Abstract
The link between erectile dysfunction (ED) and cardiovascular disease (CVD) is reviewed by assessing original papers, current consensus, previous reviews and meta-analyses. The link between these conditions is confirmed, and the evaluation and assessment summarised with a new evidence-based algorithm. ED, especially in younger men, is a marker of an increased risk of CVD, and ED needs to be incorporated into all risk-screening programmes.
Introduction
Erectile dysfunction (ED) is common, as is cardiovascular disease (CVD). As both affect similar groups it is not surprising that the two conditions frequently coexist [Citation1,Citation2]. Several epidemiological studies show both a high incidence and prevalence of ED worldwide, currently affecting up to 150 million men [Citation3]. ED increases in incidence with age, affecting two-thirds of men aged >70 years. In the Massachusetts Male Aging Study (a large community-based observational survey of men aged 40–70 years) the prevalence overall was 52% in men aged 40–70 years and graded as minimal in 17.2%, moderate in 25.2% and complete in 9.6% [Citation4]. In a European study of men aged 18–75 years the prevalence was 19% and in a UK study of men in the same age group, the prevalence was 39% for lifetime ED and 26% for current ED [Citation5,Citation6]. A consistent finding was a significant increase in ED with age, and as the world population is ageing, by 2025 the prevalence is expected to increase to 300 million men worldwide [Citation7].
Importantly, ED is now recognised for most men to be of vascular aetiology, with endothelial dysfunction as the common denominator, hence ‘ED = ED’ [Citation8]. ED often precedes CVD and is often present in men with known CVD, leading to the concept that a man with ED and no CVD symptoms is a cardiac or vascular patient until proved otherwise, and a man with known CVD should be routinely asked about his erectile function [Citation9,Citation10]. ED also has a significant negative impact on the patient and partner (a man’s problem but a couple’s concern) thus emphasising the need to address ED as early as possible [Citation11].
Risk factors
The modifiable risk factors for CVD are shared with ED. They include hypertension, hyperlipidaemia, diabetes, obesity, lack of physical exercise, cigarette smoking, poor diet, excess alcohol consumption, and psychological stress, including depression [Citation12]. Of clinical importance is the recognition that ED is an independent marker of increased risk in addition to the conventional risk factors [Citation1,Citation2]. In a systematic review and meta-analysis including six clinical trials and 740 participants from four countries, lifestyle modification and pharmacological therapy (e.g. statins) were associated with a statistically significant improvement in sexual function, changes that historically have also been shown to reduce the risk of CVD and mortality [Citation13]. Men with ED therefore provide an opportunity to identify CVD risk factors and initiate targeted risk-reduction lifestyle changes. By reducing the risk of ED this might be an unexplored motivation to tackle CVD risk factors, adding ‘life to years’ as well as years to life.
The importance of reducing risk factors remains fundamental to the overall vascular good health of the individual, and that includes sexual vascular health [Citation14]. The triad of ED, endothelial dysfunction and CVD emphasises the need for ED to be included in all CVD risk calculators [Citation15]. In addition, those who are driven by health economics can be reassured, as asking the ED question is cost neutral (i.e. free).
ED and CVD: examining the link
In 2001 two reports suggested that ED could be a marker for silent (asymptomatic) coronary artery disease (CAD) [Citation16,Citation17]. Subsequent reports identified ED preceding CAD in about two-thirds of cases, with the time interval from ED to CAD symptoms being 2–3 years and a cardiovascular event (myocardial infarction, MI, and stroke) 3–5 years, although longer time frames have been reported [Citation18–Citation20]. Furthermore, the severity of the ED correlates with the severity of the CAD [Citation21].
It has been hypothesised that the ‘artery size’ difference explains the onset of ED before a CVD event (). Penile arteries are 1–2 mm and coronary arteries 3–4 mm in diameter. Endothelial dysfunctions and plaque burden in the smaller arteries would be symptomatic (ED) before the similar process in the larger arteries affects flow. An asymptomatic lipid-rich plaque in the coronary arteries might be vulnerable to rupture, so that ED might predict an acute coronary syndrome or death, given that most acute events including sudden death occur without cardiac warning symptoms [Citation22,Citation23].
Table 1 Artery size and atherothrombosis. A significant restriction to flow in the penile arteries may be subclinical in larger vessels.
We now have the benefit of two meta-analyses addressing the role of ED in predicting the risk of CVD and both cardiovascular and all-cause mortality [Citation24,Citation25]. In a meta-analysis of 12 prospective cohort studies involving 36,744 men, ED significantly increased the risk of CVD, CAD, stroke and all-cause mortality, driven mainly by an increase in cardiovascular mortality, and did so independently of conventional risk factors [Citation24] (). In the second systematic review and meta-analysis all longitudinal studies addressing the predictive role of ED and CVD were analysed [Citation25]. Fourteen studies were included, involving 92,757 men. The findings were very similar () with, in addition, increased risk being associated with a younger age and those at intermediate CVD risk (5–20% 10-year risk).
Table 2 The relative risks for men with ED vs. no ED, in the first [Citation24] and second analysis [Citation25].
Also, the relative risk of patients with ED for all-cause mortality was significantly higher in men with known CVD [Citation25] (1.90 vs. 1.20, P = 0.021). This accords with a trial of men with known CVD, where ED was substantially predictive of all-cause mortality (hazard ratio 1.84) and the composite of CVD death, MI, stroke and admissions for heart failure (hazard ratio 1.42) with double the incidence of death from CVD and MI [Citation10].
As there is also good evidence that ED predicts an acute coronary syndrome (usually due to asymptomatic plaque rupture) [Citation26] the hypothesis of the asymptomatic lipid-rich plaque rupturing supports the artery-size hypothesis and the role of ED as a window of opportunity for preventing a subsequent CVD event, including death [Citation22,Citation25].
Assessing the patient
As ED and CVD are clearly linked, all men with ED should undergo a thorough medical, including cardiological, assessment. In the first instance, one needs to be sure of the ED diagnosis and to establish whether there is premature ejaculation, decreased libido, or a combination of problems. From a cardiovascular perspective the medical assessment should include measurements of blood pressure, fasting glucose, glycosylated haemoglobin and the lipid profile, waist circumference, thyroid function and testosterone (before 11.00 h) [Citation1,Citation2,Citation14]. Testosterone deficiency is often missed, and because it is frequently associated with type II diabetes or chronic illness such as heart failure, renal disease or hypertension, it should be excluded [Citation27].
The fundamental question is whether in men with ED there is asymptomatic CVD, especially CAD, and how to detect it. Stress testing on exercise or by pharmacology will only identify lesions influencing flow (>50–70% coronary artery stenosis), as will myocardial perfusion scanning or stress echocardiography [Citation1,Citation2]. Several studies have shown that ED is associated with markers and mediators of subclinical inflammation and endothelial activation, emphasising the potential ED/CVD link but not clarifying whether there is vulnerable plaque or not [Citation28]. Whilst stress testing has a role in establishing the cardiovascular safety of sexual activity, e.g. after MI or coronary angioplasty, subclinical plaque will not be detected and false reassurance given if stress testing is relied on for inclusion or exclusion of early plaque disease. This is obviously important because ED predicts acute coronary syndromes and all-cause mortality, which in 60% of cases are not associated with preceding cardiac symptoms [Citation25]. Therefore an evaluation of subclinical (<50%) plaque is essential, especially in the younger men at intermediate risk [Citation29]. Outpatient coronary calcium screening or multidetector CT (MDCT) shows clinical disease in men with ED and a normal exercise electrocardiogram (ECG) [Citation30]. The advantage of MDCT is that it identifies non-calcified disease, which might be an issue in the younger men [Citation31]. Interestingly, the average interval between an untreated abnormal finding on MDCT and a CVD event is 3–5 years, whether there is ED or not, and this is similar to the ED interval. Compared to a chest X-ray dose at 0.02 mSv, calcium screening at 1–2 mSv and MDCT at 5–20 mSv both increase the X-ray exposure, emphasising the importance of the diagnostic role of MDCT rather than its use as a fashionable annual screening tool [Citation32].
A reasonable strategy is to use calcium screening or preferably MDCT in those at most risk, especially younger men (aged 30–60 years), as in the algorithm (). is a right coronary lesion detected by MDCT in a 38-year-old man with a history of ED of 6 months, no cardiac symptoms, normal maximal exercise electrocardiogram and a calcium score of zero. A critical lesion is clearly apparent.
Figure 1 The investigative algorithm for CVD and ED.
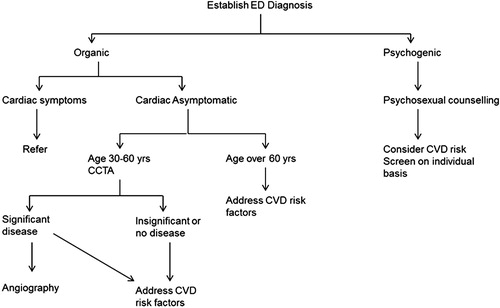
Figure 2 An angiogram showing a critical right coronary artery stenosis, with a normal exercise test and no calcium, but the patient had ED for 6 months.

Conclusion
In men with no cardiac symptoms ED, especially in younger men, is a marker of a significantly increased risk of CVD. The treatment of ED has a dual purpose, to restore sexual relations and to prevent subsequent CVD events, including death. ED in men with known CVD similarly identifies an increased risk. ED, like type II diabetes, is a cardiovascular equivalent requiring an aggressive risk-reduction strategy for CVD, whether there is or is no known CVD [Citation9,Citation33]. It is time to act on the evidence.
Conflict of interest
None.
Source of Funding
None.
Notes
Peer review under responsibility of Arab Association of Urology.
References
- G.JacksonN.BoonI.EardleyM.KirbyJ.DeanG.Hackettet alErectile dysfunction and coronary artery disease prediction: evidence-based guidance and consensusInt J Clin Pract642010848857
- A.NehraG.JacksonM.MinerK.L.BillupsA.L.BurnettJ.Buvatet alConsensus recommendations for the management of erectile dysfunction and cardiovascular diseaseMayo Clin Proc872013766778
- H.A.FeldmanI.GoldsteinD.G.HatzichristouR.J.KraneJ.B.McKinlayImpotence and its medical and psychosocial correlates: results of the Massachusetts male aging studyJ Urol15119945461
- H.A.FeldmanC.B.JohannesC.A.DerbyK.P.KleinmanB.A.MohrA.B.Araujoet alErectile dysfunction and coronary risk factors: prospective results from the Massachusetts male aging studyPrev Med302000328338
- M.BraunG.WassmerT.KlotzB.ReifenrathM.MathersU.EngelmannEpidemiology of erectile dysfunction: results of the ‘Cologne Male Survey’Int J Impot Res122000305311
- K.M.DunnP.R.CroftG.I.HackettSexual problems. A study of the prevalence and need for health care in the general populationFam Pract151998519524
- I.A.AytaJ.B.McKinlayR.J.KraneThe likely worldwide increase in erectile dysfunction between 1995 and 2025 and some possible policy consequencesBJU Int8419995056
- H.SolomonJ.W.ManG.JacksonErectile dysfunction and the cardiovascular patient: endothelial dysfunction is the common denominatorHeart892003251253
- G.JacksonP.MontorsiM.A.AdamsT.AnisA.El-SakkaM.Mineret alCardiovascular aspects of sexual medicineJ Sex Med7201016081626
- M.BohmM.BaumhakelK.TeoP.SleightJ.ProbstfieldP.Gaoet alErectile dysfunction predicts cardiovascular events in high-risk patients receiving telmisartan, ramipril, or both. The ONgoing Telmisartan Alone and in combination with Ramipril Global Endpoint Trial/Telmisartan Randomized AssessmeNt Study in ACE iNtolerant subjects with cardiovascular Disease (ONTARGET/TRANSCEND) TrialsCirculation121201014391446
- C.McVeyTaking a closer look at the impact of erectile dysfunctionMen’s Health J220031618
- C.G.BaconM.A.MittlemanI.KawachiE.GiovannucciD.B.GlasserE.RimmProspective study of risk factors for erectile dysfunctionJ Urol1762006217221
- B.P.GuptaM.H.MuradM.M.CliftonL.ProkopA.NehraS.L.KopeckyThe effect of lifestyle modification and cardiovascular risk factor reduction on erectile dysfunction: a systematic review and meta-analysisArch Intern Med171201117971803
- G.JacksonThe importance of risk factor reduction in erectile dysfunctionCurr Urol Rep82007463466
- C.VlachopoulosN.IoakeimidisD.Terentes-PrintziosC.StefanadisThe triad: erectile dysfunction – endothelial dysfunction – cardiovascular diseaseCurr Pharm Des14200837003714
- P.D.O’KaneG.JacksonErectile dysfunction: is there silent obstructive coronary artery disease?Int J Clin Pract552001219220
- M.KirbyG.JacksonJ.BetteridgeK.FriedliIs erectile dysfunction a marker for cardiovascular disease?Int J Clin Pract552001614618
- L.D.HodgesM.KirbyJ.SolankiJ.O’DonnellD.A.BrodieThe temporal relationship between erectile dysfunction and cardiovascular diseaseInt J Clin Pract61200720192025
- B.A.InmanJ.L.SauverD.J.JacobsonM.E.McGreeA.NehraM.M.Lieberet alA population-based, longitudinal study of erectile dysfunction and future coronary artery diseaseMayo Clin Proc842009108113
- A.PonholzerC.TemmlR.ObermayrC.WehrbergerS.MadersbacherIs erectile dysfunction an indicator for increased risk of coronary heart disease and stroke?Eur Urol482005512518
- P.MontorsiP.M.RavagnaniS.GalliF.RotatoriF.VegliaA.Brigantiet alAssociation between erectile dysfunction and coronary artery disease. Role of coronary clinical presentation and extent of coronary vessels involvement: the COBRA trialEur Heart J27200626322639
- P.MontorsiP.M.RavagnaniS.GalliF.RotatoriA.BrigantiA.Saloniaet alThe artery size hypothesis a macrovascular link between erectile dysfunction and coronary artery diseaseAm J Cardiol96200519M23M
- A.B.AraujoT.G.TravisonP.GanzG.R.ChiuV.KupelianR.C.Rosenet alErectile dysfunction and mortalityJ Sex Med6200924452454
- J.Y.DongY.H.ZhangL.Q.QinErectile dysfunction and risk of cardiovascular disease: meta-analysis of prospective cohort studiesJ Am Coll Cardiol58201113781385
- C.V.VlachopoulosD.G.Terentes-PrintziosN.K.IoakeimidisK.A.AznaouridisC.I.StefanadisPrediction of cardiovascular events and all-cause mortality with erectile dysfunction: a systematic review and meta-analysis of cohort studiesCirc Cardiovasc Qual Outcomes62013111
- F.MontorsiA.BrigantiA.SaloniaP.RigattiA.MargonatoA.Macchiet alErectile dysfunction prevalence, time of onset and association with risk factors in 300 consecutive patients with acute chest pain and angiographically documented coronary artery diseaseEur Urol442003360364
- G.JacksonTestosterone deficiency syndrome (TDS) and the heartEur Heart J31201014361437
- C.VlachopoulosK.AznaouridisN.IoakeimidisK.RokkasC.VasiliadouN.Alexopouloset alUnfavourable endothelial and inflammatory state in erectile dysfunction patients with or without coronary artery diseaseEur Heart J27200626402648
- M.MinerA.D.SeftelA.NehraP.GanzR.A.KlonerP.Montorsiet alPrognostic utility of erectile dysfunction for cardiovascular disease in younger men and those with diabetesAm Heart J16420122128
- G.JacksonS.PadleyErectile dysfunction and silent coronary artery disease: abnormal computed tomography coronary angiogram in the presence of normal exercise ECGsInt J Clin Pract622008973976
- S.SchroederS.AchenbachF.BengelC.BurgstahlerF.CademartiriP.de Feyteret alCardiac computed tomography. indications, applications, limitations, and training requirements: report of a writing group deployed by the working group nuclear cardiology and cardiac CT of the European society of cardiology and the European council of nuclear cardiologyEur Heart J292008531556
- J.M.GazianoP.W.WilsonCardiovascular risk assessment in the 21st centuryJama3082012816817
- G.JacksonErectile dysfunction. a marker of silent coronary artery diseaseEur Heart J27200626132614