Abstract
Objective: To evaluate the detectability, size, location and density of urinary stones with unenhanced computed tomography (CT), using the half-radiation (low) dose (LDCT) technique, compared with the standard-dose CT (SDCT), in obese patients.
Patients and methods: The study included 50 patients with a body mass index of >30 kg/m2 and bilateral renal stones diagnosed with SDCT, and managed on one side. All the patients had LDCT during the follow-up and SDCT was used as a reference for comparison.
Results: Of the 50 patients, the right side was affected in 27 and the left side in 23. In all, 35 patients had a single stone while the remaining 15 had multiple stones. With SDCT, 95 stones were detected; there were 45 of ⩽5 mm, 46 of 6–15 mm and only four of >15 mm. LDCT barely detected three stones of <3 mm, compared with SDCT, while larger stones had the same appearance at both scans. The site of stone in the kidney or the ureter did not affect its detection on LDCT vs. SDCT. The mean stone diameter was identical in both techniques. At LDCT, all stones were detected with no difference in their number, location or density vs. SDCT. However, the tube current and radiation dose were significantly lower with LDCT.
Conclusions: In obese patients with stone disease, LDCT is as accurate as SDCT, while avoiding exposure of the patient to high-dose radiation.
Abbreviations:
Introduction
Urolithiasis is a worldwide problem, affecting all geographical, cultural and racial groups [Citation1]. The lifetime risk is 10–15% in the developed world, but can be as high as 20–25% in the Middle East [Citation2]. Nephrolithiasis is largely a recurrent disease with a relapse rate of 50% in 5–10 years and 75% in 20 years [Citation3,Citation4]. CT is now recommended by many as the initial diagnostic imaging technique in patients with suspected renal or ureteric calculi [Citation5,Citation6]. Unenhanced CT has a sensitivity and specificity of 97% and 96%, respectively, for detecting urolithiasis [Citation7]. Currently, CT is the reference standard method for diagnosing urolithiasis, but it is also the major source of exposure to radiation during medical imaging [Citation8,Citation9].
Renal colic commonly affects young adults and it has a high rate of recurrence, reaching 50% [Citation10]. The repeated use of unenhanced CT for imaging patients with renal colic creates a risk of high radiation exposure on standard-dose CT (SDCT). Katz et al. [Citation11] stated that 4% of the patients in their study required repeated (three or more) CT studies for renal colic. Therefore, many authors have assessed a low-radiation dosage protocol for evaluating flank pain and detecting renal stones. Low-dose CT (LDCT) has become the standard for diagnosing urolithiasis, with various protocols and LD settings resulting in a different radiation exposure [Citation11–Citation18]. CT tube current is the most commonly adjusted scanning variable for reducing the radiation dose in CT. The radiation dose is linearly related to the tube current, so a 50% reduction of tube current implies a 50% reduction in radiation dose [Citation19]. The tube current for dose reduction can be adjusted by manual selection of a lower fixed tube current or with automatic exposure control.
In recent reports authors still claim limitations to LDCT for diagnosing urolithiasis in obese patients [Citation17,Citation20]. In these studies, older CT scanners (four-slice multi-detector CT) were used for image acquisition. Most of the studies comparing SDCT and LDCT did not use the possibilities of automatic tube-current modulation that is available in modern multi-slice CT scanners. Using this automatic current modulation gives the possibility of reducing tube current without changing it manually, depending on patient weight/body mass index (BMI) [Citation21].
The purpose of the present study was to evaluate stone detectability, size, location and density with unenhanced CT using the LDCT (half dose) compared with SDCT, using a 64-row multi-detector CT scanner, in obese patients.
Patients and methods
Study design
This prospectively designed study was conducted between January 2009 and August 2011, and included 50 patients (37 men and 13 women; mean age 43.8 years, SD 11.2, range 19–73) with a BMI of >30 kg/m2 and bilateral urinary tract stones diagnosed with SDCT, who were managed on one side. Unenhanced scans of the abdomen and pelvis from the diaphragm to the symphysis pubis were taken for all patients with the automatic SD protocol before intervention. Thereafter, all patients had unenhanced LDCT of the urinary tract during the follow-up, after intervention on one side. Images of the unoperated side were used for comparison between SDCT and LDCT; SDCT images were considered as the reference standard.
Imaging technique
The study was conducted using a 64-multi-slice helical CT scanner (Brilliance, Philips, The Netherlands). Imaging parameters for both SDCT and LDCT studies were the same (120 kV for all patients) except that the tube current was manually reduced to obtain half the radiation dose. The slice thickness was 5 mm with a 2-mm overlap. To measure the radiation dose we used the radiation-dose descriptor, termed the CT dose index, that integrates the radiation dose delivered both within and beyond the scan volume, and is the principal dose descriptor in CT, automatically calculated by the machine.
Studied parameters
All examinations were reviewed on a picture archiving and communications system (Magic View, GE, Milwaukee, WI, USA) by two experienced radiologists, and the patients were diagnosed by consensus. To measure the attenuation value we selected a region of interest for each stone, drawn manually and that included most of the stone, sparing its margin. The same window width and level were used for reading the SDCT and LDCT images. The radiologists viewed all images, compared the same level of the two studies at the same time, using the ‘compare mode’, and reported on the number, size, density and location of each stone at both studies for each patient.
Statistical analysis
The SDCT scan was considered as the control for each patient, and the readings of the LDCT scan were compared using Student’s t-test. The results of the statistical tests were considered significant at P < 0.05.
Ethical considerations
Fully informed consent was obtained from all patients and the local ethical committee approved the study. Authors received no funds and have no conflict of interest to declare.
Results
The characteristics of the stones on the unoperated side are shown in . Stones were located in the right and left sides in 27 and 23 patients, respectively. In all, 35 patients had a single stone while the remaining 15 had multiple stones. With SDCT, 95 stones were detected and their size is given in . There were 45 stones of ⩽5 mm, 46 of 6–15 mm and only four of >15 mm. LDCT barely detected three stones of <3 mm, compared with SDCT ( and ), while larger stones had the same appearance on both scans ( and ). The site of the stone in the kidney or the ureter did not affect its detection in LDCT in comparison to SDCT.
Figure 1 Non-contrast CT of the kidneys shows a hyperdense small stone (2 mm) at the left middle calyx, which was adequately visualised on SDCT (b) better than on LDCT (a).
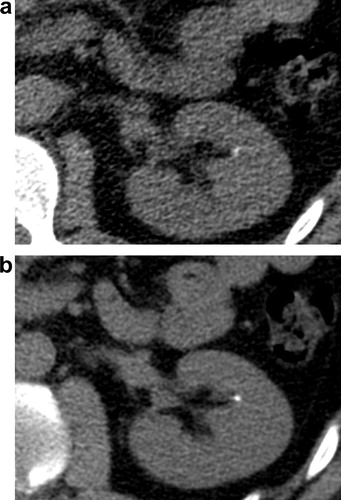
Figure 2 Non-contrast CT of the kidneys shows a hyperdense stone (8 mm) at the left middle calyx, with adequate visualisation on both SDCT (a) and LDCT (b).
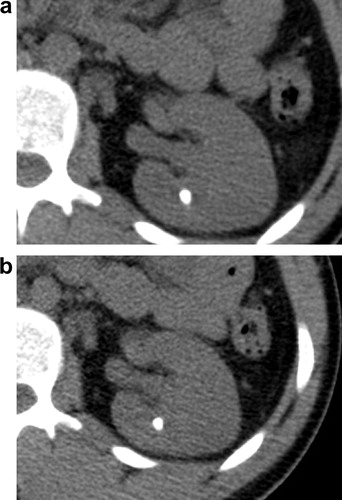
Table 1 Characteristics of the stones on the unoperated side.
Table 2 The distribution of renal stones according to the size.
A comparison between the variables of SDCT and LDCT is shown in . The mean stone diameter was identical with both techniques. At LDCT, all stones were detected with no difference in their number, location or density compared with SDCT. However, the tube current and radiation dose were significantly lower with LDCT.
Table 3 A comparison of different findings at SDCT and LDCT.
Discussion
In this study we compared LDCT and SDCT in obese patients with stone disease. The radiation dose was significantly lower with LDCT than SDCT. With both protocols there were no statistically significant differences in stone size, side, site, number, density and diameter. Only three stones of <3 mm were barely detected with LDCT, in comparison to SDCT.
Stone disease usually affects younger people and has a tendency to recur. Patients can undergo helical CT of the abdomen and pelvis many times, and thus the use of radiation in these patients should be judicious [Citation14].
Denton et al. [Citation22] raised the concern of a greater radiation dose with helical CT than with conventional IVU. They found that the average effective dose of unenhanced helical CT was more than three times that of three-film IVU. The mean effective dose for an IVU examination is reported as 2.6 mSv [Citation23], while the estimated effective dose for SDCT is 8–16 mSv and for LDCT is 0.7–2.8 mSv [Citation24,Citation25].
Niemann et al. [Citation21] stated that the effects of CT dose reduction in obese patients remain unclear. With the current use of automatic tube-current modulation techniques, concepts of absolute effective dose reduction are difficult to apply in all patients because of differences in the BMI of patients. Some authors [Citation20] reported that patients with a BMI of >31 kg/m2 should not undergo LDCT to assess ureteric calculi. Poletti et al. [Citation17] studied LDCT vs. SDCT in 13 patients with suspected renal colic and a BMI of ⩾30 kg/m2, and their results support the observation of the previous study.
In the present study, the mean reduced radiation dose was 5 mSv, which is higher than in the previously reported reduced-dose protocols. We used variable tube current to obtain half of the radiation dose from the automated dose generated at SDCT, while previous studies used a fixed low tube current. In our study we modified the dose according to body weight and this yielded an acceptable image quality that allowed a high diagnostic accuracy (100%) in our patients.
LDCT has some disadvantages in the acute-care setting with stones of <3 mm in diameter, and is less accurate for determining stone size than SDCT [Citation17,Citation18]. In our study, all stones were detected with the LDCT technique, when compared with SDCT.
We measured stone density at both SDCT and LDCT, and all stones showed insignificant changes. The LDCT scan did not affect stone detection due to the great difference between the stone density and adjacent tissue.
SDCT is the most accurate for assessing ureteric stones; this technique is probably the most appropriate method of reference for comparative studies [Citation26–Citation28]. In our study all ureteric stones were detected accurately, but all the ureteric stones were >3 mm in diameter. The site of calyceal stones made no difference in their detection with both the protocols.
To the best of our knowledge, our study is the first to assess the two methods applied routinely during the patient’s examination, unlike other studies that expose the patients to unnecessary radiation, use a phantom, or use software modulation of the radiation.
The limitation of our study is that relatively few patients were included, and that we were aware of the results of SDCT when reading the LDCT scan.
According to our results, we recommend using unenhanced LDCT (50% dose reduction) for obese patients with stone disease, especially during the follow-up after treatment, for detecting residual or recurrent stones. This protocol allows an examination of the patients with a radiation dose as low as that of IVU, and with high accuracy in comparison to SDCT. Further evaluation is recommended to study the effect of a further dose reduction and the effect of stone composition on stone density at LDCT.
In conclusion, the results of this study suggest that LDCT (using 50% dose reduction) is as accurate as SDCT for stone detection, and for evaluating size, density, number and location in obese patients with a BMI of >30 kg/m2. It is better to use LDCT in the follow-up of stone disease, but SDCT is still required until a multi-centre large series is evaluated to confirm the accuracy of LDCT.
Conflict of interest
The authors have no conflict of interest.
Notes
Peer review under responsibility of Arab Association of Urology.
References
- O.W.MoeKidney stones. Pathophysiology and medical managementLancet3672006333344
- C.Y.PakKidney stonesLancet351199817971801
- A.TrinchieriF.OstiniR.NespoliF.RoveraE.MontanariG.ZanettiA prospective study of recurrence rate and risk factors for recurrence after a first renal stoneJ Urol16219992730
- J.W.SutherlandJ.H.ParksF.L.CoeRecurrence after a single renal stone in a community practiceMiner Electrolyte Metab111985267269
- S.AbramsonN.WaldersK.E.ApplegateR.C.GilkesonM.R.RobbinImpact in the emergency department unenhanced CT on diagnostic confidence and therapeutic efficacy in patients with suspected renal colic: a prospective surveyAJR175200016891695
- J.M.TeichmanClinical practice: acute renal colic from ureteral calculusN Engl J Med3502004684693
- R.C.SmithM.VergaS.McCarthyA.T.RosenfieldDiagnosis of acute flank pain: value of unenhanced helical CTAJR166199697101
- P.W.WiestJ.A.LockenP.H.HeintzF.A.MettlerJrCT scanning. A major source of radiation exposureSemin Ultrasound CT MRI232002402410
- D.J.BrennerE.J.HallComputed tomography – an increasing source of radiation exposureN Engl J Med357200722772284
- R.SierakowskiB.FinlaysonR.R.LandesC.D.FinlaysonN.SierakowskiThe frequency of urolithiasis in hospital discharge diagnoses in the United StatesInvest Urol151978438441
- D.S.KatzN.VenkataramananS.NapelF.G.SommerCan low-dose unenhanced multidetector CT be used for routine evaluation of suspected renal colic?AJR1802003313315
- D.H.JinG.R.LambertonD.R.BroomeH.P.SaatyS.BhattacharyaT.U.LindleretalEffect of reduced radiation CT protocols on the detection of renal calculiRadiology2552010100107
- E.K.PaulsonC.WeaverL.M.HoL.MartinJ.LiJ.DarsieetalConventional and reduced radiation dose of 16-MDCT for detection of nephrolithiasis and ureterolithiasisAJR1902008151157
- J.P.HeneghanK.A.McGuireR.A.LederD.M.DeLongT.YoshizumiR.C.NelsonHelical CT for nephrolithiasis and ureterolithiasis: comparison of conventional and reduced radiation-dose techniquesRadiology2292003575580
- B.S.KimI.K.HwangY.W.ChoiS.NamkungH.C.KimW.C.HwangetalLow-dose and standard-dose unenhanced helical computed tomography for the assessment of acute renal colic: prospective comparative studyActa Radiol462005756763
- T.H.MulkensS.DaineffeR.De WijngaertP.BellinckA.LeonardG.SmetetalUrinary stone disease: comparison of standard dose and low-dose with 4D MDCT tube current modulationAJR1882007553562
- P.A.PolettiA.PlatonO.T.RutschmannF.R.SchmidlinC.E.IselinC.D.BeckerLow dose versus standard-dose CT protocol in patients with clinically suspected renal colicAJR1882007927933
- B.KarmazynD.P.FrushK.E.ApplegateC.MaxfieldM.D.CohenR.P.JonesCT with a computer-simulated dose reduction technique for detection of pediatric nephroureterolithiasis: comparison of standard and reduced radiation dosesAJR1922009143149
- M.K.KalraM.M.MaherT.L.TothB.SchmidtB.L.WestermanH.T.MorganStrategies for CT dose optimizationRadiology2302004619628
- M.HammE.KnopfleS.WartenbergF.WawroschekD.WeckermannR.HarzmannLow dose unenhanced helical computerized tomography for the evaluation of acute flank painJ Urol167200216871691
- T.NiemannM.Van StratenC.ResingerT.BayerG.BongartzDetection of urolithiasis using low-dose CT – a noise simulation studyEur J Radiol802011213218
- E.R.DentonA.MackenzieT.GreenwellR.PopertS.C.RankinUnenhanced helical CT for renal colic: is the radiation dose justifiable?Clin Radiol541999444447
- E.YakoumakisI.A.TsalafoutasD.NikolaouI.NazosE.KoulentianosC.ProukakisDifferences in effective dose estimation from dose–area product and entrance surface dose measurements in intravenous urographyBr J Radiol742001727734
- M.CohnenL.J.PollC.PuettmannK.EwenA.SalehU.MödderEffective doses in standard protocols for multi-slice CT scanningEur Radiol13200311481153
- K.FujiiT.AoyamaC.Yamauchi-KawauraS.KoyamaM.YamauchiS.KoetalRadiation dose evaluation in 64-slice CT examinations with adult and paediatric anthropomorphic phantomsBr J Radiol82200910101018
- L.Dalla PalmaR.Pozzi-MucelliF.StaculPresent-day imaging of patients with renal colicEur Radiol112001417
- B.E.Van BeersS.DechambreP.HulcelleR.MaterneJ.JamartValue of multislice helical CT scans and maximum-intensity-projection images to improve detection of ureteral stones at abdominal radiographyAJR177200111171121
- D.H.SheaforB.S.HertzbergK.S.FreedB.A.CarrollM.T.KeoganE.K.PaulsonetalNonenhanced helical CT and US in the emergency evaluation of patients with renal colic: prospective comparisonRadiology2172000792797