
Sir,
We compliment and congratulate the authors of this paper for using urethral mobilisation to correct torsion associated with hypospadias, and appreciate the hard work done in compiling the data for their publication [Citation1]. However, there are a few points in the management of congenital penile torsion and the discussion section of the article that we would like to clarify.
| 1. | There is a spelling mistake in the Discussion, stating ‘Baht’ at two places, which should be ‘Bhat’. | ||||
| 2. | We appreciate the authors’ application of the technique of step-by-step mobilisation of the urethra and measuring the degree of correction after each step, thus proving that mobilisation of the urethral plate, diverting the spongiosum and proximal urethral mobilisation is effective for correcting ventral penile curvature. A very similar technique of mobilisation of the urethral plate with the spongiosum, and proximal urethral mobilisation for correcting both ventral curvature and penile torsion was reported previously [Citation2–Citation4]. | ||||
| 3. | Although the authors mention in their technique that they mobilised the urethral plate and spongiosum, the diagram shows that mobilisation of the urethra distally was only just proximal to the hypospadiac meatus (their ) [Citation1]. Possibly the authors might not have put that figure in the article, or it needs to be explained. The mobilisation of the urethral plate/hypoplastic urethra with spongiosum distally should be into the glans, as shown in and H in the reference [Citation2]. The cause of torsion in a significant proportion of patients is an aberrant attachment of the spongiosum to the cavernosa, which also extends beneath the glans. The torsion will not be corrected unless these attachments are dissected from the glans. Mobilisation of the urethral plate and spongiosum from the meatus into the glans is a very important step in the correction of torsion, and corrects torsion in 75% of cases. This has been proposed as a third step in the algorithm mentioned by Bhat et al. [Citation2]. Furthermore, proximal urethral mobilisation into the perineal region corrected torsion in only 22% of patients in our study [Citation2]. Thus it follows that proximal urethral mobilisation alone is not going to correct the curvature in all cases. Each step is important in the correction of torsion. We could correct torsion in 87.5% cases by combining all these steps of mobilisation. The authors concur with the same, stating that urethral mobilisation alone is not sufficient to correct congenital penile torsion. | ||||
| 4. | The authors have also raised some questions in the discussion about the aetiopathology of torsion. Previous reports show that torsion occurs because of faulty insertion of the coverings of the penis, i.e., the skin and dartos fascia, which originate from the ectoderm [Citation5,Citation6] and attachments of the urethral plate/hypoplastic urethra and spongiosum to the corporal bodies and glans [Citation2]. | ||||
| 5. | Furthermore, the authors propose that in their series the torsion was due to corporal disproportion and rotation of the corpora along a longitudinal axis. Corporal disproportion is more likely to lead to lateral curvature, which is a two-dimensional deformity, rather than torsion, which is a three-dimensional one [Citation2]. A corporal intrinsic defect has been noted previously as one of the causes of torsion. However, before labelling a corporal intrinsic factor as a cause of torsion, the spongiosal attachment to glans should be released, as it is a commoner cause of torsion. | ||||
Figure 1 Showing Mobilisation of urethra proximal to meatus.
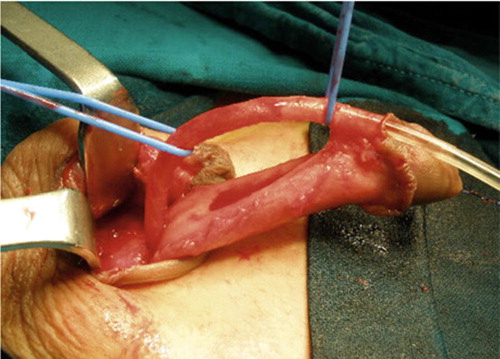
Figure 2 A & B. Showing mobilisation of urethra into glans.
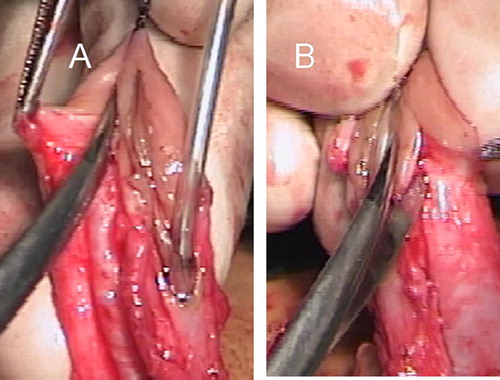
Figure 3 Mobilisation of urethral plate into glans for final correction of torsion

We agree that a suture between the opposite corpora and pubic periosteum is a known and effective technique to correct torsion, but we have reservations about taking such a suture between the opposite corpora and the pubic periosteum to create a counter-torsion, as it would either shorten the normally developed corpus cavernosum or create tension on an already twisted cavernosal cylinder. Is this not against the anatomical principles of surgery, wherein rather than correcting the pathological side, the normal side is being rendered pathological by plication? There is also a greater chance of infection of the periosteum. So if torsion persists after mobilising the urethral plate into the glans and proximal urethral mobilisation, we prefer the final adjustment of torsion to be done during skin closure if required [Citation3].
We suggest that the authors apply the technique of mobilisation of the urethral plate with spongiosum into the glans, and then re-evaluate the torsion, for a critical evaluation.
I hope this discussion will be useful for the reader when applying different techniques for correcting penile torsion.
Sincerely,
Dr. Amilal Bhat, Senior Professor and Head, and Dr. Karamveer Sabharwal, Senior Resident, Department of Urology, S.P. Medical College, Bikaner, Rajasthan, India.
Notes
Peer review under responsibility of Arab Association of Urology.
References
- A.ElbarkyA.ZakariaA.MatarA.E.NasharThe management of moderate and severe congenital penile torsion associated with hypospadias: Urethral mobilisation is not a panacea against torsionArab J Urol11201317
- A.BhatM.P.BhatG.SaxenaCorrection of penile torsion by mobilization of urethral plate and urethraJ Paediatr Urol52009451457
- A.BhatExtended urethral mobilization in incised plate urethroplasty for severe hypospadias: a variation in technique to improve chordee correctionJ Urol178200710311035
- W.T.SnodgrassJ.C.PrietoStraightening ventral curvature while preserving the urethral plate in proximal hypospadias repairJ Urol182200917201725
- J.F.RedmanN.K.BissadaOne stage correction of chordee and 180 degree penile torsionUrology71976632633
- J.F.RedmanTorsion of penis: a gross anatomic studyJ Urol1301983316318