Abstract
Objective:To study the natural history of stone passage in children with ureterolithiasis and to define factors predictive of spontaneous passage.
Patients and methods: In all, 72 children with ureteric stones were evaluated; patients with ureteric calculi of >10 mm were excluded, as were those with absolute indications for surgical stone removal. Stone size, location, side, presence of hydronephrosis, perinephric stranding and degree of the tissue-rim sign were estimated by unenhanced helical computed tomography (UHCT). All patients were sent home with no administration of an α-blocker. The stone status was evaluated by a plain abdominal film or CT at ≈6 weeks after the initial diagnostic evaluation. The time from the initial complaint to the passage of the stone was recorded for each patient.
Results: In all, 54 (75%) children with ureteric stones of ⩽6 mm eventually passed their stones spontaneously. However, stones of <4 mm and those in the distal ureter had a significantly higher spontaneous passage rate and shorter time to stone passage (P < 0.05). The UHCT findings of a higher degree of the tissue-rim sign, hydronephrosis and perinephric fat stranding were associated with a lower likelihood of stone passage.
Conclusions: The rate of spontaneous passage of ureteric stones in children varies with stone location, and perinephric stranding on UHCT seems to be useful for predicting the possibility of spontaneous passage. In cases with unfavourable signs an early intervention might have better outcomes than conservative therapy.
Keywords:
Abbreviations:
Introduction
The efficient treatment of ureteric calculi in children has generally been considered as challenging. Although there are many procedures for treating ureteric stones some patients pass stones with no intervention [Citation1]. The widespread availability of ESWL and ureteroscopy has expanded the indications for interventions to treat ureteric calculi [Citation2], but these procedures are not without risk, inconvenience and expense.
Factors such as calculus location and size, the degree of hydronephrosis and pain, and perinephric stranding have been shown to provide general predictions of the probability and duration of passage [Citation3, Citation4] . These characteristics allow the urologist to provide the patient with a general prediction of the outcomes.
Previous similar studies focused on the effect of stone size and location on the natural history of ureteric stone passage, but in the presence of several confounding factors, e.g. hydronephrosis, peri-ureteric oedema and stone impaction, an accurate estimate of the fate of calculi is difficult to obtain.
In general, stones of <5 mm have a spontaneous passage rate of 50–95%, especially if they are in the distal ureter. However, stones of 5–10 mm have a spontaneous passage rate of 10–50% depending on the portion of the ureter in which they are located [Citation5].
Coll et al. [Citation3] suggested that the rate of spontaneous passage of a stone is related to its position in the ureter, with 75% in the distal, 60% in the middle and 50% in the proximal ureter. Of children with a stone in the ureter, 25–50% might need a surgical procedure, for which ureteroscopy is an excellent method [Citation6].
Unenhanced helical CT (UHCT) is now used almost exclusively for the diagnosis and treatment of patients with acute ureterolithiasis [Citation7]. CT can show almost all stones regardless of composition, including uric acid stones that are typically radiolucent on radiography. Given the important role of UHCT in the diagnosis and treatment of children with acute ureterolithiasis, it is important to determine the relationship of spontaneous passage of ureteric calculi and imaging findings.
The parents’ and physician’s decision for intervention is influenced by many factors, including the likelihood and time to stone passage, pain and narcotic requirements, family commitments and preference. We conducted a prospective study to determine the natural history of stone passage in children with ureterolithiasis and to define factors predictive of spontaneous passage.
Patients and methods
Between April 2007 and December 2010, 72 children with ureteric stones were evaluated for spontaneous passage of their stones in a prospective study. The inclusion criteria were age <18 years and flank pain with or without microhaematuria (>3 red blood cells per high-power field). Excluded were those aged >18 years, or with any underlying anatomical abnormality of the urinary tract, and patients with absolute indications for surgical stone removal (which included infection, severe obstruction, renal impairment and uncontrollable pain). Patients with ureteric calculi of >10 mm were also excluded due to the significantly lower chance of spontaneous stone passage.
Diagnosis
Ureterolithiasis was diagnosed only if there was unequivocal evidence on UHCT. Distal ureteric stones were defined as those below the sacroiliac joints, and impacted stones were defined as calculi remaining in the same position for >2 months. The stone size reported was the dimension perpendicular to the long axis of the ureter.
The duration of impaction was determined by patient history and/or previous radiographs. The stone size, location, side, presence of hydronephrosis, perinephric stranding and degree of tissue rim sign (TRS) were estimated by UHCT. Clinical data included patient gender and age, stone size, location and impaction, and the interval to stone passage.
UHCT for predicting stone passage
To assess the role of the UHCT in predicting the clearance of ureteric stones, the presence of the TRS, perinephric-fat stranding and hydronephrosis were evaluated. A positive TRS [Citation8] was defined as annular soft-tissue attenuation (20–40 Hounsfield units) caused by an oedematous ureteric wall surrounding the stone () and it was graded as I (absent or soft-tissue attenuation diameter <2 mm) or II (soft-tissue attenuation diameter ⩾2 mm). The perinephric fat stranding [Citation8] was defined as linear areas of soft-tissue attenuation in the perinephric space () and was graded as I (absent or a few thin strands) and II (many thick strands). Hydronephrosis [Citation9] was graded as I (absent or prominence of the intrarenal pelvis or mild dilatation of the ureter) or II (moderate to marked dilatation of the renal calyces or the ureter).
Figure 1 An axial image of UHCT of a 14-year-old girl, showing a TRS.
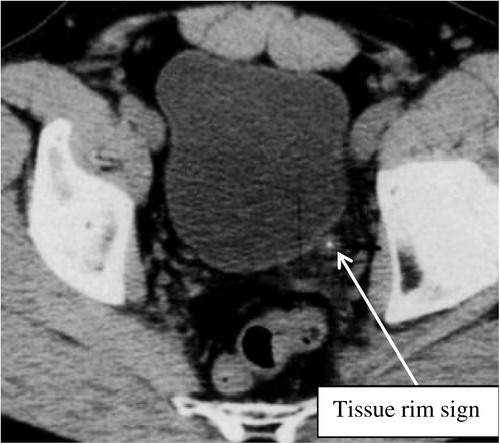
Figure 2 An axial image of UHCT showing perinephric stranding.

Follow-up
All patients were sent home with no administration of an α-blocker, and were assessed every 2 weeks until spontaneous stone passage or intervention. The follow-up consisted of a genitourinary history with the emphasis on pain, narcotic requirements, stone passage or recovery, physical examination and urine analysis. Patients were assessed by plain radiography at every visit. The interval to stone passage was estimated for each patient. The stone status was evaluated by a plain abdominal film or CT at ≈6 weeks after the initial stone episode. The time from the initial episode of colic to the incidence of stone passage was recorded for each patient. The time for spontaneous passage was defined as the day the patient reported the passage of a stone and the report was confirmed by absence of the radio-opaque calculi shadow on the plain film.
If after a 6-week follow-up the stone failed to pass spontaneously, pain was uncontrolled by therapy, fever appeared, or severe hydronephrosis occurred, a decision of active intervention was taken.
Statistical analysis
To assess the value of stone characteristics and the secondary signs on UHCT in the prediction of stone passage, the chi-square test and Fisher’s exact tests were used, with P < 0.05 considered to indicate statistical significance. Multivariate logistic regression analysis of these predictors was then used to identify the most statistically significant predictors of stone passage.
Results
The mean (range) age of the 72 patients was 7 (4–16) years and there were 44 boys and 28 girls. Thirty-nine stones were in the right ureter and 33 in the left; the mean (range) stone diameter was 4.26(2–10) mm.
In all, 54 patients (75%) passed their stones during the follow-up period, and children who did not pass their stone were treated by ureteroscopic stone removal. All of the stones were radio-opaque. Age, gender and stone laterality had no significant effect on the stone passage rate.
The relationship of stone size (in 2-mm increments) to the frequency of spontaneous passage and time to stone passage is shown in . The number of stones of each size is also indicated. The overall frequency of spontaneous passage for stones of 1–4 mm in diameter was 95%. This was associated with shorter interval to stone passage among this group. These differences were statistically significant (P < 0.05).
Table 1 Spontaneous passage frequency and average time to stone passage as a function of stone size and location.
also shows the relationship of stone location to the overall frequency of spontaneous passage. These differences in overall frequency were statistically significant for stones in the distal ureter (P < 0.05), which also had a statistically significantly shorter interval to stone passage than mid-ureteric and proximal stones.
The secondary signs on UHCT were assessed in relation to stone passage at the end of the follow-up period. The degree of the TRS, perinephric-fat stranding and hydronephrosis tended to be more severe in patients who failed to show progress in stone passage, and were significantly more severe in children who needed surgical intervention than in those who passed their stone spontaneously ().
Table 2 The effect of the secondary signs of UHCT on stone passage.
The factors affecting stone passage were entered in a stepwise logistic regression model to find the most significant factor affecting stone passage; the model showed significance (model chi-square P < 0.001). Of the factors assessed in the model (age, gender, stone size, stone location, TRS grade, perinephric-stranding grade, hydronephrosis grade) only two were significant for stone passage, i.e. perinephric stranding grade and stone location (adjusted odds ratio 39.8 and 35.5, respectively). The other factors were contributory risk factors to stone passage but were not significant ().
Table 3 Multivariate logistic regression analysis of the predictors of stone passage.
Discussion
For urologists managing patients with ureteric stones the uncertainties about how long (if at all) it will take for a stone to pass spontaneously is a common concern. The present study attempted to answer this question by raising awareness that secondary signs on UHCT can be used to predict the spontaneous passage of ureteric stones in children.
Treatment options for ureteric stones in children include conservative measures, e.g. ESWL and ureteroscopic stone extraction [Citation10]. The critical decision in the management of children with ureteric stone, in the absence of absolute indications for immediate stone removal, is how long to wait for the stone to pass spontaneously before surgical intervention.
Although guidelines have already standardised the treatment of adults with stones there is still no consensus on the natural history and management of paediatric urolithiasis. It has long been appreciated that children can pass relatively large stones, compared to those in adults [Citation11], but published data do not include many results on children. To assist parents in making an informed decision about intervention vs. observation, the likelihood of success and the interval to passage of observed ureteric calculi were evaluated.
UHCT is a well-established procedure for diagnosing urolithiasis, with a high sensitivity and specificity [Citation12]. Due to the high stone recurrence rate in children, those with stones might have many CT sessions in childhood, with frequent exposure to radiation, although recently developed CT protocols might further reduce the exposure to radiation [Citation13]. However, the radiation dose and the extent of information about renal function must be considered when using UHCT in children.
In the present study every attempt was made to allow patients to pass ureteric stones spontaneously. Each patient was followed every 2 weeks or as needed, until passage or intervention. Observation was encouraged and the mean interval before intervention was 26 days. These values reflect parent desire, failure to progress and pain, with none of these patients having renal impairment. If some of these patients had been followed further they might have passed stones spontaneously.
Reported spontaneous passage rates for ureteric stones vary widely. Several large series assessing ureteric calculi have determined the probability of spontaneous stone passage. In a series of 378 ureteric calculi, Morse and Resnick [Citation14] noted a 60% spontaneous passage rate, including 71% of distal stones and 78% of stones of ⩽3 mm.
Hubner et al. [Citation15] combined two studies with four others in a literature review, and reported a rate of spontaneous passage of 56.9% for ureteric stones of <4 mm vs. 8.3% for those >6 mm, irrespective of ureteric position at presentation. After this review and the evaluation of their last 100 patients they also believed that intervention should be considered when symptoms are present for 4 weeks, because stone passage is unlikely after that time.
There is total agreement that stone size is the most important factor for predicting the spontaneous passage of calculi [Citation16]. However, this does not seem to be discriminative enough when calculi are of mid-size. At this stage the urologist needs more information to make a valid clinical decision, but there is no clear result as to which factor should be considered first and what are the important interactions between all the factors [Citation17].
Since Smith et al. [Citation8] first reported the use of UHCT in patients with ureteric stones the value of secondary signs associated with ureteric stones, e.g. hydronephrosis, unilateral renal enlargement, perinephric oedema, unilateral absence of the white pyramid, hydroureter, peri-ureteric oedema, and lateroconal fascial thickening, have been well established.
Ege et al. [Citation9] reported that the detection of secondary signs on UHCT allowed a prediction of the clinical outcome. They suggested that five or more secondary signs of obstruction are likely to be associated with the need for endoscopic removal and/or lithotripsy. Song et al. [Citation18] studied whether secondary signs on UHCT could predict the spontaneous passage of ureteric calculi, and they concluded that the degree of hydronephrosis and perinephric oedema were useful ancillary signs in predicting the likelihood of spontaneous passage.
Multivariate analysis showed that patient gender, age, stone size, TRS and degree of hydronephrosis were unrelated to stone passage. Together, stone location and perinephric stranding grade were statistically related to stone passage (P = 0.001). Stones that were distal and not associated with perinephric stranding were more likely to pass spontaneously and require fewer interventions.
The present study has the advantage of analysing the effect on stone passage of secondary signs associated with ureteric stones on UHCT. The increased degree of TRS and hydronephrosis were useful for anticipating the failure of spontaneous passage and the need for active intervention.
There are some potential limitations of the present study. The grading system used for secondary signs of obstruction as determined by UHCT is not a standardized system, and there were relatively few patients in the study. Despite these limitations, this study raises awareness that the secondary signs on UHCT can be used to predict the spontaneous passage of ureteric stones in children. Therefore, even in small distal ureteric stones of <5 mm, if secondary signs such as high degree of TRS and hydronephrosis are identified on UHCT, early intervention seems to be better than prolonged conservative management, to avoid the potential risk of UTI or deterioration of renal function.
In conclusion, the rate of spontaneous passage of ureteric stones in children is variable, with stone location and secondary signs on UHCT, especially perinephric stranding, seem to be useful in predicting the possibility of spontaneous passage. In those cases with unfavourable signs, early intervention might have better outcomes than conservative therapy.
Conflict of interest
No conflict of interest to declare.
Source of funding
None.
Notes
Peer review under responsibility of Arab Association of Urology.
References
- J.W.SeguraG.M.PremingerD.G.AssimosS.P.DretlerR.I.KahnJ.E.LingemanetalUreteral Stones Clinical Guidelines Panel summary report on the management of ureteral calculiJ Urol158199719151921
- M.E.HassounaS.OrabW.SamehA.El-AbbadyClinical experience with shock-wave lithotripsy using the Siemens Modularis Vario lithotripterArab J Urol92011101105
- D.M.CollM.J.VaranelliR.C.SmithRelationship of spontaneous passage of ureteral calculi to stone size and location as revealed by unenhanced helical CTAJR Am J Roentgenol1782002101103
- N.TakahashiA.KawashimaR.D.ErnstI.C.BoridyS.M.GoldmanG.S.BensonetalUreterolithiasis: can clinical outcome be predicted with unenhanced helical CT?Radiology208199897102
- M.GettmanJ.SeguraManagement of ureteric stones: issues and controversiesBr J Urol95S220058593
- M.De DominicisE.MatarazzoN.CapozzaG.ColluraP.CaioneRetrograde ureteroscopy for distal stone removal in childrenBr J Urol95200510491052
- R.C.SmithM.VergaS.M.McCarthyA.T.RosenfieldDiagnosis of acute flank pain: value of unenhanced helical CTAJR166199697101
- R.C.SmithM.VergaN.DalrympleS.McCarthyA.T.RosenfieldAcute ureteral obstruction. Value of secondary signs of helical unenhanced CTAJR Am J Roentgenol167199611091113
- G.EgeH.AkmanK.KuzucuS.YildizAcute ureterolithiasis. Incidence of secondary signs on unenhanced helical CT and influence on patient managementClin Radiol582003990994
- J.G.Van SavageL.G.PalancaR.D.AndersenG.S.RaoB.L.SlaughenhouptTreatment of distal ureteric stones in children: similarities to the American Urological Association guidelines in adultsJ Urol164200010891093
- E.MinevichC.A.SheldonThe role of ureteroscopy in paediatric urologyCurr Opin Urol162006295298
- E.P.TammP.M.SilvermannW.P.ShumanEvaluation of the patient with flank pain and possible ureteral calculusRadiology2282003319326
- D.D.CodyD.M.MoxleyK.T.KrughJ.C.O’DanielL.K.WagnerF.EftekhariStrategies for formulating appropriate MDCT techniques when imaging the chest, abdomen, and pelvis in pediatric patientsAJR Am J Roentgenol1822004849859
- R.M.MorseM.I.ResnickUreteral calculi. Natural history and treatment in an era of advanced technologyJ Urol1451991263265
- W.A.HubnerP.IrbyM.L.StollerNatural history and current concepts for the treatment of small ureteral calculiEur Urol241993172176
- T.AnagnostuD.TolleyManagement of ureteric stonesEur Urol452004714721
- O.F.MillerC.J.KaneTime to stone passage for observed ureteral calculi: a guide for patient educationJ Urol1621999688690
- D.W.SongT.Y.JeongS.I.LeeD.J.KimPredicting factors for spontaneous passage of ureteral calculi based on unenhanced helical CT findingsKorean J Urol49200810941099