Abstract
Objectives: We provide an overview of the development of robotic surgery in the Middle East since its first introduction in April 2003 in the Kingdom of Saudi Arabia (KSA).
Methods: We searched MEDLINE using 20 keywords/phrases and identified 44 reports, of which only 15 were relevant. Five of these articles were duplicated when using two different keywords. Therefore, no more than 10 articles were found that were relevant to the scope of this review.
Results: After completing the MEDLINE search to identify articles related to robotic surgery in the Middle East, we noted that all of the nine case series (Level of evidence 3a) reported took place in the KSA, with no other reported series from other Middle-Eastern countries. To the best of our knowledge, there are no operating robotic surgery systems (da Vinci, Intuitive Surgical, CA, USA) in the Middle East other than in the KSA, Qatar and Egypt. The number of robotic surgery cases and newly adapted robotic procedures is increasing. Two major institutions in the KSA have expanded to robotic-assisted pyeloplasty in all of their cases since January 2005.
Conclusion: There are 10 da Vinci robots in the KSA, with over 35 trained surgeons, yet very few index cases. The cancer incidence rate, lack of practitioners’ referrals, and demographic age distribution are all factors that contribute significantly to the few index cases reported. By consolidating the robotic surgery procedures in high-volume speciality centres, hospitals can increase their case loads by promoting the multidisciplinary use of the robotic system. Even though growth is relatively slow, we believe that robotic surgery is gaining momentum, and its benefits and innovation will soon be grasped in other countries in the Middle East.
Introduction
The use of robotic-assisted surgery has grown exponentially over the past decade. It has revolutionised minimally invasive techniques for many surgical procedures worldwide, and has been adopted rapidly over the past 4 years in both the USA and Europe [Citation1]. The da Vinci robotic system (Intuitive Surgical, Sunnyvale, CA, USA) is the only surgical system that was approved for general laparoscopic surgery by the USA Food and Drug Administration (FDA) in 2000, and the only system to have received approval for cutting and suturing [Citation2]. It was approved for prostatectomy procedures in 2001, for urological surgical procedures in March 2005, for gynaecology in April 2005 and paediatric surgery in June 2005 [Citation3]. The major beneficial features of robotic-assisted surgery over standard laparoscopy include an articulating wrist with seven degrees of freedom, a three-dimensional camera system with up to ×€15 magnification, elimination of surgeon’s tremor and improved surgeon’s ergonomics. As such, robotic-assisted surgical techniques will enable the surgeon to achieve more precise surgery and better performance for specific operations [Citation2]. All these factors combined with well-trained surgeons at a highly experienced centre can improve patient outcomes. These positive outcomes include a shorter hospital stay and decreased intraoperative estimated blood loss [Citation2].
The USA market is the leader in robotic applications, with the global market a few years behind in the adoption cycle [Citation4]. By the end of 2010, the number of robot-assisted procedures that are performed worldwide has grown by ×≈347% since 2007, from 80 000 to 278 000 [Citation1,Citation3]. Of those procedures, Intuitive Surgical estimated that ×≈110 000 were hysterectomy procedures and ×≈98 000 were prostatectomy procedures, according to the Intuitive Surgical 2010 annual report [Citation3]. Other procedures have shown significant growth in urology and gynaecology, such as partial nephrectomy and sacrocolpopexy, respectively [Citation3].
Worldwide, between 2009 and 2010, the number of da Vinci systems that were installed in major hospitals increased by ×≈30%, from almost 338 to 441 [Citation3]. Currently, 1840 units have been sold and installed in over 1450 hospitals worldwide [Citation5].
In the Middle East, robotic surgery was first introduced in the Kingdom of Saudi Arabia (KSA) in 2003. At present there are 10 da Vinci robotic systems installed in eight major hospitals across the KSA. In 2010, Qatar founded the new Qatar Robotic Surgery Centre (QRSC), acquiring three da Vinci robots. To the best of our knowledge, there are no operating da Vinci robots in the Middle East other than the KSA, Qatar, and Egypt. A search of previous reports identified nine reported case series, all of which took place in the KSA, with no other reported series from other Middle-Eastern countries.
Methods
We searched MEDLINE using keywords such as ‘robotic surgery’ with a country name added (Saudi Arabia, Lebanon, Egypt, Qatar, United Arab Emirates, Dubai, Kuwait, Bahrain, Tunisia, Oman). The search identified only 10 articles that were relevant (, ), nine of which were case-report series from different institutions in Saudi Arabia, and one that explored the role of media coverage and marketing of robotic-assisted radical prostatectomy on the Internet. The remaining information in this review was acquired from the operative records collected by the da Vinci system local distributor.
Figure 1 The MEDLINE search diagram depicting the number of hits and the number of reports included.

Table 1 The number of keywords yielded 44 hits, 15 of which are significant.
Robotic surgery in the KSA
The first da Vinci system was installed in 2003 (); currently there are 10 robotic systems installed in the KSA of which six are distributed amongst four major hospitals in the capital city of Riyadh. Two are installed in different hospitals in the eastern province and two are installed in different hospitals in the western region.
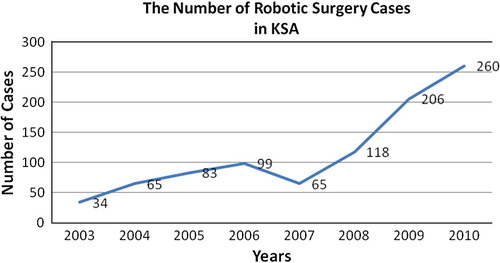
Figure 2 The number of robotic surgery cases in the KSA; the rapidly increasing adoption of surgical robots is due to the benefits provided to both surgeons and patients [Citation4].
According to the da Vinci data, there are over 35 medical doctors in KSA trained to work with the da Vinci surgical systems in the following fields; 12 in urology, eight in gynaecology, 10 in general surgery, three in thoracic and two in ear, nose and throat.
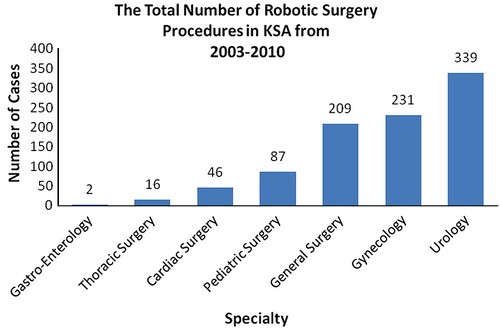
Over the past 7 years the number of procedures performed, by specialisation, in KSA were; 339 in urology, 231 in gynaecology, 209 in general surgery, 87 in paediatric and 46 in cardiac surgery ().
Figure 3 Robotic surgery procedures performed in the KSA by speciality.
Reported case series and single case reports in the KSA
Khairy et al. [Citation6] were the first to report their experience with robotic-assisted laparoscopic surgery, describing 42 robotic-assisted operations that took place between April 2003 and March 2004. Of the 42 cases, 25 were cardiac procedures and nine were cholecystectomies. They showed that robotic-assisted minimally invasive surgery can be carried out safely and can be applied in surgical fields where conventional laparoscopy can have difficulties in access [Citation6].
Alqahtani et al. [Citation7] reported their initial experience with 144 robot-assisted paediatric surgical procedures using the da Vinci robot, and showed that robotic surgery is indeed safe and feasible for several different paediatric surgical procedures, which included 39 fundoplications, 34 cholecystectomies, 25 gastric bandings, 13 splenectomies, four anorectal pull-through operations for imperforate anus, four nephrectomies, four appendectomies, four sympathectomies, three choledochal cyst excisions with hepaticojejunostomies, three inguinal hernia repairs, and two each of liver cyst excision, repair of congenital diaphragmatic hernia, Heller’s myotomy, and ovarian cyst excision; and one each of duodeno-duodenostomy, adrenalectomy, and hysterectomy [Citation7]. Ten of the 144 procedures were converted to either open surgery or to conventional minimal access surgery. Seven cases were converted to open surgery as a result of major bleeding, huge size of the organ, obstruction of the portal area creating a porto-enteric anastomosis, and failure of progression after a relatively long operating time [Citation7]. One of the three conversions to laparoscopic surgery was due to difficulty in suturing in the anterior abdominal wall during the repair of congenital diaphragmatic hernia procedure. The reasons for conversion were not related to system failure of any sort. They concluded that further system improvements and randomised studies are required to better assess the added benefits of robotic surgery compared to laparoscopic surgery [Citation7].
Alqahtani et al. [Citation8] also conducted a comparative study between 25 robotic-assisted gastric-banding procedures, all completed by one surgeon, and 50 laparoscopic adjustable gastric banding procedures. There were neither conversions nor intraoperative surgical complications. They showed that there the surgery was significantly longer for the robotic procedure than for laparoscopic banding, with no clear benefits and improvement in patient outcome. As a result, Alqahtani et al. aborted the use of robotic surgery in paediatric bariatric procedures.
In 2007, we described our experience in a single case report in which we used robotic-assisted surgery for an extended partial cystectomy and bilateral pelvic lymphadenectomy with en bloc resection of the umbilicus, urachus and bladder dome [Citation9]. The total operative time was 280 min, with an estimated blood loss of 100 mL and a total hospital stay of 3 days [Citation9]. We believe that for certain surgical procedures, the robot seems to be a promising new technique in surgical technology [Citation9].
Al-Othman et al. [Citation10] described, in a single case report, the feasibility of the da Vinci robot for performing robotic augmentation enterocystoplasty with a completely intracorporeal approach. As it was their first case, the operative time was 8 h, with a total hospital stay of 4 days [Citation10]. There is a need for a well-designed study to better describe and validate the assessments of these new procedures.
In 2008, we reported the second documented case, at the time, of robotic-assisted radical prostatectomy (RARP) in a patient with a pelvic kidney [Citation11]. The presence of an ectopic pelvic kidney is a challenge for the surgeon during RARP in avoiding injury to the pelvic kidney. Using the da Vinci robot in a technically challenging operation proved to be safe, feasible and can be carried out within the same operative time, incurring no excessive blood loss [Citation11]. The three-dimensional visual capabilities and advanced unique design of the instrumentation allowed us to perform such a delicate procedure through a 2–3 cm skin incision [Citation11].
Albassam et al. [Citation12] described a single-institution retrospective study comparing robotic-assisted Nissen fundoplication to the conventional laparoscopic Nissen fundoplication. They found that the hospital stay, the postoperative care requirements and postoperative outcomes were not significantly different between the approaches, suggesting that robotic-assisted Nissen fundoplication is a safe and feasible technique [Citation12].
Sait et al. [Citation13] reported their initial experience with 62 procedures in robot-assisted gynaecological surgery using the da Vinci robot. Four of the 62 procedures were converted to an open approach due to poor selection of one patient, bleeding and some technical problems with the robotic system [Citation13]. Robotic-assisted surgery in gynaecological practices appears to be safe, practical and well appreciated by the surgeon for certain procedures such as extended hysterectomy with pelvic lymph node dissection [Citation13]. A multi-institutional study will be required to better assess the advantages of robotic surgery in gynaecological practices [Citation13].
More recently, Al Bassam et al. [Citation14] addressed the feasibility, safety and early functional outcomes of using robotic surgery in the repair of anorectal malformations (ARMs). Their study, which they suggested as possibly the first to be published, consisted of a single institutional retrospective review of five male infants who underwent robotic-assisted repair of ARMs with recto-urethral fistula between April 2006 and March 2010. The same principle of the Georgeson technique was used in the robotically operated patients. All five procedures were performed by one surgeon who had a wide experience in both laparoscopic and robotic surgery. The five procedures were successfully completed without conversion. One patient developed left-sided epididymo-orchitis after surgery. All the patients had their colostomy closed. The follow-up was 6–36 months. Faecal continence was difficult to assess in two patients, and two patients had voluntary bowel movements without soiling. One infant had faecal soiling and is on a laxative/enema for constipation. The authors concluded that robots are very helpful in performing the anorectal pull-through in small infants. It offers a good alternative to the standard posterior sagittal anorectoplasty for repair of ARMs with recto-urethral fistula. Early results are encouraging, although more patients with a long-term follow-up are needed to further evaluate the outcomes.
QRSC
In April 2010, Qatar became the latest country in the Middle-East to establish a robotic surgery centre, the QRSC [Citation15], which serves as a training centre for doctors and nurses on robotic and minimally invasive surgery [Citation15]. The Hamad Medical Corporation greatly contributes to the quality of these training programmes, by organising live clinical observation, by jointly operating the animal laboratory, and by sharing experience, staff and other resources [Citation15]. The centre is equipped with three da Vinci medical robots, a three-dimensional surgical simulator of minimally invasive surgery for training, and a tele-mentoring theatre that allows distance training with leading doctors in other countries [Citation16].
Robot-assisted urological surgery in the KSA
Since clearance was granted by the FDA, there has been an exponential growth in the adoption of robotic-assisted procedures, especially in urology. After the rapid adoption of RARP, > 80% of RPs in the USA will be done robotically in 2010, according to unverified estimates from Intuitive Surgical [Citation17]. It has since expanded to procedures such as robotic-assisted nephrectomy (partial and total), robotic-assisted pyeloplasty and robotic assisted cystectomy [Citation18].
Until 2010, RARP has been the most adopted robotic procedure by urologists around the world [Citation3]. Despite the lack of randomised controlled studies on the outcomes of RARP vs. open RP, there have been numerous case series indicating the advantages of RARP, with significantly less blood loss, shorter hospital stay and lower rates of positive surgical margins than for open RP [Citation19].
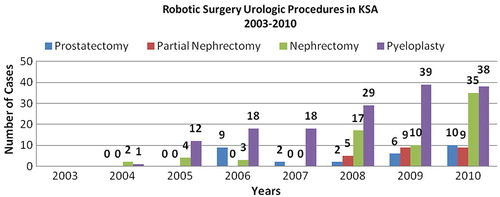
According to the data provided by the da Vinci distributor in the KSA, the total number of RARPs performed since 2004 until the end of 2010 was only 29 (). Based on these data, it could be argued that the rate of adoption is very slow and that most RPs were open. The truth is that the incidence of prostate cancer in the KSA is much lower than in the USA and Europe. In the KSA the age-standardised incidence rates of prostate cancer in 2007 were 5.7/100 000, whereas the reported values for the USA, Norway, Wales and Ireland in 2007 were 106, 109, 126 and 131.6, respectively [Citation20]. The figures reported from the Saudi Cancer Registry depended mainly on hospital-based approaches, for which some do not even have a medical record available. There is a need for community-based studies to explore the actual incidence rates of prostate cancer in the KSA. We believe that there is a substantial under-reporting of clinically diagnosed cases of prostate cancer, as well as other types of urological cancers, in our population [Citation21]. During our first prostate-cancer screening trial in 2008, we noted, among men of different age groups, that one of the major barriers for early treatment is the stigma associated with a diagnosis of cancer. This stigma often leads to late diagnosis, in which the patient usually presents with locally advanced or metastatic disease, and in turn, the treatment options offered are not surgical. Clearly, there is an urgent need to devise a nationwide prostate cancer awareness campaign, coupled with recommendations for annual screening, for all men aged ⩾€50 years, endorsed by urologists across the country. This will inevitably cause a high rate of PSA testing and screening, and the escalating use of PSA testing and subsequent biopsy will potentially increase the rate of diagnosing prostate cancer at an early stage, at which RARP can be offered as a safe and effective treatment for localised prostate cancer.
Figure 4 Robotic surgery urological procedures in the KSA, 2003-2010.
In 2011, at our institute, we have had seven men who have undergone RARP; their mean (SD) age was 63 (6) years. The mean operating time was 240 min and the surgical margin status was negative (unpublished data). This evidently shows the increase in the number of patients diagnosed with localised prostate cancer due to the active guidance of urologists for men to undergo PSA screening. In fact, we used robotic technology for all RPs since January 2005. In parallel, we and colleagues at another major institute in the KSA used robotic technology in all cases of pyeloplasty since January 2005, with no conversion reported [Citation22]. shows the variety of urological procedures that are currently adapted to robotics at our centre, as well as robotics applications that can potentially be adopted in the future. The improved patient outcomes, including less blood loss, lower infection rate and shorter hospital stay, influenced our decision to adopt robotic surgery, combined with the strong marketing that potentially attracts patients to hospitals where robotic surgery is available. A recent study by Alkhateeb et al. [Citation23] showed that media coverage and aggressive marketing have played an important role in the wide adoption of RARP. However, in a separate study it was reported that patients who had RARP were less satisfied and more regretful than those who had undergone open RP [Citation24]. This was probably due to the high level of expectation, driven by the hyperbole surrounding the procedure [Citation24]. Therefore, apart from instigating nationwide prostate cancer awareness campaigns, we believe that urologists should have a major role in educating patients, by providing them with accurate and realistic information based on the local perioperative outcome data available at their institute, as opposed to outcome data published from different groups from various centres.
Table 2 Robotic-assisted urological procedures in our centre.Table Footnotea
It is evident that there are many robotic systems in the country, but it appears that they are not used to their maximum potential (). The 930 da Vinci procedures were completed in the KSA from the introduction of the da Vinci system in April 2003 until December 2010. Although, 10 da Vinci robots have been installed, it seems that there are too many systems available to suit very few index cases, despite having more trained surgeons, some of whom have already passed the learning curve after completing over 20 cases [Citation25]. The many robotic systems, in addition to the many trained surgeons and relatively few cases, has led to the dilution of a surgeon’s experience. This relatively low volume of robotic cases will also have an effect on Resident’s teaching. As Residents and Fellows will have no opportunity to train in robotic-assisted procedures, due to the low volume of caseload, their training will most likely be compromised. Moreover, with one robotic-assisted procedure per month for example, the surgeon will find it difficult to attain the optimal benefits of robotic surgery with more favourable outcomes than those currently achieved. These few index cases are probably related to many factors, e.g. the demographic age distribution of the population and the nature of disease prevalence; 26.4%, 8%, 4.2%, 1.8% and 1.8% of the Saudi population in 2006 were in the age groups of 0–4, 45–49, 55–59, 65–69, and 70–74 years, respectively [Citation20]. Poor referral patterns amongst practitioners are another factor. Although there are many studies reporting informed recommendations on the transition from conventional laparoscopy to robotic-assisted laparoscopic procedures [Citation26], clearly some healthcare institutions in the KSA need better planning and resource allocation to better assess the maturity of installing a da Vinci robot vs. the annual volume of caseload needed.
Conclusion
Robotic technology has modernised the field of surgery. Several case series have reported the feasibility and safety of using robotic-assisted procedures in various surgical disciplines. Even though randomised trials are lacking, there is clear evidence from retrospective studies that some robotic surgery applications can reach satisfactory functional and oncological outcomes compared to laparoscopic and open techniques.
The increase in cancer incidence rates due to higher PSA screening and awareness campaigns will most likely increase the volume of referrals for patients to be treated at an early stage in which the rapidly accepted robot-assisted surgical technique can be provided as an optional choice for the patient. Another way to potentiate the use of robotics in urological surgery in the Middle East is by consolidating robotic surgery in centres of excellence, and providing an easy referral pattern for these patients. Robotic surgery also costs more than other techniques, because of the initial cost of the robot in addition to its higher maintenance and support costs. Unlike in the USA, where some robotic procedures receive reimbursements from private health insurance companies or the federal Medicare system, the healthcare systems and reimbursements in the Middle East are lagging behind. Until high-volume outcomes are achieved, various robotic procedures and system growth in the Middle East will be slow; however, we believe that the long-term opportunity for robotic surgery in the Middle East is significant.
Conflicts of interest
The authors indicate no potential conflicts of interest.
Research support
This paper is supported by Princess Jouhara Al-Ibrahim Cancer Research Center, Prostate Cancer Chair.
Notes
Peer review under responsibility of Arab Association of Urology.
References
- G.I.BarbashS.A.GliedNew technology and health care costs - the case of robot-assisted surgeryN Engl J Med3632010701704
- C.Ben MessaoudH.KharraziK.F.MacDormanFacilitators and barriers to adopting robotic-assisted surgery. Contextualizing the unified theory of acceptance and use of technologyPlos ONE62011e16395
- Intuitive Surgical Inc. Annual Report 2010. Available at http://investor.intuitivesurgical.com/phoenix.zhtml?c=122359&p.=irol-reportsAnnual.
- Robotic Surgery Market Report. 2011 Edition. Available at http://www.aarkstore.com. Accessed April 2011.
- Intuitive Surgical Products. Frequently Asked Questions. Available at http://www.intuitivesurgical.com/products/products_faq.html. Accessed November 2011.
- G.A.KhairyM.FoudaA.AbdulkarimA.Al-SaighK.Al-KattanEvaluation of robot-assisted laparoscopic proceduresSaudi Med J262005777780
- A.AlqahtaniA.AlbassamM.ZamakhsharyM.ShoukriT.AltokhaisA.Aljazairiet alRobot-assisted pediatric surgery. How far can we go?World J Surg342010975978
- A.AlqahtaniRobotic gastric banding in children and adolescents: a comparative studySurg Endosc25201136473651
- D.M.RabahRobot-assisted partial cystectomy for the treatment of urachal carcinomaCan J Urol14200736403642
- K.E.Al-OthmanH.A.Al-HellowH.M.Al-ZahraniR.M.SeyamTechniques in endourology robotic augmentation enterocystoplastyJ Endourol222008597600
- D.M.RabahF.A.AlyamiRobotic-assisted transperitoneal radical prostatectomy in a patient with pelvic kidneySaudi Med J292008288290
- A.A.AlbassamM.S.MallickA.GadoM.ShoukryNissen Fundoplication, robotic-assisted versus laparoscopic procedure: a comparative study in childrenEur J Pediatr Surg192009316319
- K.SaitEarly experience with the da Vinci surgical system robot in gynecological surgery at King Abdulaziz University HospitalInt J Women’s Health32011219226
- A.Al BassamA.GadoM.S.MallickM.Al NaamiW.Al-ShenawyRobotic-assisted anorectal pull-through for anorectal malformationsJ Pediatr Surg46201117941797
- Qatar launches robotic surgery centre. Available at http://www.arabianbusiness.com/qatar-launches-robotic-surgery-centre-155454.html. Accessed April 2010.
- The Qatar Robotic Surgery Centre. Available from: http://allaboutroboticsurgery.com/trainingcenters.html. Accessed March 2010.
- W.T.LowranceT.V.TarinS.F.ShariatEvidence-based comparison of robotic and open radical prostatectomyScientific World J10201022282237
- P.BabbarA.K.HemalRobot-assisted urologic surgery in 2010 - Advancements and future outlookUrol Ann3201117
- J.A.SmithJrR.C.ChanS.S.ChangS.D.HerrellP.E.ClarkR.Baumgartneret alA comparison of the incidence and location of positive surgical margins in robotic assisted laparoscopic radical prostatectomy and open retropubic radical prostatectomyJ Urol178200723852389
- Cancer Incidence and Survival Report Saudi Arabia 2007 Saudi Cancer Registry, Ministry of Health, KSA. Available at http://www.scr.org.sa/reports/SCR2007.pdf Figure 3.11.4, page 57, Figure 1.2, page 10.
- D.M.RabahM.A.ArafaProstate cancer screening in a Saudi population: an explanatory trial studyProstate Cancer Prostatic Dis132010191194
- H.Al-Zahraniet al personnel communicationKing Faisal Specialist Hospital And. Research Center, Riyadh (KFSHRC-R
- S.AlkhateebN.LawrentschukConsumerism and its impact on robotic-assisted radical prostatectomyBJU Int108201118741878
- F.R.SchroeckT.L.KrupskiL.SunD.M.AlbalaM.M.Priceet alSatisfaction and regret after open retropubic or robot-assisted laparoscopic radical prostatectomyEur Urol542008785793
- W.ArtibaniS.FracalanzaS.CavalleriM.IafrateM.Aragonaet alLearning curve and preliminary experience with da Vinci-assisted laparoscopic radical prostatectomyUrol Int802008237244
- P.L.SteinbergP.A.MerguerianW.BihrleJ.A.HeaneyJ.D.SeigneA da Vinci robot system can make sense for a mature laparoscopic prostatectomy programJSLS122008912