Abstract
Objectives: To evaluate a supracostal approach for percutaneous nephrolithotomy (PCNL) of staghorn calculi through a prospective study and review of previously reported cases.
Methods: From June 2009 to November 2011, 40 patients with staghorn calculi were scheduled for supracostal S-PCNL in a prospective study. Of the 40 renal units, 16 (40%) had a complete staghorn and 24 (60%) had a partial staghorn calculus. Perioperative complications were stratified according to the modified Clavien system. Univariate and multiple logistic regression analyses were used to determine statistically significant variables affecting the stone-free rate and development of complications.
Results: In all, 57 tracts were established in the 40 renal units; 23 (58%) renal units were approached through one supracostal upper pole calyx, while 13 (33%) and four (10%) required a second middle- or lower-pole puncture, respectively. Overall, 78% of patients were rendered stone-free or had clinically insignificant residual fragments with PCNL monotherapy, and this increased to 88% with auxiliary procedures. In the logistic regression analysis, a complete staghorn stone was the only independent variable for residual stones (P = 0.005). There was an overall complication rate of 38%. Independent variables with an influence on complications were staghorn stone burden (P = 0.007), and operative duration (P = 0.045).
Conclusion: The supracostal upper calyceal approach provides optimum access for the percutaneous removal of staghorn stones. Appropriate attention to the technique and to monitoring before and after surgery can detect thoracic complications, and these can be managed easily with intercostal chest tube drainage, with no serious morbidity.
Abbreviation:
Introduction
The AUA Nephrolithiasis Clinical Guidelines panel recommended percutaneous stone removal as the first treatment option for managing staghorn calculi patients [Citation1]. The management strategy for treating staghorn calculi depends on the overall stone burden, location and distribution of the stones, and the anatomy of the collecting system. The success of percutaneous stone removal depends on an adequate choice of the renal calyceal approach. The lower calyx approach fails to provide optimal access to most of the collecting system, and could be traumatic to the renal parenchyma. The superior calyceal approach is considered ideal for approaching the renal system when managing staghorn stones, complex upper and lower calyceal calculi, proximal ureteric calculi, and calculi associated with primary pelvi–ureteric junction obstruction [Citation2–Citation4] . However, many urologists hesitate to use a supracostal approach because of the potential for intrathoracic complications.
The aim of the present study was to evaluate the status of a supracostal upper calyceal access for percutaneous nephrolithotomy (PCNL) when treating staghorn calculi, from both the initial experience and a review of previous reports.
Patients and methods
From June 2009 to November 2011, 40 consecutive patients (28 men and 12 women, mean age 43.2 years, range 16–64) with staghorn calculi were scheduled for supracostal S-PCNL in a prospective case-series study. The study was approved by the local ethics committee, and all patients signed a written informed consent before participating. During the study period, 54 patients with staghorn calculi were assessed for eligibility. The decision to use S-PCNL was based on the stone location, configuration of the intrarenal collecting system, and the likelihood of maximal clearance using a single tract. The exclusion criteria were bleeding tendency, and high-lying kidneys necessitating puncture above the 11th rib. Giant staghorn calculi requiring more than one tract in addition to the supracostal tract, and calculi associated with marked calyceal deformities, were also excluded. The preoperative assessment included routine laboratory studies, e.g., blood chemistry, complete blood count, coagulation profile, urine analysis and urine culture. A radiological evaluation was obtained with multislice non-contrast CT in all patients.
The staghorn stone could be complete (involving the renal pelvis and all calyces) or partial (with branches in two of the three calyceal groups). Of the 40 patients, 16 (40%) had a complete staghorn and 24 (60%) a partial staghorn calculus. The size of the staghorn stone was based on measuring the longest linear diameter observed on a plain film [Citation5]. The mean (range) stone burden was 6.2 (4.5–10.5) cm.
Procedure
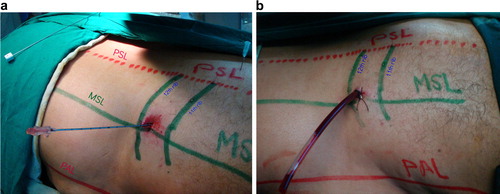
Prophylactic antibiotics were given before surgery in every case. All PCNL was performed as a one-stage procedure under C-arm fluoroscopic guidance. Renal access was determined before the procedure after assessing the stone configuration and intrarenal anatomy of the collecting system. The desired calyx and the upper-pole calyx were punctured and guidewires were fixed before dilatation of any tract. For supracostal upper-pole access, the intercostal space between the 11th and 12th rib was used in all cases. The puncture was made above the lateral half of the 12th rib at the mid-scapular line (a). The needle was advanced in the middle of the intercostal space, thus avoiding the intercostal nerve and vessels. The puncture was made during full expiration, to avoid injury to the lung or pleura. The nephrostomy tract was dilated to 30 F using Alken’s coaxial telescopic dilators. A pneumatic lithotripter was used to disintegrate the stone and any stone fragments removed by grasping forceps. When additional access was required, the Amplatz sheath was left in the upper calyx while working through the second access tract, to prevent excessive extravasation from the upper calyx into the pleural cavity. A 20 or 22 F Nelaton catheter was placed as a nephrostomy tube at the end of the procedure (b). If there was any doubt about complete stone clearance or bleeding from the other tract, an additional nephrostomy tube was placed in that tract. All patients had a nephrostogram taken at the end of surgery, and lung fields were imaged fluoroscopically with the patient prone. A chest radiogram was taken immediately after surgery, On the second day after surgery all had a routine plain film radiography, nephrotomography and ultrasonography to check for residual fragments, leakage and infrarenal obstruction. A second stage, if necessary, was scheduled after 2–3 days.
Figure 1 (a) Landmarks relevant to supracostal access: PSL, paraspinal line; MSL, midscapular line; PAL, posterior axillary line. A small needle points to the upper calyx. The puncture for a supra-12th rib approach at the MSL is in the middle of the intercostal space. (b) The nephrostomy tube placed at conclusion of the procedure.
Follow-up
Perioperative complications were stratified according to the modified Clavien system [Citation6]. The mean (range) follow-up for the entire group was 4.2 (3–6) months. At 30 days after surgery, a plain abdominal film, urinary tract ultrasonography and urine culture were obtained, and at 3 months, patients were assessed using IVU and urine culture. ‘Stone-free’ was defined as the complete absence of stones or the presence of fragments of <5 mm after the primary procedure.
Univariate and multivariate logistic regression analyses were used to identify features predictive of the stone-free rate and of complications, with P < 0.05 considered to indicate statistical significance.
Results
Before surgery, the mean (range) haemoglobin level was 11.8 (10.5–14.5) g/dL, and the serum creatinine level was 1.2 (1.01–3.5) mg/dL. Of the 40 patients, three (8%) had a serum creatinine level of >1.5 mg/dL. In all, 57 tracts were established in 40 renal units. The supracostal was the only access in 23 (58%) renal units, 13 kidneys (33%) required an upper and middle calyceal puncture, while four (10%) required a combined upper- and lower-pole puncture. There were no cases of renal access above the 11th rib. The additional subcostal puncture was made during the initial procedure in 14 (35%) renal units, and during a second session of PCNL in three (8%).
According to the above definition of stone-free, 26 renal units (65%) were treated successfully after one session of PCNL, and 14 (35%) had significant residual stones. Of these 14 renal units, four (10%) required a second session of PCNL, one (2.5%) a third session, and seven (13%) required ESWL. Two patients with significant residual stones of <1 cm were treated by placing a JJ stent and medical expulsive therapy. Thus, 31 renal units (78%) were rendered stone-free or had insignificant residuals after PCNL monotherapy, and this increased to 88% with auxiliary procedures. The patients’ characteristics, stone features and operative variables in relation to the stone-free rate after the initial PCNL procedure are listed in . Univariate analysis showed that the staghorn stone burden was significantly different between the groups (P = 0.006).
Table 1 The univariate analysis of factors affecting the stone-free rate after initial S-PCNL.
Perioperative complications occurred in 15 (38%) procedures, and were categorised according to the modified Clavien classification score (). Intraoperative bleeding was considered significant when causing haemodynamic instability or obscuring proper vision. A blood transfusion was indicated if the haemoglobin and/or haematocrit decreased to <9 g/dL and <27%, respectively. A blood transfusion was needed in four (10%) patients. One patient had persistent bleeding after surgery and was found to have a pseudo-aneurysm, for which angioembolisation was used. Hydrothorax was identified on the operating table by fluoroscopy or by an increase in airway resistance, and in the recovery room on a plain chest film. Patients with hydrothorax were treated by placing a chest tube and an underwater seal. The mean duration of chest drainage was 3.2 days. Pelvicalyceal perforation developed in one patient near to the end of the operation. The procedure was completed and the nephrostomy tube was removed after 5 days, following a nephrostogram. Any perinephric collection was treated with aspiration and by placing a JJ ureteric stent. The patient with sepsis recovered well with intravenous broad-spectrum antibiotics and other supportive measures. Persistent urinary leakage through the site of the nephrostomy was treated by placing a JJ stent. None of the patients developed lung or visceral injury. The mean (range) hospital stay after surgery was 6.8 (3–12) days.
Table 2 Complications of S-PCNL in 40 patients classified according to the modified Clavien system [Citation6].
A univariate analysis for factors affecting the complication rate is shown in . The operative time (P < 0.001) and staghorn stone burden (P < 0.001) were significantly different between the groups. From the logistic regression analysis the independent risk factor for residual stones was a complete staghorn stone (P = 0.005). Independent risk factors for developing complications were a complete staghorn stone (P = 0.007) and prolonged operative duration >140 min (P = 0.045; ).
Table 3 Univariate analysis of factors affecting complications after S-PCNL.
Table 4 Stepwise regression analysis of predictors of the stone-free rate and complications after S-PCNL.
Discussion
The superior calyx is considered ideal for approaching the renal system when managing staghorn calculi because the most posterior portion of the kidney is the posterior upper-pole calyx, and thus it provides the most direct access to the renal pelvis, upper ureter and lower-pole calyces. Even the posterior interpolar calyx can be accessible without significant angulation [Citation7]. The superior calyx lies above the 12th rib most of the time, as on full expiration 80% of right renal upper pole calyces and 85% of left renal upper pole calyces lie above the 12th rib [Citation8].
Preminger et al. [Citation9] reported cephalad movement (averaging 2.2 cm) of the kidney when patients were placed prone rather than supine, as viewed on IVU. Thus direct access to a superior calyx would require a supracostal puncture in >80% of patients.
The anatomy of the kidney in relation to the lung, parietal and visceral pleura, and the diaphragm, is important information to make a safe supracostal access tract [Citation10]. The parietal pleura is reflected to the level of the 10th rib at the mid-axillary line, and posteriorly at various levels along the 12th rib. The diaphragm is attached to the inferior border of the 12th rib, the upper lumbar vertebral anterior surfaces and the transverse process of the first lumbar vertebra. Thus a puncture above the 12th rib must always traverse the diaphragm. An injury to the intercostal artery can lead to the potential complication of haemothorax, and can be avoided by staying in the middle of the intercostal space [Citation5], or immediately above the upper border of the lower rib [Citation11].
The subcostal inferior calyx approach to staghorn stones can induce angulation and torque on the kidney, which can cause trauma and bleeding [Citation12]. Although it is technically more demanding, access through a superior calyx provides a short and straight tract along the axis of the kidney. This ability to operate via the long axis of the kidney causes less torque of the rigid nephroscope, and reduces the chance of injuring the peri-infundibular venous plexus that is possible if angulation of the tract is required to reach the stone-bearing area [Citation13], thereby reducing the chances of excessive bleeding.
While making an upper-calyx access, care should be taken to puncture through the centre of the calyceal papilla, and direct puncture through the infundibulum must be avoided. Sampaio et al. [Citation14] reported injury to an interlobar vessel in two-thirds of kidneys on puncturing the upper-pole infundibulum, while only 13% of kidneys had an arterial injury when accessed through the lower-pole infundibulum. However, when the puncture was through the centre of the calyceal papilla they detected no arterial lesions.
The reported stone-free rates after S-PCNL are variable. The lack of strict criteria to define ‘stone-free’ status, and the use of several imaging methods, might account for some of these variations. The factors related to treatment outcome after PCNL were addressed in recent reports, showing that the overall stone burden, presence or absence of secondary calyceal stones, and degree of hydronephrosis are important prognostic factors [Citation15, Citation16] .
Golijanin et al. [Citation17] reported a retrospective study of 104 patients who underwent 115 S-PCNL to treat 102 complete staghorn calculi, six large semi-staghorn calculi, three large upper calyceal stones and four significant volumes of residual stone fragments after ESWL. Additional renal access was required mainly for complete staghorn stones in 23 (20%) patients. ESWL was needed to treat residual stones in 30.4% and a ‘second-look’ PCNL in 15.6%. The stone free-rate after PCNL was 67.8%, while after PCNL followed by ESWL, second-look PCNL, or both, the stone-free rate increased to 87%.
Gupta et al. [Citation4] reported that 15 of 26 (58%) patients with staghorn calculi also required a middle calyceal puncture, as the middle calyx was difficult to reach from the superior calyx, because of the acute angle between the calyces. The supracostal access was the only access in 11 renal units, and the stones were completely cleared in 22 (85%), of which seven required a repeat PCNL and four patients required ESWL for significant residual stones.
Shaban et al. [Citation18] used PCNL in 11 patients with staghorn stones via two access tracts, one of which was supracostal and the other through the middle or the lower calyx. All renal units were managed in one session of PCNL, eight were rendered stone-free and three required ESWL.
The overall stone-free rate in the present study, at 78% by PCNL monotherapy, is comparable with those reported in previous studies [Citation2,Citation4,Citation7,Citation12,Citation15,Citation17–Citation26] (). A single upper pole puncture was used in 23 (58%) patients, with an additional puncture required in 17 (42%) to remove the middle and lower calyceal extensions, which were difficult to reach through the superior calyceal tract. In the present study, the significant factor that affected the stone-free rate after S-PCNL was the stone burden. The stone-free rate was 63% for complete staghorn stones, while 88% of patients with a partial staghorn were rendered stone-free after S-PCNL monotherapy.
Table 5 A summary of supracostal procedures in previously published studies
A staghorn stone was identified as an independent risk factor for severe bleeding after PCNL [Citation27]. El-Nahas et al. [Citation15] reported that using PCNL for staghorn calculi by urologists other than an experienced endourologist, and a positive preoperative urine culture, were independent risk factors for the development of complications. They proposed strategic factors to maximise the benefits and safety of PCNL for staghorn calculi. Preoperative planning of the number, site and direction of the access tracts should be determined after a thorough evaluation of all radiological studies. The surgeon must gain a balance between complete stone clearance and acceptable patient morbidity. Therefore, when significant complications develop, the procedure should be terminated [Citation28].
The overall complication rate after S-PCNL is 10–26% [Citation17, Citation24] . The major disadvantage of supracostal access is the potential for pleural complications. Hopper et al. [Citation11] used CT with sagittal reconstruction when patients were at both full inspiration and expiration. On expiration the needle path had a 29% chance on the right and a 14% chance on the left of transgressing the pleura, while during forced full inspiration the lung would be in the path of the needle in most patients. During expiration the lower extent of the parietal pleura crosses the 12th rib obliquely, so that the lateral part of the 12th rib lies below and lateral to the lowest limits of the pleura. Injury to the pleura can be avoided by staying above the lateral half of the 12th rib and lateral to the mid-scapular line. However, even when taking all these precautions, in a small proportion of patients the pleura can still be injured. Access through the pleural space can lead to the accumulation of fluid and cause hydrothorax, requiring the insertion of a chest tube.
Gupta et al. [Citation4] reported 63 supracostal access procedures, with 14 (22%) sustaining overall complications. Chest complications developed in seven (11%) patients, three with minimal blunting of the costophrenic angle, managed conservatively, while significant hydrothorax and haemothorax occurred in three and one patient, respectively, who were treated with chest drains.
Munver et al. [Citation2] reported an overall complication rate of 16% (16/98 tracts) for supracostal punctures, and 4.5% for subcostal tracts. Of the 98 supracostal punctures, 26 (27%) were above the 11th rib and 72 (73%) above the 12th rib. The complication rate was 35% for punctures above the 11th rib and 10% for those above the 12th rib. The overall risk of intrathoracic complications for a puncture above the 11th rib was 23%, vs. 1.4% for that above the 12th rib. Munver et al. recommended avoiding a puncture above the 11th rib, to minimise complications. The risk of bleeding that required a transfusion after puncture was 4.1%, although the risk of bleeding with a puncture above the 11th rib was no higher than for other puncture sites. Other series reported transfusion rates of 0–20% [Citation17, Citation24] .
The non-thoracic complication rate of 28% and transfusion rate of 10% in the present study are similar to those in other reported series (). Overall, the occurrence of hydrothorax (10%) was comparable with that in earlier studies (1.7–15%; ). Supra-11th rib access has been reported to have a 16 times greater risk of intrathoracic complications than a supra-12th rib access, and a 46 times greater risk than subcostal access [Citation2]. Supra-11th rib access was avoided in the present study, as recommended previously [Citation2, Citation29] . In the present study, the independent factors for complications were surgical duration and stone burden. It was assumed that a previously operated kidney can be fixed in the retroperitoneum and does not descend during expiration. In such a situation a supracostal access can be associated with a higher rate of pleural violation. However, there was no such problem in the present study.
Injuries to adjacent organs are rare during supracostal upper calyceal access. A retro-renal left colon occurring in ≈ 10% of patients when prone, or a large spleen, can preclude access via the 10th or 11th intercostal space [Citation30]. A supra-11th access could puncture the liver in 14% and spleen in 33% of patients, particularly during inspiration, whereas the risk is minimal when needles are inserted via the posterior 11–12th intercostal approach with the patient in full expiration [Citation31]. In haemodynamically stable patients, liver injuries can often be managed conservatively with tube drainage and serial monitoring [Citation32]. However, splenic injuries are associated with increased bleeding and can require immediate exploration and splenectomy. The preoperative evaluation should include prone non-contrast CT to identify calculi, their distribution in the collecting system, the stone burden, as well as the location of adjacent structures to develop the optimal trajectory for an access tract that is least prone to incur complications [Citation33].
The present study, although not randomised or controlled, indicates that supracostal upper calyceal access to staghorn calculi offers the advantages of a short direct tract with excellent visibility of most of the calyces, reasonable operative duration, and good stone-free rates. Thus although the supracostal approach to the upper pole is associated with a small risk of chest complications, such problems are easily managed by inserting a chest tube, and can usually be avoided if precautions are adequate.
Conflict of interest
No conflict of interest to declare.
Source of funding
There was no funding or any disclosure to companies.
Acknowledgement
The author acknowledges his colleagues for their support and cooperation.
Notes
Peer review under responsibility of Arab Association of Urology.
References
- G.M.PremingerD.G.AssimosJ.E.LingemanS.Y.NakadaM.S.PearleJ.S.WolfJr.AUA (AUA Nephrolithiasis Guideline Panel). AUA guideline on management of staghorn calculi: diagnosis and treatment recommendationsJ Urol173200519912000
- R.MunverF.C.DelvecchioG.E.NewmanG.M.PremingerCritical analysis of supracostal access for percutaneous renal surgeryJ Urol166200112421246
- S.G.SteningS.BourneSupracostal percutaneous nephrolithotomy for upper pole calyceal calculiJ Endourol121998359362
- R.GuptaA.KumarR.KapoorA.SrivastavaA.MandhaniProspective evaluation of safety and efficacy of the supracostal approach for percutaneous nephrolithotomyBJU Int902002809813
- N.R.NettoJr.J.IkonomidisO.IkariJ.A.ClaroComparative study of percutaneous access for staghorn calculiUrology652005659663
- D.DindoN.DemartinesP.A.ClavienClassification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a surveyAnn Surg2402004205213
- E.LangR.ThomasR.DavisI.ColonM.AllafA.HananoetalRisks, advantages, and complications of intercostal vs. subcostal approach for percutaneous nephrolithotomyUrology472009751756
- P.B.IrbyB.F.SchwartzM.L.StollerPercutaneous access techniques in renal surgeryTech Urol519992939
- G.M.PremingerS.SchultzR.V.ClaymanT.CurryH.C.RedmanP.C.PetersCephalad renal movement during percutaneous nephrostolithotomyJ Urol1371987623625
- K.L.Mooreeditor. The thorax. In: Clinically Oriented Anatomy. third ed. Baltimore: Williams & Wilkins, 1992. p. 33–125
- M.AronR.GoelP.K.KesarwaniA.SethN.P.GuptaUpper pole access for complex lower pole renal calculiBJU Int942004849852
- S.SukumarB.NairG.KumarK.V.SanjeevanH.S.BhatSupracostal access for percutaneous nephrolithotomy: less morbid, more effectiveInt Urol Nephrol402008263267
- F.J.SampaioA.H.AragaoAnatomical relationship between intrarenal arteries and the kidney collecting systemJ Urol1431990679681
- F.J.SampaioJ.F.ZanierA.H.AragaoL.A.FavoritoIntrarenal access: three-dimensional anatomical studyJ Urol1481992769773
- A.R.El-NahasI.ErakyA.A.ShokeirA.M.ShomaA.M.El-AssmyN.A.El-TabeyetalFactors affecting stone-free rate and complications of percutaneous nephrolithotomy for treatment of staghorn stoneUrology79201212361241
- Z.ZhuS.WangQ.XiJ.BaiX.YuJ.LiuLogistic regression model for predicting stone-free rate after minimally invasive percutaneous nephrolithotomyUrology7820113236
- D.GolijaninR.KatzA.VerstandingT.SassonE.H.LandauS.MeretykThe supracostal percutaneous nephrostomy for treatment of staghorn and complex kidney stonesJ Endourol121998403405
- A.ShabanA.KoderaM.N.ElGhoneimyT.Z.OrbanK.MursiA.HegazySafety and efficacy of supracostal access in percutaneous renal surgeryJ Endourol2220082933
- S.H.Mousavi-BaharS.MehrabiM.K.MoslemiThe safety and efficacy of PCNL with supracostal approach in the treatment of renal stonesInt Urol Nephrol432011983987
- R.J.HoneyJ.D.WiesenthalD.GhiculeteS.PaceA.A.RayK.T.PaceComparison of supracostal versus infracostal percutaneous nephrolithotomy using the novel prone-flexed patient positionJ Endourol252011947954
- H.N.ShahS.S.HegdeJ.N.ShahM.B.BasalSafety and efficacy of supracostal access in tubeless percutaneous nephrolithotomyJ Endourol20201010161021
- J.Jun-OuB.LojanapiwatSupracostal access: does it affect tubeless percutaneous nephrolithotomy efficacy and safetyInt Braz J Urol632010171176
- B.LojanapiwatS.PrasopsukUpper pole access for percutaneous nephrolithotomy. Comparison of supracostal and infracostal approachesJ Endourol202006391395
- N.S.KekreG.G.GopalakrishnanG.G.GuptaB.N.AbrahamE.SharmaSupracostal approach in percutaneous nephrolithotomy: experience with 102 casesJ Endourol152001789791
- C.WongR.J.LeveilleeSingle upper-pole percutaneous access for treatment of ⩾5-cm complex branched staghorn calculi: is shock wave lithotripsy necessary?J Endourol162002477481
- R.YadavM.AronN.P.GuptaA.K.HemalA.SethS.B.KollaSafety of supracostal punctures for percutaneous renal surgeryInter J Urol13200612671270
- A.R.El-NahasA.A.ShokeirA.M.El-AssmyT.MohsenA.M.ShomaI.ErakyetalPost-percutaneous nephrolithotomy extensive hemorrhage. A study of risk factorsJ Urol1772007576579
- A.R.El-NahasI.ErakyA.A.ShokeirA.M.ShomaA.M.El-AssmyN.A.El-TabeyetalPercutaneous nephrolithotomy for treating staghorn stones. 10 years of experience of a tertiary-care centre. ArabJ Urol102012324329
- C.D.LallasF.C.DelvecchioB.R.EvansA.D.SilversteinG.M.PremingerB.K.AugeManagement of nephropleural fistula after supracostal percutaneous nephrolithotomyUrology642004241245
- P.MozerP.L.ConortA.LeroyM.BaumannY.PayanJ.TroccazetalAid to percutaneous renal access by virtual projection of the ultrasound puncture tract onto fluoroscopic imagesJ Endourol212007460465
- K.D.HopperW.F.YakesThe posterior intercostal approach for percutaneous renal procedures. Risk of puncturing the lung, spleen, and liver as determined by CTAJR Am J Roentgenol1541990115117
- A.R.El-NahasA.M.MansourR.EllaithyH.Abol-EneinConservative treatment of liver injury during percutaneous nephrolithotomyJ Endourol22200816491652
- C.S.NgB.R.HertsS.B.StreamPercutaneous access to upper pole renal stones. Role of prone 3-dimensional computerized tomography in inspiratory and expiratory phasesJ Urol1732005124126