
Abstract
Objective
To compare ElShatby University Maternity Hospital and Dar Ismail Public Hospital in regard to antenatal, natal, and postnatal morbidity and the causes of maternal mortality.
Methods
A cross-sectional survey was conducted to study females who gave birth in each of the hospitals. Then, a prospective survey of the women was conducted until the 42nd day after delivery. Data were gathered from women who delivered in addition to their caring obstetricians as well as reviewing their medical records. Additionally, records of maternal mortality were reviewed. All females who gave birth between January and April 2014 (3 months) were included in the study.
Results
Two hundred and eighty females participated in the study (130 from ElShatby University Maternity Hospital and 150 from Dar Ismail Public Hospital). Significantly more rural women (29.2%) gave birth at ElShatby University Hospital than at Dar Ismail Public Hospital (16.7%), p = 0.012. More than half of all the study participants (51.8%) suffered from anemia during pregnancy. A minority (5%) of the women were diagnosed with preeclampsia, all of whom gave birth at ElShatby Hospital. Caesarean section rate was significantly higher among women delivered at ElShatby University Hospital compared to Dar Ismail Hospital (61.5% versus 41.3%, p < 001). Only 8.2% of all women needed ICU admission at ElShatby Hospital. The most common cause of maternal mortality was eclampsia, which accounted for 75% of deceased women.
Conclusion
Future studies are needed to identify and understand better the avoidable factors contributing to the relatively high rates of maternal morbidity and mortality in public hospitals. Such information will be of significant use in the processes related to providing quality services, ensuring accessibility of those services, and allocating corresponding resources aimed at reducing maternal morbidity and mortality.
1 Introduction
Despite women living longer than men, their lives are not necessarily healthy.Citation1 Pregnancy and childbirth are conditions that impact only women and may contribute to continued ill-health.Citation2 The health of women during pregnancy and/or childbirth further impacts the health and development of the next generation and the well-being of the family, both economically and socially.Citation3 However, it may be correctly assumed that attendant skilled birth personnel and corresponding supportive emergency obstetric care will reduce health risks during pregnancy and childbirth.Citation1
According to the World Health Organization, maternal morbidity is defined as any condition that is recognized to or aggravated by pregnancy and child delivery that has an adverse impact on women’s wellbeing.Citation4 Maternal mortality is defined by WHO as “Death of a woman while pregnant or within 42 days of end of pregnancy, irrespective of the length and site of the delivery, from any reason related to or aggravated by pregnancy or its management, but not from accidental or incidental causes”.Citation5
Based on the 2005 global burden of disease estimates, maternal conditions were second only to HIV/AIDS in terms of women's deaths worldwide and third in terms of disability-adjusted life-years (DALYs) for women aged 15–44 years. More specifically, maternal conditions contributed to 2.7% of deaths among women worldwide, with 12% of deaths among women aged 15–44 years.Citation2 Now, in the 21st century, approximately 60,000 women die of pregnancy-related causes each year, with the majority of these occurring in developing countries.Citation6
The causes of direct maternal death are mainly postpartum hemorrhage and hypertensive disorder, followed by sepsis, obstructed labor, and ruptured uterus. Last but not the least causes of maternal death are antepartum hemorrhage, abortion, and ectopic pregnancy. The causes of indirect maternal death range from cardiovascular diseases, anemia, and diabetes to infectious and parasitic diseases.Citation7
A decline in maternal deaths requires improving asepsis, fluid management, and blood transfusion, Furthermore, there is a need for better prenatal care. Several tools can be used to reduce maternal mortality. There is a need for increased funding and improved access to health care, to family planning services, to emergency obstetric care, and to intrapartum care.Citation8 Reduction in unnecessary obstetric surgery is another major goal.Citation9
2 Methods
A cross-sectional survey was conducted to study women who gave birth at ElShatby University Maternity Hospital and at Dar Ismail Public Hospital, followed by a prospective survey of those women in both hospitals up to the 42nd day after their delivery. Records were reviewed for maternal mortality at the Director of Health Affairs of Alexandria. All women who gave birth between January and April 2014 (3 months) were included in the study. We are comparing two systems of health care in Egypt with two separate funds from the government; the first is the university funds which is directed mainly for teaching and the other fund comes from the Ministry of health fund which is directed to give medical service for free to the whole population and it is represented by Dar Ismail hospital. Also, we believe that type of hospital is a superior measure for the study questionnaire at hand particularly in Egypt where designation of the type of hospital care may reflect physician experience and service provided. ElShatby University Hospital is a tertiary hospital receives more morbid pregnant women who needed more care and intervention. Also, ElShatby Hospital received all of the women who needed ICU care, not only those women from other facilities but also those from Dar Ismail Public Hospital because its ICU was not functioning. On the other hand, Dar Ismail Public Hospital is a secondary hospital funded by the ministry of health to treat women free of charge.
Several research tools were used for data collection from the women. First, interview questionnaire to all the study participants was used to collect information regarding socio-demographic background, antenatal morbidity, and care received. Data in reference to the nature of the delivery and patient care received also were collected from the physician attending each delivery. Second, data related to postnatal morbidity and care received were collected through weekly phone inquiry with the women from both hospitals until the 42nd day after delivery.
Lastly, transfer sheet was used to transfer data concerning maternal mortality from records kept at the Director of Health Affairs of Alexandria during the period of the study.
3 Statistical methodology
Data were collected, coded, and then entered into an IBM compatible computer, using SPSS (Statistical Package of the Social Sciences), version 18 for Windows. Data were checked for accuracy and then for normality, using Kolmogrov-Smimov & Sharpiro-Wilk tests. Discrete variables were expressed as numbers and percentages, while continuous variables were expressed as means and standard deviations. Unpaired independent samples t-test was used as a parametric test of significance for comparison between two sample means, Chi-square (X2) test was used for paired comparison of dichotomous variables and Fisher’s exact test was used when appropriate. The statistical tests were considered significant if P-value was < 0.05.
4 Results
The study participants were 280 women (130 delivered at ElShatby University hospital and 150 delivered at Dar Ismail Public Hospital) with a response rate 95.3%. shows that the mean age of the participants was 27.09 ± 5.723 years. Women who delivered at ElShatby University Hospital were significantly older than their counterparts at Dar Ismail Public Hospital (29.5 ± 6.096 versus 26.02 ± 4.769 years, p = 0.012). Despite that, a higher percentage of those who delivered at ElShatby University Hospital (7.7%) were young (15 to <20 years) compared to 6.7% of those delivered in Dar Ismail Public Hospital. Significantly more rural women (29.2%) gave birth at ElShatby University Hospital than at Dar Ismail Public Hospital (16.7%), p = 0.012. Consanguinity was significantly more encountered in women who delivered at ElShatby (26.2%) than in their counterparts at Dar Ismail Public Hospital (16%) p = 0.037. shows that 15.7% of the participants suffered from hypertension during their antenatal period, with a significant higher percentage of ElShatby women at 27.7% compared to5.3% of Dar Ismail women where p < 0.001. Only 3.6% of all the study participants suffered from gestational diabetes during the antenatal period, with a higher rate in ElShatby University Hospital participants (5.4%) than in Dar Ismail women (2%), but the difference was not significant. More than one- half of the women (51.8%) suffered from anemia during antenatal period, with insignificant difference between the two hospitals. About one-sixth of the women suffered from urinary tract infections (UTI) during antenatal period. A significantly higher percentage of ElShatby University Hospital women suffered from prenatal UTI than did their counterparts (21.5% versus 12%) where p = 0.032. Antepartum hemorrhage (APH) occurred in only 4% of the women. The rate of APH among women who delivered at ElShatby University Hospital was three times greater than for the women who delivered at Dar Ismail Public Hospital (OR = 3), with insignificant difference between the two hospitals. Five percent of the women were diagnosed as preeclampsia; all of whom were at ElShatby University Hospital. Only two women had a history of blood transfusion. Three women had a history of ICU admission during their pregnancy. All of these women gave birth at ElShatby University Hospital.
Fig. 1 Distribution of delivered women at El Shatby and Dar Ismail hospital according to their antenatal morbidity.
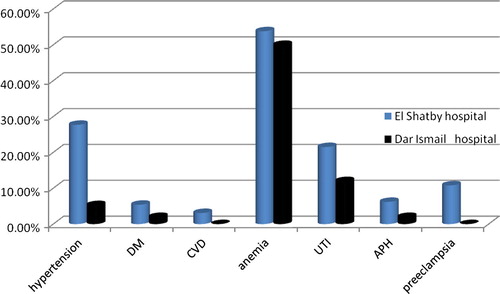
Table 1 The distribution of delivered women at El Shatby and Dar Ismail hospitals by socio-demographic characteristics
As shown in , the rate of normal delivery compared to caesarean section (CS) for the women in this study was nearly equal (49.3% and 50.7% respectively). A significantly higher percentage of CS occurred at ElShatby University Hospital compared to Dar Ismail Public Hospital (61.5% and 41.3% respectively). In regard to outcome of delivery, still births accounted for 8% of total deliveries. Only 8.2% of all women in the study needed ICU admission after delivery, and all of them gave birth at ElShatby Hospital. More than one third of the women (37.9%) received immediate postnatal health education. A significantly higher percentage of women delivering at Dar Ismail received health education than did their counterparts (55.3% versus 17.7%, p < 0.001. Less than half of the women (43.2%) started breast feeding within 6 hours after delivery. More than one third of them (37.8%) started breast feeding after 6 hours of delivery. Women who delivered at Dar Ismail breast fed their babies within 6 hours from delivery more significantly than did those who delivered at ElShatby Hospital where p < 0.001.
Table 2 The distribution of delivered women at El Shatby and Dar Ismail hospital according to their morbidity and care during their natal period.
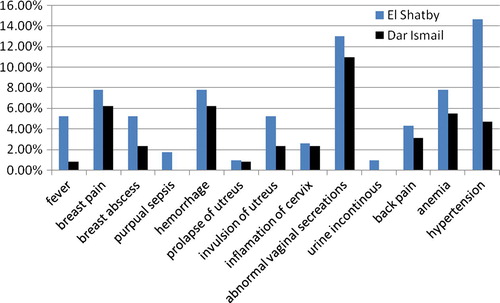
shows that the most common postnatal morbidity in the study participants were abnormal vaginal secretions, breast pain, postpartum hemorrhage, anemia, and breast abscess (12%, 6.9%, 6.9%, 6.6% and 3.7% respectively). Almost one-tenth of the women (9.5%) displayed hypertension in the postnatal period, with a higher percentage at ElShatby University Hospital than at Dar Ismail Hospital (14.7% versus 4.7%. Only 2.9% of the women complained of postnatal fever, with a significant higher percentage at ElShatby University Hospital than at Dar Ismail Public Hospital (5.2% versus 0.8%). In the postnatal period only two women suffered from puerperal sepsis.
Fig. 2 Distribution of delivered women at El Shatby and Dar Ismail according to their post natal morbidity.
As regard the causes of maternal mortality, six women out of eight died from eclampsia, one woman died from ectopic pregnancy, and one woman died from postpartum hemorrhage. All eight women died at ElShatby University Hospital.
5 Discussion
The current study revealed that ElShatby University Hospital received more pregnant women coming from a rural area than did Dar Ismail Public Hospital (29.2% versus 16.7%) with a significant difference. This can be explained by the fact that ElShatby University Hospital as a tertiary hospital receives more morbid pregnant women who needed more care and intervention. Also, ElShatby Hospital received all of the women who needed ICU care, not only those women from other facilities but also those from Dar Ismail Public Hospital because its ICU was not functioning.
In the present study, the mean age of the women was 27.09 ± 5.72 years. This nearly coincides with the mean age of child bearing in Egypt (27.8 years) and in Middle East regions, as recorded by the United Nations in 2011.Citation10
In the WHO systematic review of 2004, the maternal morbidities most frequently reported were hypertensive disorders of pregnancy (14.9%).Citation11 The present study found that hypertensive disorders accounted for 15.7%, which matches the figure in the WHO systemic review. There were a significantly higher percentage of hypertensive disorders in ElShatby University Hospital women than at Dar Ismail public Hospital (27.7% and 5.3% respectively). There is a high incidence of hypertensive disorders in Egypt, which may be due to poor dietary habits, a lack of exercise, and more stressful conditions during pregnancy. The present study also found that preeclampsia was present in about 5% of the women, all of whom were admitted to ElShatby Hospital, a facility which regularly receives high risk cases since it is a well-equipped tertiary university training hospital.
The main maternal morbidity in this study was anemia that was present in about half of the women (51.8%) in both hospitals with no significant difference. In relation to the WHO systemic review which states that anemia in pregnancy shouldn‘t exceed 4.5%, the results of this study show very high rates of anemia. Perhaps, the causes are the high prevalence of schistosomiasis, high rate of hepatic diseases, high number of parity, short interval between pregnancies, and poor dietary habits, especially in rural areas of Egypt. Regardless, the high anemia figure coincides with what WHO reported that 35% to 75% (56% on average) of pregnant women in developing countries and 18% of women from industrialized countries are anemic.Citation12
In terms of the current study, the second most common morbidity was urinary tract infection (UTI), which was present in about one-sixth of the women (16.4%) that was much higher than the WHO systemic review maximum figure of 1.1%. The rate of UTI in El Shatby University Hospital women was higher than in Dar Ismail Public Hospital women (21.5% versus 12%) with a significant difference. Urinary tract infection was higher in other studies conducted in Egypt (1985, 1992 and 1987) which revealed that UTI ranged between (22–28.8%).Citation13–Citation15 UTI was also higher in the Al Haddad study (30%) conducted in Yemen in 2005,Citation16 as well as in the Sheikh study (28.5%) conducted in Pakistan in 2000.Citation17 These high numbers magnify the size of the problem which necessitates a rapid solution, particularly because UTI is related to different adverse outcomes of pregnancy.
The results of this study are similar to those of a study done in 2009 by Abo El MaattyCitation18 who compared maternal mortality and morbidity between ElShatby University Hospital and Gamal Abd El Nasser Hospital, a health insurance hospital. That comparison showed that antepartum hemorrhage (APH) in ElShatby women was 7.6% compared to 6.2% in the present study. On the other hand, the rate of APH in Gamal Abd El Nasser Insurance HospitalCitation18 was more than what was found in this study in Dar Ismail Public Hospital (5.1% versus 2%).
The present study found that gestational diabetes was present in 5.4% of ElShatby women and in 2% of Dar Ismail Hospital, which was lower than what was reported in the Abo El Maatty study where in ElShatby and Gamal Abd El Nasser hospitals the rate of gestational diabetes was 14.2% and 10.1% respectively.Citation18
The present study showed that cardiovascular diseases were present in 3.1% of ElShatby women, with no cases among the women who delivered in Dar Ismail hospital. This 3/1% figure was lower than in the Abo El Maatty study which reported a rate of CVD 8.2% and 5.7% in ElShatby and Gamal Abd El Nasser Insurance hospitals respectively.Citation18
The present study showed that delivery in about half of all women was by caesarean section, with significantly different rates between the two hospitals. In ElShatby hospital, slightly over three-fifths of the women delivered by caesarian section (61.5%) compared to slightly over two-fifths of the females delivered in Dar Ismail Public Hospital (41.3%). The study’s overall rate of CS was higher than both the national average of hospital-based caesarean CS rates of 6.3% (range 0.3–37%)Citation19 and the WHO recommendation of 15%. There is no consensus worldwide as to what is an appropriate rate of caesarean section, but a rate below 5% may indicate poor coverage and inadequate access to the procedure, while a rate higher than 25% may reflect excessive use.Citation20 There are several possible reasons for the high rate of CS in this study. First, ElShatby University Hospital, as a university hospital, receives high risk pregnancy women in need for delivery by CS. Additionally, the high rate of primary CS increases the rate of repeated CS.
In this study, the most common cause of postnatal morbidity was hypertension (9.5% of all women), with a higher rate of 14.7% among ElShatby women compared to a rate of 4.7% among Dar Ismail women, with a significant difference between the two hospitals. Postpartum hemorrhage occurred in 6.9% of all the study women, with no significant difference between the two hospitals in this study. This figure is much less than the rate of 24.1% found in the Abo El Maatty study at ElShatby hospital in 2009.Citation18 It may be reasonably assumed that, over time, improvement of postnatal care has taken place at ElShatby University Hospital.
This study revealed that two women (0.8%) suffered from puerperal sepsis. They gave birth at ElShatby Hospital. This percentage is less than the 1.5% reported by the WHO systemic review.Citation11
In a study done by Roushdy in Egypt in 2006,Citation7 the direct causes of maternal death accounted for 69.5%, while indirect causes accounted for 30.5%. In the present study, all maternal deaths were at El Shatby Hospital, as a result of direct causes. Eclampsia accounted for 75% of cases. One case was due to postpartum hemorrhage (12.5%), and another case was due to ectopic pregnancy (12.5%).
One limitation to this study is that the population of Alexandrian mothers may not represent mothers of other governorates in Egypt. Moreover, the classification of hospitals into university and ministry of health would vary between frontier governorate and the lowest levels in metropolitan Egypt.
6 Conclusion
Future studies are needed to identify and understand better the avoidable factors contributing to the relatively high rates of maternal morbidity and mortality in public hospitals. Such information will be of significant use in the processes related to providing quality services, ensuring accessibility of those services, and allocating corresponding resources aimed at reducing maternal morbidity and mortality.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 10 February 2017
References
- World Health OrganizationReport on women and health: today's evidence tomorrow's agenda2009World Health OrganizationGeneva91
- P.S.RibeiroK.H.JacobsenC.D.MathersC.Garcia-MorenoPriorities for women's health from the Global Burden of Disease studyInt J Gynaecol Obstet10220088290
- V.FilippiR.GanabaR.F.BaggaleyHealth of women after severe obstetric complications in Burkina Faso: a longitudinal studyLancet370200713291337
- R.A.BangA.T.BangM.H.ReddyM.D.DeshmukhS.B.BaituleV.FilippiMaternal morbidity during labor and the puerperium in rural homes and the need for medical attention: a prospective observational study in Gadchiroli, IndiaBJOG1112004231238
- Maternal Mortality in Central Asia. Central Asia Health Review (CAHR); 2008.
- World Health OrganizationTrends in maternal mortality, released by the World Health Organization, the United Nations Children's Fund, the United Nations Population Fund and the World Bank2010World Health OrganizationGeneva September
- N.RoushdyClinical study: non obstetric hemorrhage: effectiveness of the non pneumatic anti shock garment in EgyptInt Sch Res Netw Obstet Gynecol62011
- A.CostelloK.AzadS.BarnettAn alternative study to reduce maternal mortalityLancet3689546201014771479
- World Health OrganizationMonitoring emergency obstetric care: a handbook2009World Health OrganizationGeneva152
- United Nations, Department of Economic and Social Affairs, Population Division (2011): World Population Prospects New York; 2010.
- G.MetinS.LaleP.B.AnaV.JoseP.GildaWHO systematic review of maternal mortality and morbidity: methodological issues and challengesBMC Med Res Methodol42004165
- World Health OrganizationThe prevalence of anemia in women: a tabulation of available information2nd ed.1992World Health OrganizationGeneva
- Agina MFH. Urinary Infections Among adult females out patients' attendants at the Banha University Hospital with special reference to pregnancy. Thesis, M.Sc. Egypt: Medical Microbiology. Zagazig: Banha Branch, Zagazig University Faculty of Medicine; 1985.
- Maqlad AF. Urinary Tract Infection Associated with pregnancy. Thesis M.Sc. Egypt: Medical Microbiology. Shebein El Koum: Menoufia University Faculty of Medicine; 1992.
- M.A.HagrasiB.Abu EitahM.A.SherifM.M.FahmA symptomatic bacteriuria in pregnant womenZag Univ Med J1041987255261
- A.M.Al HaddadUrinary tract infection among pregnant women in Al Mukalla district, YemenEast Mediterranean Health J1132005505511
- M.A.SheikhM.S.KhanG.M.ArianIncidence of urinary tract infection during pregnancyEast Mediterranean Health J622000265271
- Abo El Maaty N. study of maternal mortality and morbidity incidence among pregnant women in El Shatby maternity university and Gamal Abd El Naser health insurance hospitals. Thesis, M.Sc. Alexandria (Egypt): El Shatby University Maternity Hospital, Faculty of Medicine; 2009.
- M.F.CotchS.L.HillierR.S.GibbsD.A.EschenbachEpidemiology and outcomes associated with moderate to heavy Candida colonization during pregnancyAm J Obstet Gynecol17821998374380
- P.GichangiL.ApersM.TemmermanRate of Caesarean Section as a Process Indicator of Safe Motherhood Programs: The Case of KenyaJ. Health Popul Nutr192200152