
1 Introduction
Acute renal colic is a common clinical problem encountered in the emergency department [ER]. The most common cause of renal colic is ureteral stone. However, various intra-abdominal pathologies can cause the same clinical picture including appendicitis, diverticulitis, ovarian torsion, pancreatitis or vascular aneurysmCitation1 (see Figs. –).
Figure 1 A 45 male patient with left renal colic, (A) axial unenhanced MDCT showing left vesico-ureteral calculus (arrow), (B) Axial prone image, (C & D) unenhanced MDCT with curved multiplanar reformatted coronal and sagittal reconstruction showing the calculus (arrow), (E) Sagittal sonographic image of the left kidney shows moderate hydro-nephrotic and hydro-ureteral changes with the upper ureter measures 8 mm and (F) axial sonographic image of the urinary bladder shows left veiscourteral calculus 6 mm in size (arrow).
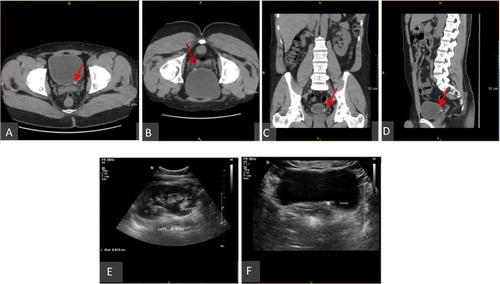
Figure 2 A 41 years old male patient with right renal colic, (A) axial unenhanced MDCT showing right upper ureteral hyper-attenuating calculus with positive rim sign along with moderate hydro-nephrotic and hydro-ureteral changes, (B & C) unenhanced MDCT with curved multiplanar reformatted coronal & sagittal images and (D) sagittal sonographic image of the right kidney shows moderate hydro-nephrotic changes.
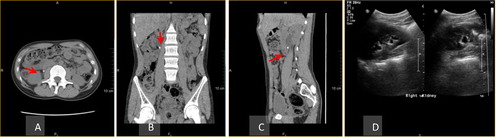
Figure 3 A 37 years old male with right renal colic, (A) axial unenhanced MDCT showing lower calyceal right renal hyper-attenuating calculus (arrow), (B & C) unenhanced MDCT with curved multiplanar reformatted coronal & sagittal images and (D) sagittal sonographic image of the right kidney shows the same finding.
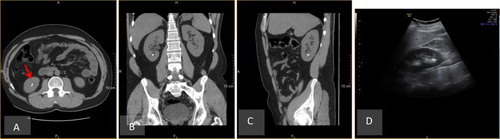
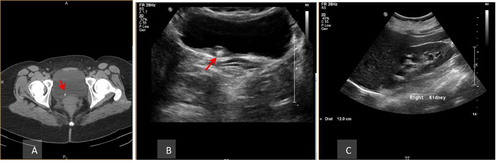
Figure 4 A 42 years old male patient with right renal colic, (A) axial unenhanced MDCT showing right vesico-ureteral calculus (arrow), (B) axial sonographic scan of the urinary bladder shows the calculus at the vesico-ureteral junction with localized hypo-echoic thickening at the bladder wall suggestive of edematous changes (arrow) and (C) sagittal sonographic scan of the right kidney shows moderate hydro-nephrotic changes.
Ultrasonography [US] can detect urinary calculi as echogenic foci with or without posterior acoustic shadowing which depends on the amount of calcium within a stone and on the stone size.Citation2 This examination has a lot of advantages including wide availability, cost-effectiveness, lack of radiation and no requirement of either intravenous contrast injection or patient preparation. It is efficient in detecting renal, vesico-ureteral junction and Vesical calculi,Citation3 but is not helpful in diagnosis ureteral stones especially those of the mid ureteral portion. Also it is insensitive to small calculi that are less than 2 mm.Citation4 It can detect urinary calculi consequent complications as hydro-nephrosis yet some patients complaining of acute obstruction may have little or no pelvicalyceal dilatation.Citation2 Furthermore sometimes extra-renal pelvis or pelvi-ureteral stricture can give false positive findingCitation5 (see and ).
Table 1 Comparison of the results of calculi detected by ultrasonography (US) and calculi detected by multidetector computed tomography (MDCT).
Table 2 Comparison of the results of secondary signs of obstruction (hydro-nephrosis/hydro-ureter) detected by US and MDCT in relation to calcular size in cases with ureteral and vesico-ureteral calculi.
Also Ultrasonography can help in detecting some of the other intra-abdominal pathologies that simulate urinary calculi clinically as cholycystitis, complicated ovarian cyst and abdominal aortic aneurysm.Citation1 But being operator depended is still a major disadvantage that cannot be ignored.
Un-enhanced helical CT has been used to evaluate renal colic since 1995 and after years of experience in this technique, conventional radiography and intra-venous urography became historical radiological examinations for evaluation of urinary tract calculi, especially in acute renal colic.Citation6 This technique showed high sensitivity reaching to 98–100% and specificity 92–100% for detection of urinary calcular disease. It is a quick examination, requiring no patient preparation or intra-venous contrast injection. Also it can give an idea about the chemical composition of the stone by measuring the attenuation and the attenuation/size ratio of the calculi,Citation7 and hence assist in the management of the patient. It helps in revealing other intra-abdominal pathologies that give similar clinical picture to the calcular disease.
The goal of this study is to evaluate the role of MDCT in diagnosis and management of urinary calculi disease compared to Ultrasonography for the patient with acute renal colic in emergency department.
2 Material and methods
This study included 137 patients presented to the ER department of a private hospital, complaining of renal colic during the period from October 2014 till January 2015. Inclusion criteria includes any adult with uncomplicated unilateral renal colic [Loin pain radiating to groin] and exclusion criteria was pediatric age group patients [Below 18 years of age] pregnant females or any patient with history of previous renal calculi or any other urinary disease. All the patients receive only pain killers in the ER before coming to the radiology department. No consent was taken as both US and MDCT were done as a part of routine management of these patients by ER departmental policy. Human ethics committee approval for this study was obtained from the institutional review board of the hospital. Ultrasonography and interpretation of the MDCT images were done by two experienced uroradiologists [15 years experience], US was done first and then MDCT was done in an interval of 30 min to 2 hours with the radiologist reporting the MDCT was blind to the US findings.
Un-enhanced MDCT was performed using a Multidetector row helical scanner [Light speed VCT 64, GE Medical systems, USA], A non low dose one phase protocol was used as by radiology departmental policy as follows; Gantry speed 0.4 s per rotation with an X ray voltage of 140–120 kV, and a current of 230–350 mA, slice thickness 5 mm, beam collimation of 1.25 mm, pitch 0.9. Patients were scanned in a supine position with a full bladder and in breath hold status. Scanning stared from the upper border of dorsal 11 vertebral body till the lower border of symphysis pubis. Scanning time was about 20 s. In cases with vesico-ureteral calculi, extra-images were taken for the bladder in a prone position. CT examination was performed without intra-venous, oral or rectal administration of contrast material. Data were sent to a compatible workstation and curved multiplanar coronal and sagittal reconstructions were obtained.
Ultrasonography of kidneys, ureters and bladder was done using ultrasound machine [HD II XE, Philips medical system, Nederland B.V] with 2–5 curved array transducer using abdominal setting.
For kidney examination patients were in supine or right/left lateral decubitus using liver or spleen as an acoustic window. Scanning was done during deep inspiration where sagittal and axial images for both kidneys were obtained.
For urinary bladder examination, patients were in supine position with full bladder. Sagittal and axial images for the bladder were taken.
Both MDCT and US images were reviewed on workstation [VEBRO, Germany] where findings included presence of calculi, calcular size and location and any consequent back pressure changes evident on either kidney or ureter. Additionally in CT; calculus attenuation value, attenuation/size ratio and rim sign in ureteral calculi were obtained.
A follow up of three months duration was done to the patients who had negative both US and MDCT examination to detect if they have been re-admitted again to the ER for the same complain (acute renal colic) to make sure that the negative cases are true negative and this time interval was suggests by the urologist who attended these cases in the ER.
3 Statistical analysis
IBM SPSS statistics [V.21.0, IBM Corp., USA. 2012] were used for data analysis. Chi-square test was used to study the association between each 2 variables or to compare between 2 independent groups as regarding the categorized data. The probability of error at 0.05 was considered significant while at 0.01 was highly significant.
4 Results
Among the 137 cases included in this study 45 were females [33%] and 92 were males [67%]. Their ages ranged from 18 to 75 years old [mean age of 46.5 years]. All the patients were presented with acute renal colic.
Sixty-one cases [44%] had negative both US and MDCT examinations, two cases of them [1.4%] passed calculi spontaneously [this data was obtained from ER records]. Retrospective reviewing of the CT images of these two cases revealed small calcified foci related to the lower ureter just above the vesico-ureteral junction. Both were of 2 mm average size and there was no ureteral dilatation or evident rim sign. They were misinterpreted as phleboli. The remaining fifty-nine [43%] cases were not admitted again to ER department with the same complain which is renal colic in an interval of 3 months duration post first scanning.
Seventy cases [51%] had calcular disease as follows; 19 cases [27%] showed renal calculi, 31 cases [44%] had ureteral calculi, 19 cases [27%] had vesico-ureteral junction calculi and one case [1.4%] showed Vesical calculus.
Eight cases [6%] had no calcular disease but they showed other positive renal findings in the form of, 3 cases had simple renal cysts, one case showed angiomyolipoma and one case revealed renal cell carcinoma. In those 5 cases both MDCT and US were able to detect the abnormalities. The rest of these 8 cases had extra renal findings as follows; one case sigmoid diverticulitis, one case post-appendectomy right iliac fossa inflammation and one case with suspected lower ureteral stricture. Only MDCT was able to reach a diagnosis in those cases with a 100% sensitivity compared to US which showed a sensitivity of 72%.
Concerning renal calculi [19 cases], MDCT was able to detect all the cases with sensitivity reaching up to 100%, while sonography detected only 18 cases with a sensitivity of 95% showing statistically non-significant difference between the two modalities in detecting renal calculi (p value > 0.05). Suggested reasons for missing this stone by sonography were likely related to the small size of the stone (which was 3 mm) and to its location (being in the lower pole of the left kidney which is sometimes masked by colonic gases). No secondary signs of obstruction as hydronephrosis and hydro-ureter could be detected.
Thirty-one cases of ureteral calculi were included in this study, 12 cases were in the upper third of the ureter [between the end of the pelvicalyceal system till the second lumber vertebra], 9 cases were in the mid ureter [between lumbar 2 vertebra till lumbar 4 vertebra] and 10 cases were in the lower ureter [below lumber 4 vertebral body till the vesico-ureteral junction]. Regarding the upper ureteral calculi MDCT detected all the cases with sensitivity reaching up to 100%, while sonography detected only 4 cases with sensitivity of 60%. Nineteen cases of the mid and lower ureteral calculi could not by detected by sonography due to obscuring of the ureter by bowel gases while MDCT detected all of the mid ureteral calculi with sensitivity of 100% while in the lower ureter it missed two calculi showing sensitivity of 83%. For overall ureteral calculi US gives 53% while MDCT gives 93% sensitivity showing statistically significant difference between two modalities with p value < 0.05.
Also in the nineteen cases of the vesico-ureteral junction calculi MDCT detected all the cases, while US detected only 8 cases showing statistically significant difference between two modalities with p value < 0.05.
Only one case with Vesical calculus was included in the study and it was of large size 40 mm and both modalities detected it easily, the cause of the renal colic in that case was probably due to intermittent obstruction of the ureteral orifice.
Regarding the ureteral and vesico-ureteral calculi with calcular size greater than or equal 6 mm [13 cases], both MDCT and US were able to detect secondary signs of obstruction [hydro-nephrosis/hydro-ureter] in 11 cases of them [84%], while in calculi smaller than 6 mm [37 cases], MDCT detected 20 cases [54%] compared to US which detected 13 cases [35%].
In the 31 cases of ureteral calculi, rim sign was observed in 21 cases [68%].
Seven cases of ureteral calculi underwent endoscopic calcular extraction [two calculi were in the mid ureter while the rest were in the lower ureter], the calculus size ranged from 6 mm to 10 mm. Their CT density was between 670 Hounsfield units [Hu] to 1300 Hu and their attenuation/size ratio was 103 up till 163.
5 Discussion
The goal of imaging in evaluating acute renal colic is to determine the presence of calcular disease, malignancy or malformation. Regarding calcular disease, we need to know calculi location, size and composition as these parameters affect the patient’s management where calculi above 5 mm are less likely to pass spontaneously in contrary to calculi less than 5 mm,Citation8 while low attenuation calculi like urate calculi respond well to medical treatment [urinary alkalinization] which is not suitable for high attenuation calculi like calcium oxalate.Citation9 Also assessing the presence of any complication as hydro-nephrosis/hydro-ureter or if there is no calcular disease encountered, trying to reach a final diagnosis explaining the patient’s complain.Citation10
US is considered a good modality in evaluating patients referred from ER department with renal colic especially in cases when we need to avoid radiation hazards as in pediatric age group and in pregnant females. US can easily detect renal calculi,Citation2 in this study its sensitivity was 95% compared to 100% for MDCT, regarding ureteral calculi it was 53% compared to 93% for MDCT and in vesico-ureteric junction calculi its sensitivity was 63% compared to 100% for MDCT, the low sensitivity of US in detecting ureteral calculi can be explained by the fact that most of the ureteral course is obscured by bowel gases and it needs a large sized stone with considerable hydro-ureteral changes to allow the modality to detect the abnormality.
Regarding presence of complications as hydro-nephrosis/ hydro-ureter, both modalities have equal sensitivity in calculi more than or equals to 6 mm but with calculi less than 6 mm, MDCT has a higher sensitivity with detection of 54% of the cases compared to 35% for US.
One of the major benefits of CT over US is the global examination of the whole abdomen and pelvis which can accurately detect other causes giving similar clinical picture of acute renal colic. In the eight cases of non calcular disease US could detect 5 cases, all of them with renal pathology giving sensitivity of 72% compared to 100% for MDCT.
Since the introduction of helical CT as an imaging modality for evaluation of renal colic by Smith et al in 1995, it has proven to be the most sensitive radiological modality in detecting and characterizing renal calcular disease.Citation11
Helical CT is superior to US in visualization of the whole ureteral course and by the availability of multi-slice scanners, in addition to shorter examination time, which is most needed in patients in acute pain, the volumetric manner of data acquisition with curved multiplanar reconstruction [MPR] technique to obtain coronal and sagittal images besides the routine axial images makes the assessment of any hyper-dense focus along the ureteral course much easier and to determine if it is in the ureter or calcification within a vessel wall or just a phlebolith.Citation1 Also in MDCT we can detect a rim sign which is a soft tissue area surrounding the calculus which can differentiate it from a phlebolith.Citation12 In this study rim sign was elicited in 21 cases [68%] out of 31 cases of calculi, so rim sign could be used as a CT finding to differentiate calculi from phleboli in problematic cases.
Measuring calculus size and attenuation value and obtaining attenuation/size ratio can give an idea about the composition of the calculus and hence its ability to be resolved by medical treatment or to be more amenable to shock wave lithotripsy. Mean attenuation value of 652 HU and attenuation/size ratio of 80 or greater was found to be highly suggestive of calcium oxalate calculi while urate calculi have mean attenuation value of 344 HU and attenuation/size ratio generally below 80.Citation13 In this study we could not evaluate this point properly because of the small number of cases [7 cases] who underwent ureteroscopic calcular extraction and calculus chemical composition analysis; however, all seven cases were calcium oxalate calculi, their mean attenuation value was 985 HU and mean attenuation/ size ratio was 133.
Radiation hazards should be considered when using MDCT as an imaging modality of choice, In this study a conventional, non-low dose, one phase CT protocol was performed, CT dose index [CTDI] for all the patient was between 6 and 21 mGy with mean of 12 mGy and Dose-Length Product [DLP] was between 280 and 970 mGy with mean of 459 mGy. According to the European Commission Radiation Protection report 118, the effective dose of CT is 10 mSv,Citation14 however, new low dose protocols for urinary calculi are available by modifying some of the CT parameters like increasing the pitch ratio and lowering either the KV or mAs, by this way the effective radiation dose can be reduced and by using these protocols there will be no much image noise that could obscure an alternative diagnosis if calcular disease is not detected,Citation15 but even with this reduction in effective radiation dose, the modality is not optimum for pregnant ladies and pediatric age group patients.
6 Conclusion
Un-enhanced MDCT outperforms Ultrasonography in evaluation of urinary tract calculi, it is the most sensitive test and it is recommended to be used as the first tool in the diagnostic work up of patients with acute renal colic when the risk of the disease outweighs the risk of radiation exposure.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
References
- Jia-HwiaWangShu-HuciShenShan-SuHiangCheng-YenChangProspective comparison of unenhanced spiral computed tomography and intravenous urography in the evaluation of acute renal colicJ Chin Med Assoc7120083036
- V.GianfrancoN.GiluseppinaF.PaoloUS detection of renal and ureteral calculi in patients with suspected renal colicCrit Ultrasound JSuppl 12013S3
- V.M.PaisA.L.PaytonC.A.La GrangeUrolithasis in pregnancyUro Clin North Am3420074352
- K.A.FowlerJ.A.LockenJ.U.DuchenseUS for detecting renal calculi with nonenhanced CT as a reference standardRadiology12002109113
- V.CauniR.MultescuB.GeavleteThe importance of Doppler ultrasonographic evaluation of the ureteral jets in patients with obstructive upper urinary tract lithiasisChirurgia (Bucur)1032008665668
- G.JindalP.RamchandaniAcute flank pain secondary to Urolithasis: radiologic evaluation and alternate diagnosisRadiol Clin North Am452007395410
- J.RichmondRadiological diagnosis of kidney stonesNephrology122007S34S36
- D.M.CollM.J.VaranelliR.C.SmithRelationship of spontaneous passage of ureteral calculi to stone size and location as revealed by unenhanced helical CTAJR1782002101103
- C.C.WenS.Y.NakadaTreatment selection and outcomes: renal calculiUro Clin North Am342007409419
- R.C.SmithM.VaranelliDiagnosis and management of acute ureterolithiasis: CT is truthAJR Am J Roentgenol175200036
- Smith JK, Lockhart ME, Kenney PJ. Urinary calculi imaging. Medscape, emedicine; 2015.
- G.J.MertenW.P.BurgessL.V.GrayPrevention of contrast induced nephropathy with sodium bicarbonate: a randomized controlled trialJAMA291200423282334
- B.TurkbeyE.AkpinarC.OzerMutlidetector CT technique and imaging of urinary stone disease: an expanded reviewDiagn Interv Radiol162010134144
- E.K.LangR.J.MacchiaR.ThomasImproved detection of renal pathologic features on multiphasic helical CT compared with IVU in patients presenting with microscopic hematoureaUrology612003528532
- M.K.SungS.SinghM.K.KalraCurrent status of low dose Multidetector CT in the urinary tractWorld J Radiol282011256265