9220101622
- Jump up to: a bR.F.LaPradeJ.K.WozniczkaM.P.StellmakerC.A.WijdicksAnalysis of the static function of the popliteus tendon and evaluation of an anatomic reconstruction: the “fifth ligament” of the kneeAm J Sports Med3832010543549
- F.D.WadiaM.PimpleS.M.GajjarA.D.NarvekarAn anatomic study of the popliteofibular ligamentInt Orthop272003172174
- R.F.LaPradeT.J.GilbertT.S.BollomF.WentorfG.ChaljubThe MRI appearance of individual structures of the posterolateral kneeAm J Sports Med282000191199
- M.MunshiM.L.PretterklieberS.KwakG.E.AntonioD.J.TrudellD.ResnickMR imaging, MR arthrography, and specimen correlation of the posterolateral corner of the knee: an anatomic studyAJR180200310951101
- A.DiamantopoulosA.TokisM.TzurbakisI.PatsopoulosA.GeorgoulisThe posterolateral corner of the knee: evaluation under microsurgical dissectionArthroscopy212005826833
- G.-S.HuangJ.S.YuM.MunshiAvulsion fracture of the head of the fibula (the arcuate sign): MR imaging findings predictive of injuries to the posterolateral ligaments and posterior cruciate ligamentAJR1802003381387