
Abstract
Objective:
To perform an economical single-step renal dilatation (RD) during percutaneous nephrolithotomy (PCNL), using directly a 30-F Amplatz dilator over the central Alken dilator, in a trial to reduce the operative duration and radiation exposure during RD while avoiding an exchange of dilators that might increase the risk of blood loss.
Patients and methods:
In a prospective randomised study including 49 patients divided into two groups, the first had RD before PCNL using the standard metallic telescopic dilators (Alken), and the second had RD using the 30-F Amplatz dilator over the central Alken dilator. The operative duration, with X-ray exposure, was calculated. The procedure outcome in terms of complications, stone-free rates and hospital stay was evaluated statistically.
Results:
The tract was dilated correctly in all cases. The operative duration and X-ray exposure was shorter in patients undergoing single-step RD (P < 0.05). There were perioperative complications, according to the Clavien grading system, in 17 (34%) patients but there was no statistically significant difference between the groups. The stone-free rates were comparable in both groups.
Conclusion:
A single-step RD during PCNL is feasible, with a shorter operative duration and X-ray exposure. The outcomes were comparable with those of a standard metallic telescopic RD.
Introduction
Percutaneous nephrolithotomy (PCNL) is an effective treatment for renal stones of >2 cm. This technique is associated with high success rates, decreased morbidity and fewer complications than is conventional renal stone surgery [Citation1]. An important and integral step in PCNL is renal puncture and tract dilatation with insertion of the access sheath, but during these steps bleeding can occur, although it usually responds to the tamponade effect provided by the access sheath [Citation2].
There are currently three standard methods for renal dilatation (RD), i.e., metal telescoping dilators (Alken), sequential fascial dilators (Amplatz), and the one-step balloon dilatation.
Metal telescopic dilators are reusable and thus more economical, and they maintain a tamponade effect throughout the dilatation. Previous reports suggest no difference between metallic and sequential fascial dilatation in terms of safety and efficiency [Citation3]. Fascial dilators are disposable and it has been suggested that during sequential dilator exchanges, the tamponade effect on the renal parenchymal tract is lost, which can lead to more blood loss during the exchange process [Citation4]. Both metallic and sequential fascial dilators are time-consuming to use, with an increased incidence of kinking of the guidewire during tract development, thus hindering adequate RD.
In an attempt to reduce the blood loss from the repetitive passage of progressively larger dilators, the one-step balloon dilatation was developed. The reduced blood loss is thought to be due to the constant pressure applied on the renal parenchyma during dilatation before the sheath is advanced. The disadvantages of this method are its cost and that it is not reusable [Citation5].
Thus in this study we assessed the use of an economical single-step RD using directly the 30-F Amplatz dilator over the central Alken dilator in a trial to reduce the operative duration and radiation exposure during RD, while avoiding an exchange of dilators that might increase the risk of blood loss.
Patients and methods
This was a prospective randomised study conducted between March 2013 and March 2014, initially including 67 patients with large (>2 cm) and/or multiple renal stones amenable to PCNL. The study followed the tenets of the Declaration of Helsinki, with an informed consent signed by all the patients who were included. Patients excluded were those with recurrent renal surgery on the same side, a body mass index (BMI) of >35 kg/m2, and uncorrected coagulopathies. Finally, 49 patients were divided into two groups, using sealed envelopes, with the first having tract dilatation using metallic telescopic dilators (Alken), and the second having tract dilatation in a single step using the 30-F Amplatz dilator over the central Alken dilator using the following technique.
Cystoscopy was done with insertion of an open-tip 7-F ureteric catheter, followed by renal puncture in the prone position and insertion of both the first and safety guidewire. The lumbodorsal fascia was punctured and split using a long haemostat under fluoroscopy (). The central Alken dilator was advanced over the guidewire and this was followed by directly inserting the 30-F Amplatz dilator, with the surgeon applying constant pressure and slowly advancing the dilator and then the access sheath under fluoroscopy (). We then used a 27-F nephroscope with a ballistic energy source for stone disintegration.
Figure 1 Puncture of the lumbodorsal fascia.
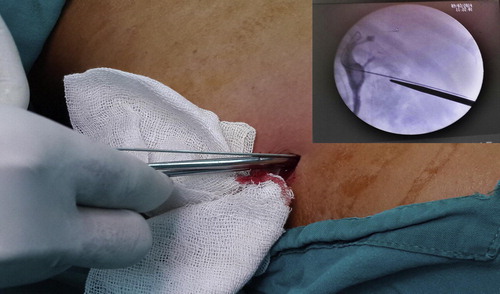
Figure 2 RD using the 30-F Amplatz dilator.

The operative duration (calculated from the time of cystoscopy to securing the 30-F nephrostomy tube to the skin) and that of fluoroscopic exposure were recorded at the end of the procedure. Haemodynamic changes and any need for transfusion were evaluated and recorded during the first 24 h after surgery. Any perioperative complications were classified according to the modified Clavien grading system. The total hospital stay was evaluated for each group.
The data obtained were assessed statistically, with P < 0.05 considered to indicate statistical significance.
Results
Patients having tract dilatation using the single-step technique were statistically significantly older than those having their tract dilated using the Alken dilators; otherwise there were no differences in the clinical variables between the groups ().
Table 1 Perioperative variables and outcome of the procedures.
In all patients there was renal access with correct tract dilatation, and the operative duration and that of fluoroscopy exposure was statistically significantly longer when using the Alken dilators than with the single-step RD ().
The stone-free rate was assessed using a plain abdominal film on the day after surgery, with residual fragments of <5 mm considered to be clinically insignificant. There were residual fragments in three (6%) of the 49 patients. There was no significant difference in stone-free rates between the groups. There was no statistically significant blood loss (comparing haemoglobin levels before and after surgery) in both groups, or between the postoperative values in both groups. A blood transfusion was needed in two patients, one from each group. There were complications, according to the modified Clavien grading system, in 17 (34%) patients; seven (41%) had grade 1 complications, with grade 2 and 3 complications in eight (47%) and two (12%), respectively. There was no statistically significant difference in complication rates between the groups, and no reported organ injury in any patient.
In the absence of complications, patients were discharged on the same day the urinary catheter was removed, and there was no statistically significant difference in the duration of hospital stay between the groups ().
Discussion
Tract dilatation is an essential step in PCNL, and inadequate RD can hinder the introduction of the access sheath and provoke bleeding. RD is classically done using metallic telescopic dilators (Alken), sequential fascial dilators (Amplatz), and single-step balloon dilator. Although all three methods are usually safe, reports show a higher blood loss for metallic telescopic RD than for the Amplatz and balloon dilatation [Citation6].
In the present study the duration of X-ray exposure was statistically lower for single-step Amplatz RD than for metallic RD. A shorter X-ray exposure was also reported by Frattini et al. [Citation7], who used one-step RD with a 25-F or 30-F Amplatz dilator to gain renal access.
In the present study the overall operative duration when using the single-step Amplatz RD was significantly shorter than when using Alken dilators, and to the best of our knowledge this is the first study to consider the overall operative duration including the time taken to insert the ureteric catheter, as older series only evaluated the fluoroscopy time and/or time to gain renal access and stone disintegration [Citation7–Citation9].
The single-step Amplatz RD was safe and effective [Citation10], and in the present study the stone-free rates were comparable in both groups, as were the complication rates, which also did not differ between the groups.
Although not objectively measured nor compared statistically, the cost of using the reusable telescopic metallic dilators (Alken) and the single-step 30-F Amplatz dilator is apparently lower than for the non-reusable balloon dilator.
The present study had several limitations, as it included relatively few patients, did not consider the effect of previous renal surgery, and did not test the efficiency of this technique when supracostal renal access was used.
In conclusion, the single-step Amplatz RD is a time-saving procedure, being safe, subjectively economical and an effective technique to gain renal access. We found no specific complication with this technique, and the morbidity rates were comparable with those of the classical metallic telescopic RD. We recommend its use for patients undergoing PCNL.
Conflict of interest
None.
Source of funding
None.
Notes
Peer review under responsibility of Arab Association of Urology.
References
- V.G.BirdB.FallonH.N.WinfieldPractice patterns in the treatment of large renal stonesJ Endourol172003355363
- A.P.GanpuleD.H.ShahM.R.DesaiPostpercutaneous nephrolithotomy bleeding aetiology and managementCurr Opin Urol24L2014189194
- H.U.OzokL.SagnakA.B.SenturkN.KarakoyunluH.TopalogluH.ErsoyA comparison of metal telescopic dilators and Amplatz dilators for nephrostomy tract dilation in percutaneous nephrolithotomyJ Endourol262012630634
- M.P.YuhicoR.KoThe current status of percutaneous nephrolithotomy in the management of kidney stonesMinerva Urol Nefrol602008159175
- K.L.LeeM.L.StollerMinimizing and managing bleeding after percutaneous nephrolithotomyCurr Opin Urol172007120124
- C.DehongL.LiangrenL.HuaweiW.A.QiangComparison among four tract dilation methods of percutaneous nephrolithotomy: a systematic review and meta-analysisUrolithiasis412013523530
- A.FrattiniA.BarbieriP.SalsiN.SebastioS.FerrettiE.Bergamaschiet alOne shot. A novel method to dilate the nephrostomy access for percutaneous lithotripsyJ Endourol152001919923
- S.FalahatkarH.NeiroomandM.AkbarpourS.A.EmadiN.KhakiOne-shot versus metal telescopic dilation technique for tract creation in percutaneous nephrolithotomy. Comparison of safety and efficacyJ Endourol232009615618
- M.AmjadiA.ZolfaghariA.ElahianA.TavoosiPercutaneous nephrolithotomy in patients with previous open nephrolithotomy: one-shot versus telescopic technique for tract dilatationJ Endourol222008423425
- S.AmirhassaniS.H.Mousavi-BaharA.Iloon KashkouliS.TorabianComparison of the safety and efficacy of one-shot and telescopic metal dilatation in percutaneous nephrolithotomy: a randomized controlled trialUrolithiasis422014269273