Abstract
Objective: To report our experience of phalloplasty using a radial forearm free-flap (RFF) and insertion of a penile prosthesis for the amputated phallus.
Patients and methods: Phalloplasty was carried out in nine intersex patients with ambiguous genitalia as a result of female circumcision, with a consequent partial or complete excision of theirmicrophallus. Sixmonths later a penile prosthesiswas inserted in the periostium of the lower border of the symphysis pubis in the first six patients.
Results: All patients were fully satisfied with the size and cosmetic appearance of their penis. One patient had a urinary fistula that was closed surgically. All of the patients are continent. The penile prosthesiswas implanted successfullywith no complications.
Conclusions: Phalloplasty using a RFF and insertion of a penile prosthesis for the amputated phallus are technically feasible, with good clinical and functional outcomes.
Abbreviations:
Introduction
Some families in Upper Egypt perform female circumcision by excising part of the labium minor and clitoris during early childhood. If this is done in patients with an intersex condition and reared as females the micropenis will be excised, resulting in a major problem, particularly after puberty.
Since the first report Bogoras [Citation1] in 1936 of the construction of a neophallus in a patient with an amputated penis, by using an abdominal pedicle flap, there has been continuous development and improvement of such operative techniques. Many types of free flaps have been described, such as the musculocutaneous latissimus dorsi free flap and osteocutaneous free-fibula flap [Citation2, Citation3] . Chang and Hwang [Citation4] popularised the radial forearm free-flap (RFF) in 1984. Currently there are no controlled randomised prospective studies available to confirm if the RFF is the ‘gold standard’ for penile reconstruction; in the present study we present data to support the use of the RFF phalloplasty as a reliable technique for creating a normal-looking penis. We also present the feasibility of both phalloplasty and urethroplasty in one stage, and the insertion of a penile prosthesis at 6 months after surgery in intersex patients who have no micropenis.
Patients and methods
From 2001 to 2010, nine patients (aged from 14–18 years) were operated to create a neophallus. The presenting symptoms were male psychological behaviour, ejaculation with sexual excitation, the appearance of a testicular bulge in the inguinal region and primary amenorrhoea. On clinical examination they were confirmed to be male pseudohermaphrodites ().
Figure 1 A male pseudo-hermaphrodite with an amputated phallus.

Abdominal ultrasonography, CT and diagnostic laparoscopy were used to detect Müllerian organs. All patients also had a chromosomal analysis that confirmed them to be normal males. All patients were also evaluated by a psychiatrist.
Informed consent was obtained from the patients and their parents, and the procedure was approved by the ethical committee of the Faculty of Medicine, Assiut University.
Surgical technique
Two teams operated simultaneously. The urological team prepared the proximal urethral stump, with de-gloving of the amputated penis, excision of the chordae, orchidopexy and scrotoplasty. Finally, a percutaneous suprapubic tube was placed.
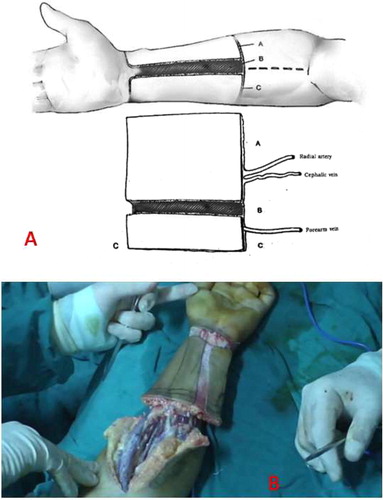
The microsurgical team prepared the flap. Under tourniquet control, a RFF (11 cm long and 13 cm wide) was planned on the volar surface of the left forearm. A strip of skin 1 cm wide along the axis of the flap was de-epithelialised, dividing the flap into an ulnar part (3 cm wide) which would be the neo-urethra, and a radial part (9 cm wide), which would be the penile skin. The flap was raised with the radial artery, one superficial vein and the terminal branch of the lateral cutaneous nerve of the forearm (A and B).
Figure 2 A,B; The RFF planned on the volar surface of the left forearm. The flap is raised with the radial artery, one superficial vein and the terminal branch of the lateral cutaneous nerve of the forearm.
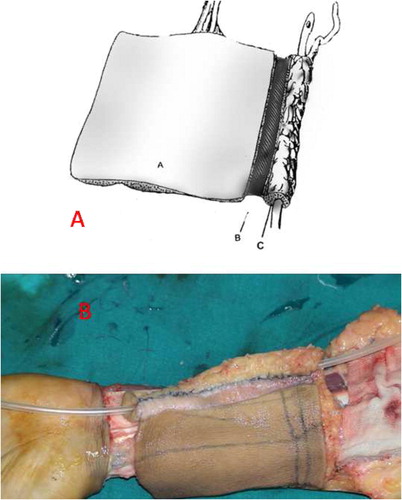
The ulnar part of the flap was rolled around a silicone catheter so that the skin surface faced inside, and the skin edge was sutured to the ulnar side of the de-epithelialised area, thus forming the neo-urethra (A and B).
Figure 3 A,B; The ulnar part of the flap is rolled around. The skin surface faces inside, forming the neourethra.
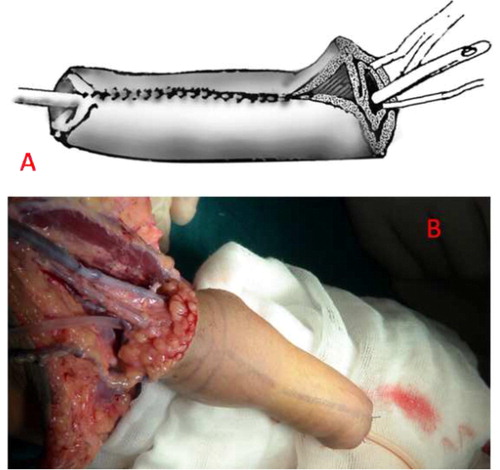
The radial part of the flap was then rolled around the neo-urethra so that skin surface faced outwards and the two subcutaneous surfaces were opposed together (A and B). The skin edges formed the border of the flap around the neo-urethral meatus. The tourniquet was then deflated and the flap allowed to perfuse. The recipient side in the medial surface of the upper left thigh was dissected to prepare the recipient vessels (the profunda femoris artery and great saphenous vein) and the recipient nerve (the medial cutaneous nerve of the thigh).
Figure 4 A,B. The radial part of the flap is rolled around the neo-urethra with the skin surface facing outwards.
The new penis was then transferred and a catheter passed into the proximal urethral stump. The proximal edge of the reconstructed penile skin was sutured to the perineal skin, incorporating the remaining corporal tissue.
The neurovascular bundle was then passed into the skin tunnel to reach the medial surface of the thigh. The neurovascular anastomosis was then made with 10/0 monofilament Nylon using an operating microscope. After vascular and nerve anastomosis the bare segment of the amputated penis was buried by the wide tube of the flap; the new urethra was anastomosed to the proximal urethral tube using 4/0 polyglactin, and the surrounding skin was sutured to the skin using 3/0 polyglactin. The bare area of forearm was covered by a partial-thickness skin graft taken from the thigh.
At 6–18 months after the phalloplasty, a penile semi-rigid prosthesis was implanted to the new phallus in six patients. The dorsal tube in the phallus was dilated to permit the insertion of the prosthesis, which was covered by a PTFE mesh before fixation to the periostium of the lower border of the symphysis pubis (). The mean (range) follow-up was 4 (1–10) years.
Figure 5 Insertion of the penile prosthesis into the new phallus.

Results
The mean operative duration was 8 h and no anaesthetic complications were recorded. No operative complications were reported during the orchidopexy, urethral reconstruction and scrotoplasty. The remaining penile shaft after de-gloving of the penis and excising the chordae was 2–3 cm long. No vascular complications were reported and the flap survived successfully in all cases. There were no complications related to the donor area.
The closed suprapubic tube was removed after the urethral catheter was removed (21 days) and all patients voided well. The hospital stay was 3 weeks to 1 month. The length of the new phallus was 11–15 cm and all patients were fully satisfied with the size and cosmetic appearance of their penis. All patients reported tactile sensational perception at 6–12 months after surgery.
Eight patients had satisfactory voiding with regard to the force and direction of the urinary stream, with no dysuria, incontinence or postvoid residual urine. One patient had a urinary fistula at the junction of the phallus and the scrotum, which was closed surgically. The prosthesis was implanted successfully with no complications in the six patients, with a satisfactory cosmetic and functional outcome ().
Figure 6 The new phallus with a semi-rigid prosthesis implanted inside.

Discussion
All the present patients were confirmed as males by karyotyping and male sexual behaviour, but had suffered an amputation of their phallus as a result of a misdiagnosis of ambiguous genitalia at birth. We performed both the phalloplasty and urethroplasty in one stage, with no complications apart from one urethral fistula. The penile prosthesis was implanted successfully at 6 months after the initial surgery, and all patients were satisfied with the cosmetic and functional outcome.
Different techniques have been used for penile reconstruction in patients with partial or complete amputation of the penis, caused by an animal bite or after trauma or cancer excision [Citation5]. The criteria for assessing the success of penile reconstruction can be summarised as follows; (i) The aesthetic appearance of the neophallus must be as normal as possible; (ii) The penile shaft must contain a urethra, to allow voiding while standing, and with a normal stream; (iii) The penile shaft must allow the implantation of a penile ‘stiffener’ to allow intercourse; (iv) The morbidity of the donor area must be minimal, with an easily concealed scar [Citation6].
The present results were satisfactory during the follow-up, and included an assessment of the length of the phallus, the cosmetic appearance, the function of new urethra, and the donor site scar. The recipient nerve in the present patients was the medial cutaneous nerve of the thigh. All patients reported a good tactile sensation but the erogenous sensibility could not be assessed as they were not yet married. However, our opinion is consistent with Gilbert et al. [Citation7], who stated that the return of erogenous sensation might be a result of ‘dissociated sensibility’, i.e. the ability of the brain to interpret other peripheral stimuli as erogenous. Leriche et al. [Citation8] reported erogenous sensation in only 9% of patients having a complete phalloplasty for female-to-male transsexual surgery, despite incorporating dorsal nerves into the neural anastomosis.
Most of the previous reports considered urethral complications as the major drawback of phalloplasty [Citation6]. In the present series only one patient had a urethral fistula, with no cases of stricture reported.
Inserting a penile prosthesis into the new phallus is a delicate procedure, but the present results showed that it provided good satisfaction and rigidity [Citation9, Citation10] . There were no complications related to interval between phalloplasty and insertion of the prosthesis, and we think that 6 months was sufficient. We used a semi-rigid prosthesis for economic reasons, and to avoid pressure necrosis of the flap, even though the inflatable type is better.
Our technique of phalloplasty is a valuable option for those with penile insufficiency, giving good results in terms of patient self-esteem and sexual well-being. This technique can be used to treat penile agenesis, bladder exstrophy, traumatic amputations and gender reassignments.
The RFF for phalloplasty has some limitations related to the size of the forearm, and difficult flap design in obese patients. In the present study we had to us the medial cutaneous nerve of the thigh, as the cavernous nerve was rudimentary, and this might lead to problems with erogenous sensation. Finally, we recommend that a larger series of patients with different causes of the need for phalloplasty are assessed, to evaluate more clearly the use of the RFF for phalloplasty and urethroplasty.
Conflict of interest
None declared.
Source of funding
There was no extra funding needed.
Notes
Peer review under responsibility of Arab Association of Urology.
References
- N.BogorasUber die volle plastische Wiederherstellung eines zum Koitus fahigen Penis (Peniplastica totalis)Zentralbl. Chir.22193612711276
- M.L.DjordjevicM.Z.BumbasirevicP.M.VukovicS.SansaloneS.V.PerovicMusculocutaneous latissimus dorsi free transfer flap for total phalloplasty in childrenJ. Pediatr. Urol.22006333339
- M.SengezerS.OztürkM.DeveciZ.OdabaşiLong-term follow-up of total penile reconstruction with sensate osteocutaneous free fibula flap in 18 biological male patientsPlast. Reconstr. Surg.1142004439450
- T.S.ChangW.Y.HwangForearm flap in one-stage reconstruction of the penisPlast. Reconstr. Surg.741984251258
- N.LumenS.MonstreyP.CeulemansE.van LaeckeP.HoebekeReconstructive surgery for severe penile inadequacy: phalloplasty with a free radial forearm flap or a pedicled anterolateral thigh flapAdv. Urol.2008704343
- J.L.SempleJ.B.BoydG.A.FarrowM.A.RobinetteThe ‘cricket bat’ flap: a one-stage free forearm flap phalloplastyPlast. Reconstr. Surg.881991514519
- D.A.GilbertM.W.WilliamsC.E.HortonJ.K.TerzisB.H.WinslowD.M.GilbertetalPhallic reinnervation via the pudendal nerveJ. Urol.1401988295299
- A.LericheM.O.TimsitN.Morel-JournelA.BouillotD.DembeleA.RuffionLong-term outcome of forearm flee-flap phalloplasty in the treatment of transsexualismBJU Int.101200812971300
- A.BallaroJ.PryorD.RalphProsthesis implantation after radial free flap phalloplasty in patients with bladder exstrophyInt. J. Impot. Res.111999341342
- J.J.HageDynaflex prosthesis in total phalloplastyPlast. Reconstr. Surg.991997479485