
Abstract
Objective:
To determine the utility of the urinary stone-attenuation value (SAV, in Hounsfield units, HU) from non-contrast computed tomography (NCCT) for predicting the success of extracorporeal shock-wave lithotripsy (ESWL).
Patients and methods:
The study included 305 patients with renal calculi of ⩽30 mm and upper ureteric calculi of ⩽20 mm. The SAV was measured using NCCT. Numerical variables were compared using a one-way analysis of variance with posthoc multiple two-group comparisons. Univariate and multivariate regression analysis models were used to test the preferential effect of the independent variable(s) on the success of ESWL.
Results:
Patients were grouped according to the SAV as group 1 (⩽500 HU, 81 patients), group 2 (501–1000 HU, 141 patients) and group 3 (>1000 HU, 83 patients). ESWL was successful in 253 patients (83%). The rate of stone clearance was 100% in group 1, 95.7% (135/141) in group 2 and 44.6% (37/83) in group 3 (P = 0.001).
Conclusions:
The SAV value is an independent predictor of the success of ESWL and a useful tool for planning stone treatment. Patients with a SAV ⩾956 HU are not ideal candidates for ESWL. The inclusion criteria for ESWL of stones with a SAV <500 HU can be expanded with regard to stone size, site, age, renal function and coagulation profile. In patients with a SAV of 500–1000 HU, factors like a body mass index of >30 kg/m2 and a lower calyceal location make them less ideal for ESWL.
Introduction
Currently ESWL is the treatment of choice for most renal calculi ⩽30 mm, with success rates of 60–99% [Citation1–Citation3]. The failure of ESWL results in wasted medical costs, deterioration in patients with obstructed kidneys, unnecessary exposure to ionising radiation and to shock waves. Hence, it is desirable to distinguish those patients who would benefit from ESWL from those who need an alternative treatment.
Several studies concluded that the outcomes of ESWL correlate with several factors, including stone size, location, renal and calyceal anatomy, body mass index (BMI), stone composition, and recently the stone-attenuation value (SAV) [Citation4–Citation7]. Thus we evaluated whether the SAV of urinary calculi on non-contrast CT (NCCT), measured as Hounsfield units (HU) can be used as an independent predictor of calculus fragmentation by ESWL.
Patients and methods
Between June 2009 and October 2011, and with approval of the ethics board committee, 305 patients with a solitary renal or upper ureteric stone were treated by ESWL, using an electrohydraulic lithotripter, in a prospective study at the Beni-Suef University Hospital, Egypt.
An a priori power analysis used to calculate the sample size (Stats Direct version 2.7.2, Cheshire, UK), with the difference in the success rate of ESWL according to the SAV considered to be the principal study outcome. The calculation was based on comparing two proportions from independent samples using the chi-squared test, the α-error level was fixed at 0.05 and the power was set at 95%. The lowest ESWL success rate was ≈77%, and accordingly the optimum sample size was calculated to be ⩾81 patients in each arm to be able to detect a minimally important difference in the success rate of 20%.
The patients comprised 184 men and 121 women, aged 20–63 years, with either a renal stone ⩽3 cm (pelvic or calyceal) or an upper ureteric stone ⩽2 cm. Patients had radio-opaque stones and a normal renal anatomy. Patients with upper urinary tract stones >3 cm, an abnormal renal anatomy, morbid obesity (BMI ⩾ 40 kg/m2), renal insufficiency, distal obstruction, uncontrolled coagulopathy, uncontrolled hypertension, renal artery or aortic aneurysm, an active UTI or pregnancy were excluded from the study.
All patients were evaluated by a complete history and physical examination, urine analysis, urine culture, coagulation profile, complete blood count, and serum creatinine level. Imaging included abdomino-pelvic ultrasonography (US), a plain abdominal film, and NCCT with slices every 3 mm to measure the highest mean SAV and size of the stone.
The SAV was measured from three axial NCCT slices for each stone, i.e., one at the level of the stone’s maximum diameter, and one above and one below nearer to both poles of the stone. In each image, a circle was drawn inside the stone perimeter and the SAV was measured, with the highest value recorded.
All patients were treated by ESWL using an electrohydraulic lithotripter (using a spark-gap system with ellipsoidal focus, X-ray fluoroscopy localisation, a focal pressure of 55–110 MPa, focal point dimensions of 2.40 × 0.6 cm, a focal distance of 13.5 cm, and a shockwave frequency of 30–120/min).
All patients were treated while supine and by one urologist, and received intravenous analgesia in the form of 1 mg/kg meperidine hydrochloride and intravenous fluids throughout the procedure. Shock waves were not synchronised with the patient’s electrocardiogram. The power was increased from 6 to 22 kV, using a standardised protocol (500 shock waves up to 10 kV, 500 up to 14 kV, 1000 up to 18 kV, and 500 up to 22 kV), with a frequency of 60 shocks/min. The session was stopped when the machine’s upper limit of shock waves per session (2500) was reached.
Patients were followed up at 1 week after ESWL with a plain abdominal film and US. If there were significant fragments a second session of ESWL was planned. However, if there were only insignificant fragments the patients were given medical treatment and re-evaluated after 1 month. The final results were considered after the complete passage of all fragments or after 3 months from the last ESWL session.
The outcome of ESWL was described as a success or failure, where success included stone-free, i.e., complete stone clearance, or clinically insignificant residual fragments <4 mm with no symptoms at 3 months after ESWL. Failure was defined as residual stone fragments, i.e., clinically significant residual fragments ⩾4 mm after three sessions of ESWL, as confirmed by a plain film, or in patients with no evidence of fragmentation after three sessions of ESWL, as confirmed on a plain film.
The data are presented as the mean (SD) and range, or frequency (number of cases) and percentage, as appropriate. Numerical variables were compared between the study groups using a one-way anova with posthoc multiple two-group comparisons. To compare categorical data the chi-squared test was used. An exact test was used when the expected frequency was <5. Univariate and multivariate regression analysis models were used to test for the preferential effect of the independent variable(s) on the success rate. In all test, P < 0.05 was considered to indicate statistical significance.
Results
gives the data for patients and stones in each group, and for all 305 patients. The one-way anova test comparing the age, stone size, stone site, BMI and the SAV for each group showed that the three groups were comparable in all criteria except for the SAV (P < 0.001) and the stone size in group 1, which was greater than in the other groups (P < 0.001). The overall success rate of ESWL was 83% (253 patients). The mean (SD) SAV among the patients in which ESWL was successful was 669.2 (339.7) HU, whereas for those in whom ESWL failed it was 1099 (78.4) HU.
Table 1 The SAV with gender and stone site.
The univariate analysis using a t-test in all patients () showed that the stone site, BMI and SAV were the only statistically significant factors that influenced the success of ESWL. The success of ESWL was almost 90% for stones in the renal pelvis, 87% in the middle calyx, 85% in the upper ureter, 84% in the upper calyx and 69% for lower calyceal stones (P = 0.004). The univariate analysis using a t-test among each of the three groups showed that a BMI >30 kg/m2 was a significant predictor of the failure of ESWL in group 2 (P = 0.006), together with the SAV (P = 0.009). A linear regression analysis of the data from all patients showed that a high BMI (>30), a higher SAV (P < 0.001) and a stone in the lower calyx (P = 0.004) were predictors of the failure of ESWL. A linear regression through-the-origin analysis among each of the three groups showed that a high BMI (>30) (P = 0.000), a higher SAV (P = 0.002) and a stone in the lower calyx (P = 0.021) were predictors of failure in group 2, but only a high BMI predicted failure in group 3 (P = 0.001). In group 3, ESWL failed in 20 patients with lower calyceal stones (67%; ), vs. in 23 (49%) in those with stones in other locations, and this was a statistically significant predictor of the failure of ESWL in this group using the linear-by-linear association (P = 0.029).
Table 2 The effect of different variables on the success of ESWL (univariate analysis).
Table 3 The effect of SAV on the success of ESWL, the number of ESWL sessions, shock wave number and power required, and the results for lower calyceal stones.
However, on a multivariate logistic regression analysis in all patients, only a high BMI (>30) and higher SAV (>1000) were predictors of failure (P < 0.001). A logistic regression analysis of patients within each of the three groups showed that a high BMI and a stone in the lower calyx stone were predictors of failure in group 2 (P = 0.008 and 0.049, respectively) and only a high BMI predicted failure in group 3 (P = 0.015).
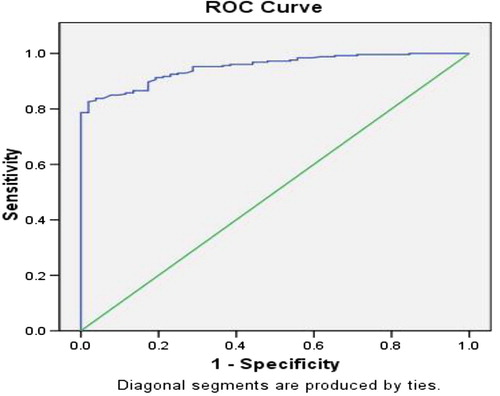
We used a receiver operating characteristic (ROC) curve () for the SAV to determine which SAV could be used to predict the success or failure of ESWL. Interpretation of the ROC curve showed that the ideal threshold SAV for success was ≈1000 HU, i.e., a SAV <877 HU would predict success with 100% specificity and 79% sensitivity and a SAV ⩽1112.5 HU would predict success with 71% specificity, and 95% sensitivity. A SAV ⩽1032 HU maximised both sensitivity and specificity, predicting success with 85% specificity and 87% sensitivity. Using the Youden index (a point that maximises the vertical distance of the curve from the line of equality) a SAV ⩽956.5 HU would predict success with 98% specificity and 83% sensitivity.
Figure 1 The ROC curve for HU to determine which SAV threshold predicts the success or failure of ESWL.
There were some complications; five patients (1.6%) had fever (>38 °C) and were managed with intravenous antibiotics. There were also 11 patients (3.6%) who had steinstrasse (among 92 patients, 11.9%, with large stones of ⩾22 mm), of whom eight were managed conservatively and three needed ureteroscopy.
Discussion
ESWL has revolutionised the management of urolithiasis, with further decreases in morbidity and mortality rates [Citation8]. The overall success rate of ESWL for treating upper urinary tract stones is 60–95%. Several factors are associated with a poor success rate of ESWL, including large renal calculi, stones within dependant or obstructed portions of the collecting system, stone composition (mostly calcium oxalate monohydrate and brushite) and obesity or a body habitus that hinders imaging. For patients with these clinical characteristics, alternative treatments should be considered [Citation9].
The failure of ESWL, necessitating multiple sessions, leads to an increase in the medical costs as well as the development of undesirable complications such as acute renal injury, haemorrhage and oedema. Proper case selection depends on several factors for both the success of ESWL and the avoidance of the side-effects of this treatment.
Dretler and Polykoff [Citation10] introduced the concept of stone fragility on ESWL, based on the composition of the stone. Cystine and brushite calculi are the most resistant to ESWL, followed by calcium oxalate monohydrate, struvite, calcium oxalate dihydrate, and uric acid stones. Stone composition affects the resistance to fragmentation and the type of fragments produced. Cystine and calcium oxalate monohydrate tend to produce large pieces that are difficult to clear from the collecting system, and they should be treated by ESWL only when the stone burden is small (i.e., <1.5 cm). Those patients with larger stones should preferentially be treated with percutaneous nephrolithotomy or ureteroscopy [Citation11,Citation12]. Except for cystinuric patients and patients who have had previous stone analysis, the accurate prediction of stone composition is not possible [Citation12].
Stone shape, homogeneity, and radiographic density in comparison with bone on a plain abdominal film have been used to predict stone composition and fragility, but the overall accuracy of predicting stone composition from plain radiographs was reported to be only 39% and therefore inadequate for clinical use [Citation13,Citation14]. NCCT can capture a density difference of 0.5%, as opposed to a plain film, which requires a density difference of >5% [Citation15]. The overlapping radio-densities preclude an accurate determination of stone composition, but NCCT provides an abundance of information on urinary tract calculi, including the size, shape, number, location, SAV, and skin-to-stone distance [Citation16].
Joseph et al. [Citation17] grouped patients according to the SAV in the same categories as used in the present study. The rate of stone clearance was 100% in group 1, 85.7% in group 2 and 54.5% in group 3. Patients in group 3 required a higher median number of shock waves for stone fragmentation than those in groups 1 and 2 (7300, 2500 and 3390, respectively). The mean SAV and number of shock waves required for stone fragmentation were significantly positively correlated, and those authors concluded that the success rate for stones with a SAV >1000 HU was significantly lower than that for stones with an SAV <1000 HU. Pareek et al. [Citation4] found that the mean (SD) SAV for the stone-free and residual-fragment groups were significantly different, at 577.8 (182.5) vs. 910.4 (190.2) HU, respectively, concluding that renal calculi with a high SAV (>900 HU) are more amenable to endoscopic manipulation as the initial treatment rather than ESWL.
Gupta et al. [Citation18] concluded that the worst outcome was in patients with a SAV >750 HU and a stone diameter >1.1 cm, as 77% of those patients needed more than three sessions of ESWL, and the clearance rate was 60%. Wang et al. [Citation19] concluded that a SAV >900 HU is a significant predictor of the failure of ESWL.
In the present study the overall number of stone-free patients after ESWL for upper urinary tract stones was 253/305 (83%). In 52 patients (17%) ESWL failed, which is consistent with previous studies reporting a failure rate of 5–20%.
The present study confirmed the results of previous studies for the effect of the SAV on the results of ESWL. All patients with a SAV ⩽500 HU were stone-free after one session, irrespective of the size and location of the stone (even for lower calyceal stones of up to 29 mm, ). In this group it was apparent that the stones start to fragment, and complete the fragmentation, at a low power (15–18 kV in 58% of patients). Nevertheless, the stones needed <2500 shock waves to achieve complete stone fragmentation (2040–2300 in 63% of the patients), with a mean (range) of 2118 (2040–2500) shock waves. This was not tested statistically, as more patients would be needed for a valid assessment of these findings ().
In patients with SAVs of 501–1000 HU the ESWL was successful in 95.7%, with about half of the patients needing two or three ESWL sessions; on average about two sessions are required, with a mean (range) of 4245 (2500–7500) shock waves. Predictors of failure in this group included a higher SAV >877 HU, a BMI >30 and a stone in the lower calyx.
In patients with a SAV >1000 HU, ESWL was successful in fewer than half of the patients (44.6%), none of them in a single session, with 16 of the 37 successful cases (43%) requiring three sessions. They required a mean (range) of 6080 (5000–7500) shock waves. The best predictor of ESWL failure in this group was a BMI >30, although a lower calyceal stone could also be predictive of failure.
The results in patients with a SAV ⩽500 HU warrant the expansion of the list of candidates eligible for ESWL. This list might include either patients who were previously contraindicated or for whom there was anxiety about the side-effects of a greater number and power of shock waves delivered to their kidneys, patients with large stones (i.e. renal stones ⩾3 cm and ureteric stones ⩾2 cm), those with renal insufficiency or coagulopathies, and infants and young children, who would be managed successfully with ESWL as fewer shock waves and a lower power are required to successfully treat this group of patients.
In patients with SAVs of 500–1000 HU, ESWL is an ideal treatment, but is expected to be less successful in some groups of patients, like obese patients with a BMI >30, with lower calyceal stones, and a SAV ⩾877 HU. Pareek et al. [Citation4] and El-Nahas et al. [Citation7] also reported that obesity or a BMI >30 had a significant negative effect on stone disintegration and the success rate of ESWL. The present study confirmed this effect of BMI, especially in patients with a SAV >500 HU.
Lower calyceal stones had the lowest success rate (68.5%) compared to other stone locations (), and were a significant predictor of failure, especially in patients with a SAV of 501–1000 HU, and to a much lower extent in those with a SAV >1000 HU.
There are some technical points related to our ESWL machine that might question the reproducibility of the present results with those from other ESWL machines. In particular, they concern the influence of BMI on success, as the focal distance of our machine was 13.5 cm, which is less than in many other machines that have focal distances of 14–18 cm. However, the Dornier HM3 (which has the highest reported success rate) has a focal distance of only 13 cm, and in all patients in the present study we could locate the stone. Moreover, our findings were consistent with the previous findings of many studies on the negative influence of a high BMI (>30).
Also, the focal point dimensions for our machine (2.40 × 0.6 cm) were also smaller than many other machines (smaller than that of the Dornier HM3, of 9 × 1.5 cm), which might affect the quality of the disintegration. However, the high focal pressure of 55–110 MPa might compensate for this, and our results were consistent with the reported success rates for ESWL.
In patients with a SAV >956.5 HU (or more simply, >≈1000 HU), ESWL should not be considered or offered to patients as a first treatment, especially in those with a BMI >30 and lower calyceal stones. As failure would be expected in more than half, together with the need for many sessions, this will increase the treatment-related morbidity with little cost benefit. Therefore, we recommend treating them with other methods rather than ESWL.
In conclusion, the SAV is an independent predictor of the success of ESWL, and a useful tool for planning the treatment of stones. Patients with a SAV >956.5 HU are not ideal candidates for ESWL. The inclusion criteria for ESWL in patients with a SAV <500 HU can be expanded for stone size, site, age, renal function and coagulation profile. In patients with a SAV of 500–1000 HU, factors like obesity and lower calyceal location make them less ideal for ESWL.
Conflict of interest
None declared.
Source of funding
None.
Notes
Peer review under responsibility of Arab Association of Urology.
References
- J.S.WolfR.V.ClaymanPercutaneous nephrostolithotomy. What is its role in 1997Urol Clin N Am2419974358
- J.E.LingemanD.NewmanJ.H.MertzP.G.MosbaughR.E.SteeleR.J.Kahnoskiet alExtracorporeal shock wave lithotripsy: the Methodist Indiana experienceJ Urol135199611341137
- J.J.RassweilerC.RennerC.ChaussyS.ThüroffTreatment of renal stones by extracorporeal shockwave lithotripsy: an updateEur Urol392001187199
- G.PareekN.A.ArmenakasG.PanagopoulosJ.J.BrunoJ.A.FracchiaExtracorporeal shock wave lithotripsy success based on body mass index and Hounsfield unitsUrology6520053336
- J.W.ChoiP.H.SongH.T.KimPredictive factors of the outcome of extracorporeal shockwave lithotripsy for ureteral stonesKorean J Urol532012424430
- A.N.ArgyropoulosD.A.TolleyOptimizing shock wave lithotripsy in the 21st centuryEur Urol522007344354
- A.R.El-NahasA.M.El-AssmyO.MansourK.Z.SheirA prospective multivariate analysis of factors predicting stone disintegration by extracorporeal shock wave lithotripsy. The value of high-resolution noncontrast computed tomographyEur Urol51200716881694
- N.L.MillerJ.E.LingemanManagement of kidney stonesBMJ3342007468472
- Y.M.TanS.K.YipT.W.ChongM.Y.WongC.ChengK.T.FooClinical experience and results of ESWL treatment for 3,093 urinary calculi with the Storz Modulith SL 20 lithotripter at the Singapore general hospitalScand J Urol Nephrol362002363367
- S.P.DretlerG.PolykoffCalcium oxalate stone morphology: Fine tuning our therapeutic distinctionsJ Urol1551996828833
- K.C.SawJ.E.LingemanLesson 20. Management of calyceal stonesAUA Update Series201999154159
- G.PittomvilsH.VandeursenM.WeversJ.P.LafautD.De RidderP.De Meesteret alThe influence of internal stone structure upon the fracture behaviour of urinary calculiUltrasound Med Biol201994803810
- S.RamakumarD.E.PattersonA.J.Le RoyC.E.BenderS.B.EricksonD.M.Wilsonet alPrediction of stone composition from plain radiographs: a prospective studyJ Endourol131999397401
- C.G.ChaussyG.J.FuchsCurrent state and future developments of noninvasive treatment of human urinary stones with extracorporeal shock wave lithotripsyJ Urol1411989782789
- D.BonB.DoreJ.IraniM.MarroncleJ.AubertRadiographic prognostic criteria for extracorporeal shock-wave lithotripsy. A study of 485 patientsUrology481996556561
- D.E.ZilbermanM.N.FerrandinoG.M.PremingerE.K.PaulsonM.E.LipkinD.T.BollIn vivo determination of urinary stone composition using dual energy computerized tomography with advanced post-acquisition processingJ Urol184201023542359
- P.JosephA.K.MandalS.K.SinghP.MandalS.N.SankhwarS.K.SharmaComputerized tomography attenuation value of renal calculus: can it predict successful fragmentation of calculus by extracorporeal shock wave lithotripsyJ Urol167200219681971
- N.P.GuptaM.S.AnsariP.KesarvaniA.KapoorS.MukhopadhyayRole of computed tomography with no contrast medium enhancement in predicting the outcome of extracorporeal shockwave lithotripsy for urinary calculiBJU Int95200512851288
- L.J.WangY.C.WongC.K.ChuangS.H.ChuC.S.ChenL.C.Seeet alPrediction of outcomes of renal stones after extracorporeal shock wave lithotripsy from stone characteristics determined by unenhanced helical computed tomography: a multivariate analysisEur Radiol15200522382243