
Abstract
Background
Obesity is gradually assuming an epidemic dimension among adults in Nigeria. Unfortunately, this has led to the increase in the prevalence of chronic diseases.
Objective
The study was designed to assess the prevalence of obesity among adults in Issele-uku, Aniocha North Local Government Area of Delta State, Nigeria.
Materials and Methods
The study employed a cross-sectional study design conducted among 201 respondents utilizing a simple random sampling technique. A validated semi-structured questionnaire was administered to obtain information from respondents; while descriptive and inferential statistics was used to analyze the data.
Results
The results show that more of the respondents were between the ages of 18–40 years, while about half 101(50.50%) were females and 104(52.0%) were married. Furthermore, only 46(23.0%) were overweight while 17.50% and 5.50% were pre-obese and obese respectively. The mean Body Mass Index of the respondents was 23.02 ± 4.42 while the respondents demonstrated positive attitude towards prevention of obesity. In addition, only eating akpu/fufu significantly predicted obesity (R2 = 0.034) while both sex (P = .350) and educational status (P = 0.165) did not significantly influence obesity and some of the respondents’ 82(41.0%) exercises once in a while.
Conclusion
The study recommended more awareness campaign on the dangers of obesity across communities in Nigeria.
1 Introduction
Obesity defined by the World Health Organisation,Citation1 as a Body Mass Index (BMI) ≥30 kg/m2 is gradually assuming an epidemic dimension in the world with Nigeria also having its own share of the burden.Citation2–Citation5 This current trend of obesity has been attributed to the socio-economic and epidemiological transition of Nigeria from a lower income country to a middle income country; resulting in the change of lifestyle behaviours and dietary intake. As a result many Nigerians now live sedentary lifestyle while at the same time consuming diet with excess caloriesCitation6; thus, resulting in high energy intake with low energy expenditure among most adult Nigerians. However, whatever the causes of obesity, its long term impact on the life of adults across Nigeria is well documented. Obesity has been shown to be a predisposing factor in the rising prevalence of morbidity and mortality associated with non-communicable diseases like type-2 diabetes mellitus, hypertension, cancer, stroke among adults.Citation7–Citation9 The World Health Organisation Global InfoBase have shown the increase in Nigeria of overweight and obesity by 23% in men and 18% in women and 49% in men and 39% in women between 2002 and 2010.Citation4,Citation5 In addition, several studies have also documented the prevalence of obesity in Nigeria, for instance a study in Ile-Ife South-West Nigeria documented the prevalence of overweight to be 20.30%,Citation10 while a similar study in Ilorin North-Central showed the prevalence of overweight to be 35.10%.Citation11 Furthermore, a similar study in Lagos South-West Nigeria also documented the prevalence of obesity to be 22.20%Citation12 while a study in Maiduguri North-East Nigeria showed the prevalence of obesity to be 8.10%.Citation13 Furthermore, according to the Global Health Observatory Data adverse metabolic effects such as blood pressure, cholesterol, triglycerides and insulin resistance can result from overweight and obesity. In addition, risks of coronary heart disease, ischemic stroke and type-2 diabetes mellitus increases steadily with increasing body mass index.Citation4 In addition, raised body mass index also increases the risk of cancer of the breast, colon, prostate, endometrium, kidney and gall bladder; while mortality rates increases with increasing degrees of overweight.Citation4
However, despite the glaring risk associated with obesity many adults in developing countries have the impression that overweight and obesity only affects the developed worldCitation5 and culturally in Nigeria there is this notion that any individual with huge body mass index is a sign that the individual is rich and is living well. This misconception has helped to promote the ongoing silence as it concerns obesity which has been shown to be on the increase in both urban and semi-urban areas.Citation14–Citation16 Therefore this study was carried out in a semi-urban community of Issele-uku to assess the prevalence of obesity among adults 18–60 years.
2 Materials and methods
2.1 Study design
The study utilized a descriptive cross-sectional design. Thus 200 persons were selected for the study from the age of 18–60 years.
2.2 Study area
The study was conducted in Issele-uku the headquarters of Aniocha North Local Government Area of Delta State. Issele-uku is comprised of 10 quarters namely; Ogbe-Ofu, Idumu-inei, Ogbedibo, Ogbolie, Ogbe-Owele, Ogbe-nti, Ogbe-utu, Ishiekpe, Idumu-Ahaba and Aniofu.
2.3 Study population
The study population comprises adults from 18 years to 60 years residing in Issele-uku town.
2.4 Sample size determination
Sample size was determined using single population proportion formula n = Z2 p (1 − p)/d2, with the following assumptions: prevalence (p) of 35% from previous studyCitation17 95% confidence level, 5% margin of error. Accordingly, the minimum sample size (n) was found to be 201.
2.5 Sampling procedure
Five quarters from issele-uku were randomly selected from the ten quarters in the community. The five quarters selected were Ogbe-Ofu, Idumu-inei, Ishiekpe, Ogbolie and Ogbe-utu quarters. Thus respondents were randomly selected from the five selected quarters.
2.6 Instrument for data collection
A semi-structured questionnaire was used to obtain information from the respondents. The questionnaire was structured into section A-F. Section A obtained information on respondents’ socio-demographic characteristics, B assessed the prevalence of obesity and section C sought information on respondents’ attitude towards obesity prevention. Furthermore, section D assessed respondents’ personal health history and eating habits, while section E identified the factors influencing obesity and section F assessed the type of exercise usually engaged by the respondents. In addition, Anthropometric measurement of height and weight were also done using standard calibrated instruments.
2.7 Data analysis
Responses from the questionnaires were entered into the computer and data generated were analyzed using Statistical Product for Service Solutions (SPSS) version 16.0 manufactured by IBM incorporated. Descriptive statistics was used to analyze the data which was presented in tables and charts. Chi-square test was used to determine the association between Body Mass Index and socio-demographic variables with level of significance set at P < .05. In addition, linear regression co-efficient R2 was used to predict the factors that influences obesity.
2.8 Anthropometric measurement
The height and weight obtained were used to calculate the Body Mass Index of the respondents using the formula BMI = Weight (kg)/Height (m2). Body-mass index categories were defined using the WHO cut points in units of kg/m2, normal weight = 18.5 kg/m2 - < 25 kg/m2, overweight = 25 kg/m2 - < 30 kg/m2 and obese ≥ 30 kg/m2. Other additional cut-off points used include severe thinness = <16.00 kg/m2, moderate thinness = 16.00–16.99 kg/m2, mild thinness = 17.00–18.49 kg/m2 while pre-obese = 25.00–29.99 kg/m2, obese class 1 = 30.00–34.99 kg/m2, obese class 11 = 35.00–39.99 kg/m2 and obese class 111 = ≥40.00 kg/m2.
2.9 Ethical consideration
Ethical clearance was obtained from the Department of Public and Community Health, Novena University. Verbal consent was also obtained from the community leaders in the community.
3 Results
3.1 Socio-demographic characteristics of the respondents
As shown in below, more of the respondents 50(25.0%) were between the age group of 18–24 years, 38(19.0%) between 25–30 years and 35(17.50%) between ages 31–35 years. In addition, about half 101(50.50%) were females while 99(49.50%) were males and more than half 104(52.0%) were married, 89(44.50%) were single respectively. Furthermore, 107(53.50%) of the respondents attained tertiary education; 72(36.0%) attained secondary education and 20(10.0%) primary education respectively. In the same vein, almost one third 65(32.50%) were business men and women, 39(19.50%) public servant and 19(9.50%) were farmers.
Table 1 Socio-demographic characteristics of the respondents.
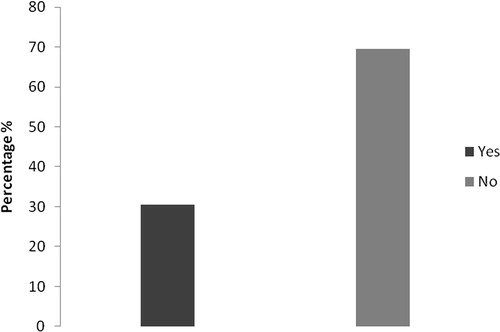
From below, almost majority of the respondents 139(69.50%) affirmed that they do not have a history of obesity in their family while 61(30.50%) affirmed that they do have a history of obesity in their family.
Fig. 1 Family history of obesity.
3.2 Prevalence of obesity among the respondents
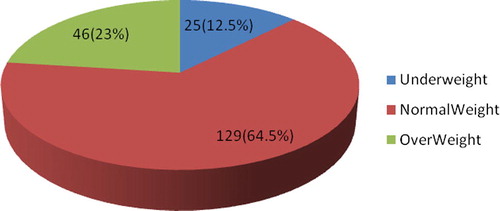
According to below, most of the respondents were normal weight 129(64.50%), 46(23.0%) were overweight and 25(12.50%) were underweight respectively.
Fig. 2 Prevalence of Obesity among the respondents.
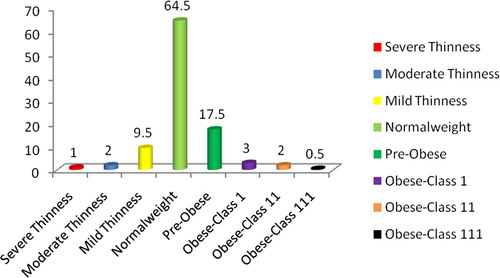
Breaking down the bodyweight of the respondents shows that 64.50% were normal weight, 9.50%, 2.0%, 1.0% had severe thinness, moderate thinness and mild thinness respectively while 17.50% were pre-obese, 3.0%, 2.0%, 0.50% were obese class 1, obese class 11 and obese class 111 respectively ().
Fig. 3 Prevalence of Obesity among the respondents.
As shown in below, the respondents had a mean height of 1.59 ± 0.074, mean weight of 58.44 ± 11.58 and mean BMI of 23.02 ± 4.42.
Table 2 Anthropometric characteristics of the respondents.
3.3 Attitude towards obesity prevention
According to below, almost one third of the respondents 65(32.50%) agreed that obesity can lead to death while 26(13.0%) disagreed. Furthermore, more than half 114(57.0%) strongly agreed that regular checking of weight is important to prevent obesity while only 5(2.50%) disagreed and almost half 99(49.50%) agreed that low fatty food can prevent obesity while 10(5.0%) disagreed. In addition, 112(56.0%) strongly agreed that exercising regularly can prevent obesity while 10(5.0%) disagreed and 101(50.50%) agreed that avoiding intake of fatty foods and meat can prevent obesity while 26(13.0%) disagreed.
Table 3 Attitude towards obesity prevention among respondents.
3.4 Health history
The health history of the respondents shows that majority 182(91.0%), 16(8.0%) and 2(1.0%) were never, rarely and often treated for heart disease while 171(85.50%), 23(11.50%), 6(3.0%) were never, rarely and often treated for hypertension respectively. Furthermore, 164(82.0%), 31(15.50%) and 4(2.0%) were never, rarely and often treated for diabetes while 182(91.0%), 11(5.50%) and 5(2.50%) were never, rarely and often treated for kidney problem ().
Table 4 Health History of the respondents.
3.5 Factors that influences obesity
According to below, only fufu/akpu significantly predicted obesity with a weak correlation and this account for only 3.40% of developing obesity. Other factors such as snacks, garri, chicken, pounded yam also have weak correlation and did not significantly predict obesity.
Table 5 Factors that influences obesity among the respondents.
According to below, more of the respondents 82(41.0%) only exercise once in a week while 23.0%, 18.0% and 13.50% only exercise weekly, daily and monthly respectively.
Table 6 Type of exercise engaged by the respondents.
The type of exercise engaged in by the respondents shows that 98(50.80%), 28(14.50%), 24(12.40%) and 22(11.40%) engaged in walking, football, skipping cycling respectively.
4 Discussion
4.1 Socio-demographic characteristics
The socio-demographic characteristics of the respondents’ shows more of the respondents were between the ages of 18–24 years, were females, married and were educated. This finding is slightly different from previous studies were the respondents age group were between 35–44 years and 21–30 years respectively.Citation18,Citation19
4.2 Prevalence of obesity
The Body Mass Index (BMI) classification of the respondents shows more of the respondents were normal weight and pre-obese. This finding is similar to previous findings in the six geopolitical zones in Nigeria where the respondents were normal weight and overweight and a study in Benue North Central where the respondents were also had normal weight and overweight.Citation18,Citation20
The mean anthropometric measurement of height, weight and BMI of the study was slightly lower than the study carried out in South-Western Nigeria, North-Central Nigeria and South-South Nigeria.Citation14,Citation19,Citation21
4.3 Knowledge of obesity among the respondents
Almost all of the respondents have heard or were aware of obesity and that awareness can be said to have translated into good knowledge of obesity among the respondents. This finding is different from a previous study in Jos where the respondents demonstrated fair knowledge of obesity.Citation22
4.4 Attitude towards obesity
In addition, the respondents exhibited good attitude towards obesity as they agreed obesity could lead to death if not properly handled, disposed to regular checking of weight to prevent obesity, eating more of low fatty food to prevent obesity and engage in regular exercise to prevent obesity. This finding is also similar to previous study in Nigeria where the respondents exhibited good attitude towards obesity.Citation23
Furthermore, majority of the respondents affirmed they have never been treated for any of the listed defects of heart disease, hypertension; diabetes and kidney problem. This findings is not surprising as very few of the respondents were obese and obesity is often a risk factor for most of these diseases.
More than one third 41.0% of the respondents say they exercise once in a while. However, this is not healthy enough and if not checked some of the respondents might become obese in the near future. There was no significant relationship between the numbers of times the respondents exercise and their BMI. This finding is consistent with previous studies.Citation22
The findings of the study showed more males were overweight than females, although this was not statistically significant. This findings was similar to previous study but had a significant relationship with BMI.Citation22 Possible reasons for this could be the fact that they have reduced physical activity but as males, are more likely to be taller than their female counterparts; since BMI is a function of both height and weight, the ‘shorter’ females have an increased tendency for obesity while ‘taller’ males are overweight. Similarly, respondents with tertiary education were more overweight than those with primary and secondary education; although the relationship was still not significant. This finding can probably be because people with higher tertiary education are assumed to have better socio-economic status and have been shown to be prone to obesity than their counterpart with lower socio-economic status.Citation14,Citation24,Citation25
The possible limitations of the study is that some of the assessed variables such as family history of obesity, health history and exercise routine were all based on the responses given by the respondents. Consequently, there was no independent or clinical confirmation of these variables.
4.5 Conclusion
The study showed most of the respondents had normal weight and some were already susceptible to obesity. In addition, some of the respondents still exhibit poor exercise lifestyle and consume calorie loaded food such as fufu/akpu, saturated containing food like kpomo, burgar, chicken, snacks which might cause them to be obese. Therefore, more efforts should be put in place by policy makers and health educational instructors in taking the message of obesity as a risk factor for most non-communicable diseases which is becoming more prevalent in Nigeria.
Conflict of interest
The authors declare no conflict of interest.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 12 November 2017
References
- World Health Organization. Technical Report Series. Geneva, Switzerland: World Health Organization. Physical Status: The Use and Interpretation of Anthropometry. 1995;854 1-1-9950.
- WHO: Fact sheet on Obesity 2010; 2012. <http://www.who.int/topics/obesity/en/>.
- B.M.PopkinL.S.AdairS.W.NgGlobal nutrition transition and the pandemic of obesity in developing countriesNutr Rev702012321
- Ono T, Guthold R, Strong K. WHO Global Comparable Estimates: Global Infobase data for saving lives; 2005. <http://apps.who.int/infobase/Index.aspx>.
- S.N.Akarolo-AnthonyW.C.WillettD.SpiegelmanC.A.AdebamowoObesity epidemic has emerged among NigeriansBMC Pub Health142014455
- G.U.P.IlohA.N.AmadiB.O.NwankwoV.C.UgwuObesity in adult Nigerians: a study of its pattern and common primary co-morbidities in a rural Mission General Hospital in Imo state, south-eastern NigeriaNig J Clini Pract1422011
- F.AziziM.RahmaniH.EmamiTehran lipid and glucose study: rational and DesignCVD Prevent32000242247
- R.WeissJ.DziuraT.S.BurgertObesity and the metabolic syndrome in children and adolescentsNew Engl J Med35023200423622374
- S.DaiD.R.LabartheJ.A.GrunbaumR.B.HarristW.H.MuellerLongitudinal analysis of changes in indices of obesity from age 8 years to age 18 yearsAm J Epid1562002720729
- R.A.AdedoyinC.E.MbadaM.O.BalogunR.A.AdebayoT.MartinsS.IsmailObesity prevalence in adult residents of Ile-Ife, NigeriaNig Q J Hosp Med1922009100105
- O.O.DesaluA.K.SalamiP.O.OluboyoJ.K.OlarinoyePrevalence and socio-demographic determinants of obesity among adults in an urban Nigerian populationSahel Med J11220086164
- C.O.AmiraD.O.B.SokunbiD.DolapoA.SokunbiPrevalence of obesity, overweight and proteinuria in an urban community in South West NigeriaNig Med J5222011110113
- A.L.OyeyemiB.O.AdegokeA.Y.OyeyemiB.DeforcheI.De BourdeaudhuijJ.F.SallisEnvironmental factors associated with overweight among adults in NigeriaInt J Behav Nutr Phys Act9201232
- A.O.SolaA.O.StevenJ.A.KayodeA.O.OlayinkaUnderweight, overweight and obesity in adults Nigerians living in rural and urban communities of Benue StateAnn Afr Med102011139143
- I.I.UlasiC.K.IjomaO.D.OnodugoA community–based study of hypertension and cardio–metabolic syndrome in semi–urban and rural communities in NigeriaBMC Health Serv Res1910201071
- I.O.AmoleA.D.OlaOlorunL.O.OdeigahS.A.AdesinaThe prevalence of abdominal obesity and hypertension amongst adults in Ogbomosho, NigeriaAfr J Prim Health Care Fam Med312011
- O.O.OladapoA.O.FalaseL.SalakoO.SodiqK.SoyinkaK.AdedapoPrevalence of cardiometric risk among a rural Yoruba South-Western Nigeria Population: a population based surveyCardiovasc J Afr2120102631
- C.I.OkaforI.D.GezawaA.A.SabirT.H.RaimiO.EnangObesity, overweight, and underweight among urban NigeriansNig J Clin Pract1762014
- R.A.AdebayoM.O.BalogunR.A.AdedoyinO.A.ObashoroJohnL.A.BisiriyuO.O.AbiodunPrevalence and pattern of overweight and obesity in three rural communities in southwest NigeriaDiab Metab Syndr Obes72014153158
- O.S.AdediranO.S.AdeniyiA.K.JimohO.O.AlaoUnderweight, overweight and obesity in adults Nigerians living in rural and urban communities of Benue StateAnn Afr Med1022011139143
- O.M.AdienboV.O.HartW.A.OyeyemiHigh Prevalence of Obesity among Indigenous Residents of a Nigerian Ethnic Group: the Kalabaris in the Niger Delta Region of South-South NigeriaGreener J Med Sci262012152156
- M.E.BanwatM.P.ChingleL.A.LarN.DamiA.I.ZoakahPattern of obesity among chief executives of public and private organizations in Jos, Plateau state, NigeriaNig J Basic Clin Sci9120121822
- I.J.NkwokaM.O.EguaM.AbdullahiA.Sabi’uA.I.MohammedOverweight and obesity among staff of Usmanu Danfodiyo University, Sokoto, NigeriaInternat Res J582014290295
- L.McLarenSocioeconomic status and obesityEpidemiol Rev2920072948
- A.DrewnowskiS.E.SpecterPoverty and obesity: the role of energy density and energy costsAm J Clin Nutr792004616