Abstract
Objective: To present the results of upper calyceal access during percutaneous nephrolithotripsy (PCNL) for stones in the lower calyx, as PCNL is considered the most effective minimally invasive surgery for managing lower calyceal stones, with percutaneous access either directly to the lower calyx or through an upper or middle calyx.
Patients and methods: The study included 76 patients with single (51) and multiple (25) stones in the lower calyx, and stones in the lower calyx plus renal pelvis (six) and associated pelvi-ureteric junction obstruction (PUJO, five). They were managed by PCNL using retrograde access through the upper-pole calyx in addition to laser endopyelotomy for the PUJO.
Results: The mean duration required for establishing the retrograde nephrostomy tract was 14.4 min, and for completing the procedure was 40 min. The mean fluoroscopy exposure time was 3.2 min. Access from the upper calyx allowed easy and rapid advancement of the nephroscope to the lower calyx. The stones varied in size, at 10–25 mm. Stones were cleared completely in 70 of the 76 patients (92%); the stone-free rate was 100%. The residual stone fragments (2–4 mm) in the remaining six patients (8%) were considered insignificant. Complications were minor in four patients (5%), and included pleural effusion in two, bleeding in one and an arteriovenous fistula in one.
Conclusions: Upper-pole calyceal access for PCNL provides easy and effective clearance of stones in the lower calyx. This access should be considered for PCNL of single or multiple stones in the lower calyx.
Abbreviations:
Introduction
Lower calyceal stones or residual stone fragments after ESWL often do not require intervention except if they are symptomatic or associated with recurrent infection. Intervention is also required if the stones are present in a solitary kidney with a high risk of stone migration to the ureter causing obstruction and possible anuria. Small untreated stones in the lower calyx either migrate spontaneously to the ureter, or more commonly grow larger with an increased risk of infection [Citation1]. Only 11% of patients with calyceal stones remain symptom-free after 10 years of follow-up [Citation1].
As reported by Albala et al. [Citation2], the clearance rates after percutaneous nephrolithotripsy (PCNL) for stones in the lower calyx varied with stone size, being 100% for stones of ⩽10 mm, 93% for 11–20 mm and 86% for 21–30 mm. Those authors did not specify the puncture access site in their series. A stone of >10 mm in a small lower calyx can occupy a significant proportion of that calyx. Puncturing the calyx for PCNL will allow a limited space to accommodate the Amplatz sheath and nephroscope. This can cause difficulties in the procedure and hinder the efficacy of clearing stone fragments. In the present study the upper-pole calyx was punctured in all patients, and the objective was to evaluate the outcome of PCNL for lower calyceal stones after access from an upper pole calyx.
Patients and methods
In this retrospective study between June 1997 and December 2011, 76 unselected patients with lower-pole stones (single in 51 and multiple in 25) were treated by PCNL. Six patients had additional stones in the renal pelvis. Hydronephrosis was present in 11 patients, caused by a stone in the renal pelvis in six or associated PUJ obstruction (PUJO) in five. No patients had abnormal findings in the contralateral kidney. The lower calyx con was simple in 42 patients and compound in the remaining 34. The mean (range) age of the patients was 37 (25–70) years, and 41 were men and 35 women ().
Table 1 Patients and stones treated.
Procedure
The procedure was done under C-arm fluoroscopic guidance by retrograde percutaneous upper-calyceal access. The patient was placed in the lithotomy position with the ipsilateral hemipelvis and scapula elevated using appropriate support. Retrograde access was made using the Lawson retrograde nephrostomy wire puncture set (Cook Urological, Spencer, IN, USA). The steps done were in accordance with the technique described by Hawkins et al. [Citation3]. A 7-F Torcon catheter was advanced over a guidewire into the desired upper calyx. A 3-F PTFE sheath containing the 4.3 mm (0.017-inch) stainless-steel puncture wire was then advanced through the Torcon catheter.
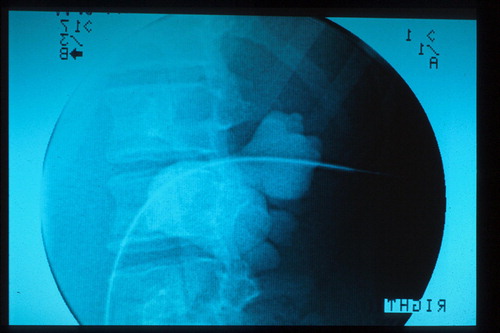
Under fluoroscopic control all punctures were made during inspiration, where the kidney is pushed down, and the goal was to obtain subcostal access. The puncture wire was advanced from the lumen of the upper calyx into the kidney parenchyma and body wall in a horizontal plane to the skin (). The posterior axillary line was used as a landmark on the skin for the emergence of the puncture wire. A small skin incision was made over the protruding skin area by the puncture wire, allowing it to exit through that incision.
Figure 1 Fluoroscopy-guided retrograde puncture of the upper calyx.
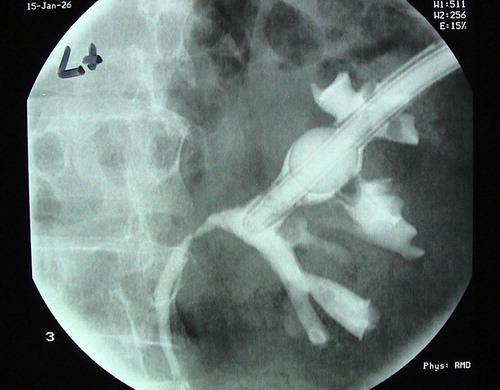
Fascial dilators were used antegradely to create a tract wide enough to allow the Torcon catheter to advance out through it. After removing the Torcon catheter, the puncture wire was exchanged for a standard 0.9 mm guidewire to complete the formation of a 28-F nephrostomy tract. Lithotripsy was achieved either ultrasonically or with the Lithoclast, using a short nephroscope. The rigid ureteroscope was resorted to when the lower calyx had a narrow neck (11 cases) or when the access to the lower calyx was too long (four cases). Laser endopyelotomy was used for the PUJO, with antegrade insertion of an endopyelotomy stent (five cases). A nephrostomy catheter was fixed at the end of the procedure through the upper calyx (). A chest radiogram was taken routinely immediately after surgery in all patients.
Figure 2 The nephrostomy catheter in the upper-pole calyx, with the nephrostogram.
Follow-up
Postoperative stone clearance was assessed before the patient was discharged, using a plain X-ray of the abdomen, and CT. Nephrostograms were taken before removing the nephrostomy tube, to exclude ureteric obstruction by possible residual stone fragments. Follow-up plain films were taken routinely at 2 months after discharge from the hospital.
Results
The mean (range) duration required to establish the retrograde nephrostomy tract was 14.4 (9–35) min, with a fluoroscopy exposure time of 3.2 (3–14) min. The duration of PCNL was 40 (20–60) min, with a fluoroscopy exposure time of 4.5 (3–14) min. The skin puncture was below the costal margin in 43 patients, and a supracostal puncture was above the 12th rib in 25 patients, and above the 11th rib in eight ().
Table 2 Results of the procedure.
Once the nephroscope was introduced into the intrarenal system it was easily advanced from the upper calyx through the renal pelvis to the lower calyx. Patients with stones in the renal pelvis had their stones removed before proceeding to manage the lower calyceal stones. The mean (range) stone size was 17 (10–30) mm. Complete stone clearance was documented by plain films and tomography before patient discharge in 70 of the 76 patients. In the remaining six patients small stone fragments (2–4 mm) were detected. The postoperative stone-free rate was 100% before discharge from the hospital, based on the consideration that residual stone fragments of ⩽4 mm are statistically insignificant. Postoperative nephrostograms taken before removing the nephrostomy catheters showed ureteric patency in all patients. Complications occurred in four patients (5%). Two with a skin puncture above the 11th rib developed pleural effusion that was managed conservatively. Bleeding occurred during tract dilatation in one patient, who required transfusion of one unit of blood. Another patient developed an arteriovenous fistula that was successfully managed by percutaneous embolisation. None of the patients had pneumothorax or haemothorax. The mean (range) hospital stay was 4.5 (3–7) days.
Discussion
Even though rapid advances in flexible ureterorenoscopy are yielding promising results for clearing lower calyceal stones [Citation4], the results of PCNL remain superior to those of both flexible ureterorenoscopy and ESWL [2Citation2,Citation5,Citation6] . The access site for PCNL that targets a lower-pole calyceal stone varies according to the surgeon’s preference. The lower calyx containing the stone is also frequently selected as the access site. If the stone is >10 mm the space available for the Amplatz sheath and the nephroscope can be limited, making the procedure difficult. Moreover, with the stone being positioned between the tip of the nephroscope distally and the neck of the lower calyx proximally, stone fragments during lithotripsy are liable to escape from the calyx to more remote sites in the intrarenal system. This can significantly reduce the rate of stone clearance at the end of the procedure. These limiting factors were not present in the current study when an upper-pole calyceal puncture was used. The Amplatz sheath was in the renal pelvis just proximal to the neck of the lower calyx. The tip of the nephroscope was advanced into the lower calyx, reaching the stone, and lithotripsy performed with the stone fragments entrapped within the calyx.
The upper-pole calyx is considered the most versatile site through which most of the intrarenal system can be easily entered [Citation7, Citation8] . It provides optimal visibility and ease of intraoperative advance of the Amplatz sheath or the rigid nephroscope to the lower-pole calyx. When the nephroscope reaches the lower-pole calyx containing a stone, the stone is fragmented easily even if large and occupying most of the calyceal lumen. Stone fragments are entrapped inside the calyx and are cleared by PCNL, with a greater potential for complete stone clearance.
Stone clearance after ESWL, retrograde intrarenal surgery or PCNL is considered complete when there are no stone fragments detected or if there are residual fragments of ⩽3–4 mm [Citation3,Citation4,Citation9–Citation11] . Plain films were taken in all patients before discharge, and at the 2-month follow-up. They all showed complete stone clearance in 70 of the 76 patients; the remaining six had insignificant stone fragments of 2–4 mm in the lower calyx.
The notion that supracostal access for PCNL should be discouraged because of the potential risk of damage to the lung and pleura is inaccurate. Pleural injury is usually prevented when an antegrade supracostal skin puncture is made lateral to the midscapular line, below the 11th rib, during deep ‘expiration’ [Citation12]. However, in the author’s experience, retrograde puncture of the upper calyx is better made at full ‘inspiration’. The kidney during full inspiration is at its lowest level, and is completely below the lung, with no risk of lung injury if the puncture is made in a horizontal plane (). At full inspiration the skin was punctured under the costal margin in more than half the patients (57%). Among the eight patients (11%) who had a skin puncture above the 11th rib, two developed pleural effusion that was self-limited. None of the patients had a lung injury. Complications reported in this and other studies after supracostal access were few [Citation8,Citation13–Citation16] , and are comparable in severity with subcostal access [Citation14].
The retrograde percutaneous access into the collecting system has been adopted as a routine procedure by the author since January 1997. Few cases were done using antegrade access, and too few to add to this study for comparing the results. Retrograde access was previously achieved by various methods, that included placing a ureteric catheter, inserting a flexible ureteroscope or using a retrograde inserted device [Citation7]. In the present study the Lawson retrograde nephrostomy wire puncture set was used. Retrograde percutaneous access has the advantage of being a safe procedure that establishes the nephrostomy tract easily and rapidly, with low fluoroscopy exposure, even in the presence of an undilated collecting system [Citation17, Citation18] . Retrograde access also provides control of both ends of the guidewire used, thus eliminating the risk of accidental wire displacement, particularly at the time of tract dilatation.
Ureteric obstruction is a limiting factor for retrograde access [Citation19], and retrograde access should not be attempted if there is ureteric obstruction. Advance of the nephroscope from the upper- to the lower-pole calyx can be hindered if the neck of the lower calyx is narrow. This can be corrected by balloon dilatation of the narrow neck or by using a low calibre rigid ureteroscope that can pass through the narrow neck, and then use Lithoclast lithotripsy (11 cases in the present study). The ureteroscope can also be used instead of the nephroscope if the access to the lower calyx is too long (four cases in the present study).
Most previous studies failed to mention the site of calyceal puncture used for PCNL. This important variable can be a defining factor in improving stone clearance, and should be addressed more thoroughly in future studies.
In conclusion, percutaneous retrograde access through the upper-pole calyx for PCNL was used to treat stones in the lower calyx and to manage associated PUJO. Establishment of a nephrostomy tract was rapid and safe, with low irradiation exposure. Access to the renal pelvis and lower-pole calyx was easy, and the stone-free rate for stones of 10–30 mm in the lower calyx (and renal pelvis) was 100%.
Conflict of interest
No conflict of interest.
Funding
This work was not funded.
Notes
Peer review under responsibility of Arab Association of Urology.
References
- W.HübnerP.PorpaczyTreatment of caliceal calculiBr J Urol661990911
- D.M.AlbalaD.G.AssimosR.V.ClaymanJ.D.DenstedtM.GrassoJ.Gutierrez-AcevesetalLower pole I. A prospective randomized trial of extracorporeal shock wave lithotripsy and percutaneous nephrostolithotomy for lower pole nephrolithiasis-initial resultsJ Urol166200120722080
- I.F.HawkinsJr.P.HunterG.LealG.NanniM.HawkinsB.FinlaysonetalRetrograde nephrostomy for stone removal: combined cystoscopic/percutaneous techniqueAm J Roentgenol1431984299304
- Knoll T, Buchholz N, Wendt-Nordahl G. Extracorporeal shockwave lithotripsy vs. percutaneous nephrolithotomy vs. flexible ureterorenoscopy for lower-pole stones. Arab J Urol; in press.
- Bagley DH, Healy KA, Kleinmann N. Ureteroscopic treatment of larger renal calculi (>2 cm). Arab J Urol; in press.
- A.R.El-NahasH.M.IbrahimR.F.YoussefK.Z.SheirFlexible ureterorenoscopy versus extracorporeal shock wave lithotripsy for treatment of lower pole stones of 10–20 mmBJU Int2012 Epub ahead of print
- J.S.WolfPercutaneous approaches to the upper urinary tract collecting systemA.J.WeinL.R.KavoussiA.C.NovickA.W.PartinC.A.PetersCampbell-Walsh Urology10th edn.2012Elsevier SaundersPhiladelphia13241356
- A.RazaS.MoussaG.SmithD.A.TolleyUpper pole puncture in percutaneous nephrolithotomy, a retrospective review of treatment, safety and efficacyBJU Int1012008599602
- M.S.PearleJ.E.LingemanR.LeveilleeR.KuoG.M.PremingerR.B.NadleretalProspective, randomized trial comparing shock wave lithotripsy and ureteroscopy for lower pole caliceal calculi 1 cm or lessJ Urol173200520052009
- A.SkolarikosA.G.PapatsorisDiagnosis and management of postpercutaneous nephrolithotomy residual stone fragmentsJ Endourol23200917511755
- P.CarlssonA.C.KinnH.G.TiseliusH.OhlsenM.RahmqvistCost effectiveness of extracorporeal shock wave lithotripsy and percutaneous nephrolithotomy for medium-sized kidney stones. A randomized clinical trialScand J Urol Nephrol261992257263
- S.G.SteningS.BourneSupracostal percutaneous nephrolithotomy for upper pole calyceal calculiJ Endourol121998359362
- P.N.MaheshwariM.G.AndankarS.HedgeM.BansalThe supracostal approach for percutaneous nephrolithotomyBJU Int852000557559
- E.RadeckaM.BrehmerK.HolmgrenA.MagnussonComplications associated with percutaneous nephrolithotripsy: supra- versus subcostal access. A retrospective studyActa Radiol442003447451
- E.LangR.ThomasR.DavisI.ColonM.AllafA.HananoetalRisks, advantage, and complications of intercostal vs subcostal approach for percutaneous nephrolithotripsyUrology742009751755
- R.GuptaA.KumarR.KapoorA.SrivastavaA.MandhaniProspective evaluation of safety and efficacy of supracostal approach for percutaneous nephrolithotomyBJU Int902002809813
- H.Y.WongL.HinsonD.P.GriffithRetrograde nephrostomy. advantages, disadvantages, and the learning curveJ Endourol91995461463
- T.KawaharaH.ItoH.TeraoM.YoshidaT.OgawaH.UemuraetalUreteroscopy assisted retrograde nephrostomy: a new technique for percutaneous nephrolithotomy (PCNL)BJU Int2012 Epub ahead of print
- D.H.HoskingRetrograde accessA.D.SmithG.H.BadlaniD.H.BagleyR.V.ClaymanG.H.JordanL.R.KavoussietalSmith’s Textbook of Endourology1996Quality Medical Publishing Inc.St. Louis, Missouri