
Abstract
Objective:
To evaluate the efficacy and safety of bipolar transurethral resection of the prostate (TURP) in patients with a large prostate (>90 g), as a significant recent modification of TURP is the incorporation of bipolar technology, which uses the same technique as monopolar TURP but with normal saline as the irrigant.
Patients and methods:
Forty patients with a prostate of >90 g and who were considered at risk for monopolar TURP were treated by bipolar TURP. The operative duration, resection time, resected tissue weight, resection rate, resection ratio, amount of irrigation fluid used, the decrease in intraoperative haemoglobin level, haematocrit and serum sodium levels, and the blood loss were recorded. The follow-up data were analysed.
Results:
The mean (SD) operative duration was 116.3 (25.52) min, the resection time was 106.5 (25.69) min, the resected volume was 78.9 (20.58) g, the decrease in haemoglobin levels was 1.67 (0.46) g/dL, the mean serum sodium decline was 2.60 (0.68) mmol/L, and the blood loss was 532 (101.2) mL. The blood loss/g of resected tissue was 6.85 (0.70) mL. The mean (SD) postoperative bladder irrigation time was 2.0 (0.32) days, the catheterisation time was 3.25 (0.55) days and the postoperative hospital stay was 3.25 (0.55) days.
Conclusion:
Bipolar technology makes it possible to use TURP to treat patients with very large prostates and who are at risk when treated by the standard monopolar technology, with a satisfactory safety profile and with favourable efficacy.
Introduction
BPH is a disease of older men and thus comorbid conditions are common. The complications of TURP have been reduced over the last two decades due to advances in technology and mechanics. However, concerns remain about complications, such as TUR syndrome, blood loss and urethral strictures [Citation1]. Despite the introduction of alternative procedures, TURP is still the standard operation for managing BPH in small and medium-sized prostates [Citation2]. TURP has undergone many modifications over the last two decades to decrease the rate of perioperative complications [Citation1].
Different types of irrigant solutions have been used for TURP, e.g., distilled water, sorbitol, glycine, mannitol and normal saline. Fluid absorption during TURP is inevitable and carries the risk of developing TUR syndrome, with serious morbidity and mortality [Citation3]. Normal saline as an isotonic solution is the most physiological irrigant for TURP, but it conducts electricity and this prohibits its use with conventional monopolar TURP [Citation4]. A significant recent modification of TURP is the implementation of bipolar technology. Bipolar TURP uses the same technique as monopolar TURP but can be done using normal saline as the irrigant, and thus bipolar TURP is now being widely used [Citation5].
The principles of bipolar resection using high-frequency current have been tested experimentally and clinically by different manufacturers [Citation6]. Bipolar TURP is similar to monopolar TURP, but requires a specialised resectoscope and loops that can return the current through the loop or within the inner sheath. As it permits cutting in a conductive saline medium, this allows the operation to be performed using normal physiological saline. The cutting loop electrode can also be used to coagulate, and modifications of the electrode also allow tissue vaporisation [Citation7].
The advantages of bipolar resection are the use of normal saline as an irrigant, reducing the risk of TUR syndrome, and an improvement in haemostasis, resulting in better intraoperative visualisation, a shorter catheterisation time and reduced hospital stay [Citation8].
There are many types of bipolar devices in the market, e.g., a controlled tissue-resection system (ACMI, Marlborough, MA, USA), a plasmakinetic system (Gyrus ACMI, Southborough, MA, USA), and transurethral resection in saline (TURis, Olympus, Tokyo, Japan) [Citation1], and thus bipolar TURP is not a homogenous technique. The efficacy and the safety of each bipolar device must be evaluated separately [Citation9].
The aim of the present study was to determine whether bipolar TURP adds any advantage to standard TURP in patients with large prostates who are at risk if treated by standard monopolar TURP, and if bipolar TURP is safe and effective. Thus we evaluated the efficacy and safety of bipolar TURP in patients with a large prostate (>90 g).
Patients and methods
Forty patients with a prostate of >90 g and who were considered at risk using monopolar TURP were treated using bipolar TURP by one surgeon who had extensive experience (10 years) in monopolar TURP. The study was conducted at the authors’ institution between 2011 and 2013, as a prospective study. The indications for TURP included moderate to severe LUTS not responding to medical treatment, refractory retention due to prostatic obstruction, recurrent haematuria due to BPH, effects on the upper urinary tract system and recurrent UTIs due to prostatic enlargement.
An informed consent was obtained from all patients, and all patients were assessed by a detailed medical history, physical examination, laboratory evaluation and uroflowmetry study.
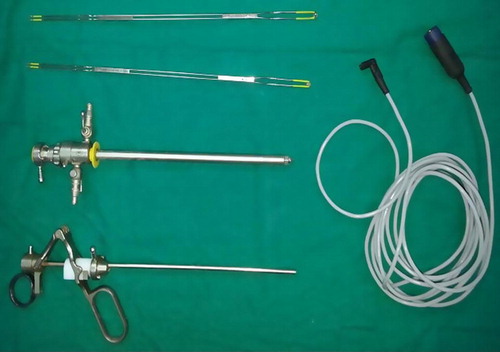
We used the TURis system (ERBE VIO 300 D, Gyrus), which is compatible with the Karl-Storz bipolar TURP system, using a cutting mode setting of 200–280 W and a coagulation mode setting of 80–120 W. We used a 26-F continuous-flow resectoscope with a rotating inner tube and separate irrigation channels, an active bipolar working element from Karl-Storz, and bipolar cutting and vaporising loop electrodes (all Karl-Storz, Germany). The irrigant used was isotonic 0.9% saline at room temperature ( and ).
Figure 1 Cutting and vaporising bipolar loops.

Figure 2 26-F continuous-flow resectoscope, working element, cutting and vaporising loop electrodes, and bipolar cord.
The surgical technique for bipolar TURP is similar to that for monopolar TURP, with a few differences. The resection is started at the bladder neck, followed by resection of the lateral lobes and then the anterior lobe, with the apical tissue resected last. During the ‘cutting’ resection in bipolar TURP, the ‘plasma corona’ should be developed before starting the resection. The cutting loop should be held away from the prostate tissue by a few millimetres when initiating the cutting current via the foot pedal. The prostate chips are created in a way similar to those in monopolar TURP and are displaced into the bladder by the inflow of the saline solution. The chips are then removed from the bladder. If there is a delay between operating the cutting switch and initiation of the plasma corona there is probably charred tissue on the surface of the loop. When that occurs the loop should be placed away from tissues and this allows the plasma to be formed for a few seconds, which cleans the loop. During coagulation, no plasma is formed, and instead a whitish area around the coagulated point is visible. Bipolar TURP has the advantage of vaporising the adenoma in areas that are difficult to be resected by the cutting loop.
Importantly, there should be no dilutional hyponatraemia with bipolar TURP, but volume overload is a potential risk, so the regular administration of a loop diuretic (furosemide 40 mg) after an hour of surgery is recommended.
The operative data recorded were the type of anaesthesia, operative duration, resection time (the time from starting the resection until the insertion of the three-way urethral catheter), resected tissue weight, resection rate (resected tissue weight/resection time), resection ratio (resected tissue volume/total prostate volume), amount of irrigant used, and the declines in intraoperative haemoglobin level, haematocrit and serum sodium. The blood loss was estimated from the preoperative haemoglobin concentration, volume of irrigant used, and haemoglobin concentration in the irrigation fluid return obtained immediately after finishing the procedure. The irrigant return should be heparinised during the procedure by adding 1500 IU of heparin/8 L of irrigant return, then uniformly mixed to prevent coagulation of the blood contents. The blood loss was then calculated as reported previously [Citation10,Citation11], i.e., the preoperative haemoglobin concentration, minus that in the irrigant return (g/dL) × volume (L) × 1000. The rate of blood loss (amount of blood loss/resection time) and the amount of blood lost/g of resected tissue were also calculated. Intraoperative complications and blood transfusions when indicated were recorded.
The postoperative evaluation included vital signs (pulse, blood pressure, and temperature), immediate complete blood count and serum sodium levels, analgesic requirements, the need for blood transfusion, bladder irrigation time, catheterisation time, hospital stay, and complications, if present. All patients were followed for ⩾1 year using the IPSS, uroflowmetry and measurements of maximum urinary flow rate (Qmax) and the postvoid residual urine volume (PVR).
The results were assessed statistically by a univariate analysis of the pre and post-operative IPSS, PVR and Qmax (at 1 month and 1 year) using the Wilcoxon test.
Results
The mean (SD) age of the patients was 67.7 (3.96) years. Twelve (30%) presented in acute urinary retention, 28 (70%) had moderate to severe LUTS, and 26 (65%) had associated comorbidities in the form of diabetes mellitus, hypertension, cardiac diseases, and renal impairment. The mean baseline data and values immediately after TURP are summarised in .
Table 1 Baseline data and values immediately after TURP.
Complications during the first month after TURP were classified according to the modified Clavien system [Citation12]. The grade I complications included haematuria with or without blood clot retention in three patients, and they were managed by bedside bladder irrigation. Another three patients developed a UTI and they were managed by antibiotics. The grade II complications included one patient who developed hypertension and signs of volume overload; he had a history of ischaemic heart disease, and this complication was managed by the anaesthesiologist using furosemide diuretics (0.1 mg/kg) as an initial bolus dose, followed by 0.1 mg/kg/h. The dose could be doubled every 2 h to a maximum of 0.4 mg/kg/h, guided by central venous pressure. Another two patients required blood transfusion after TURP when the haemoglobin level was <10 g/dL, and one unit of blood was transfused to each patient.
All patients were followed up by assessing the IPSS, Qmax and PVR, with results after 1 month for 38 and at 1 year for 31 patients ().
Table 2 Univariate analysis comparing variables before, and at 1 month and 1 year after TURP, using the Wilcoxon test.
At 9 and 11 months respectively, two patients complained of lower urinary tract obstructive symptoms, with recurrent attacks of UTI, and investigations showed a bulbar urethral stricture that was managed endoscopically by visual internal urethrotomy.
Discussion
There are other studies of bipolar TURP in patients with large prostate glands, and summarises the data of the present and other studies [Citation13–Citation16]. Kan et al. [Citation16] reported a mean (SD) operative duration of 87.0 (34.3) min, a resected volume of 45.7 (18.2) g, and mean declines in haemoglobin of 1.1 (1.0) g/dL, and a serum sodium level of 0.5 (3.2) mmol/L, and with only one case of intraoperative bleeding in the bipolar TURP group. Their results are comparable to those in the present study, and the differences were due to the smaller baseline prostate size they selected.
Table 3 A comparison of the results before and after TURP in the present study and other similar studies.
Kwon et al. [Citation15] also reported similar results in their bipolar TURP group, with a mean operative duration of 132.9 (49.8) min, a resected volume of 41.4 (11.9) g, a resection rate of 0.34 (0.11) g/min and an intraoperative decline in haemoglobin of 1.2 (1.0) g/dL and a sodium level of 1.1 (2.2) mmol/L, with no severe intraoperative bleeding that required a blood transfusion, and no significant intraoperative complications.
The present results are also similar to those of Finley et al. [Citation13], who reported a mean resection time of 163 min and a mean resected tissue weight of 80.8 g. A mean of 6.1 L of saline was used, with a mean decline in haemoglobin of 2.1 g/dL and in serum sodium of 3.3 mmol/L, with no patient requiring a blood transfusion. Bhansali et al. [Citation14] reported that bipolar TURP might be advantageous for reducing the blood loss in men with a large prostate, as they reported significantly less blood loss in the bipolar TURP group (196 mL) than with conventional TURP (361.5 mL).
In the present study two patients required blood transfusion and there were only three with complications (one with haematuria and clot retention, and two with recurrent attacks of UTI and urethral stricture). These results are comparable to those of Kwon et al. [Citation15], who reported no complications in the bipolar TURP group. The hospital stay was 6.3 (1.3) days in their bipolar group, which was significantly shorter than that of the monopolar TURP and open prostatectomy groups, and there was no need for a blood transfusion in the bipolar group. They reported two cases of TUR syndrome and three patients (16%) required blood transfusions in the monopolar TURP group.
Finley et al. [Citation13] reported a mean catheterisation time of 76 h and a mean hospital stay of 12 h, the shorter hospital stay being due to the postoperative protocol, as patients were discharged with a urethral catheter in situ as soon as their urine became clear. They also reported that no patient required blood transfusion and there were no complications during or after TURP.
Kan et al. [Citation16] reported a mean hospital stay of 4.8 (2.5) days; six patients (7%) received blood transfusions and 11 (13%) developed complications in the form of retention of urine, readmission for haematuria, and re-operations for prostatic enlargement and urethral stricture.
Bhansali et al. [Citation14] reported transfusion rates of 6% and 21% in their bipolar and monopolar TURP groups, respectively, and the catheterisation time was 19.5 h in the bipolar group, vs. 39.3 h in the monopolar group, which was statistically significant. The hospital stay was shorter in the bipolar than in the monopolar group (1.4 vs. 2.6 days).
In the present study there were significant improvements (P < 0.001) in all the follow-up variables compared to the baseline values (). Kwon et al. [Citation15] also reported a highly significant improvement in the IPSS and Qmax from baseline values after bipolar TURP in large prostates (>100 g) at 3 months after TURP (). This was also in accord with the results of Kan et al. [Citation16], who reported a significant improvement in the IPSS and Qmax from baseline values after bipolar TURP in large prostates of >100 g (). Finley et al. [Citation13] reported that the mean IPSS and PVR reflected a significant improvement from baseline values after bipolar TURP for such large prostates. This was comparable to the results of Bhansali et al. [Citation14] who also reported a highly significant improvement in IPSS and Qmax from baseline after bipolar TURP in large prostates (>70 g) at a mean of 3 months of follow-up ().
In conclusion, despite the relatively few patients and short follow-up in the present study, bipolar technology allowed TURP in patients with very large prostates and who were at risk if treated by standard monopolar TURP, with a satisfactory safety profile and with favourable efficacy. The higher resection speed due to better vision and better haemostasis, in combination with absence of time-limiting risk factors, enabled the surgeon to resect as much prostatic tissue as possible.
Conflict of interest
None.
Source of Funding
None.
Notes
✰ This journal is partially supported by Karl Storz GmbH. That support had no influence on the peer-review of this paper, which was entirely independent of Karl Storz.
Peer review under responsibility of Arab Association of Urology.
References
- J.RassweilerD.TeberR.KuntzR.HofmannComplications of transurethral resection of the prostate (TURP) – incidence, management, and preventionEur Urol502006969979
- S.MadersbacherG.AlivizatosJ.NordlingC.R.SanzM.EmbertonJ.J.de la RosetteEAU 2004 guidelines on assessment, therapy and follow-up of men with lower urinary tract symptoms suggestive of benign prostatic obstruction (BPH guidelines)Eur Urol462004547554
- R.G.HahnFluid absorption in endoscopic surgeryBr J Anaesth962006820
- H.SinghM.R.DesaiP.ShrivastavK.VaniBipolar versus monopolar transurethral resection of prostate: randomized controlled studyJ Endourol192005333338
- C.MamoulakisM.TrompetterJ.de la RosetteBipolar transurethral resection of the prostate: the ‘golden standard’ reclaims its leading positionCurr Opin Urol1920092632
- H.BottoT.LebretP.BarreJ.L.OrsoniJ.M.HerveP.M.LugagneElectrovaporization of the prostate with the Gyrus deviceJ Endourol152001313316
- M.M.IssaTechnological advances in transurethral resection of the prostate: bipolar versus monopolar TURPJ Endourol22200815871595
- J.S.StarkmanR.A.SantucciComparison of bipolar transurethral resection of the prostate with standard transurethral prostatectomy: shorter stay, earlier catheter removal and fewer complicationsBJU Int9520056971
- P.FaulB.SchlenkerC.GratzkeC.G.StiefO.ReichR.G.HahnClinical and technical aspects of bipolar transurethral prostate resectionScand J Urol Nephrol422008318323
- J.EkengrenR.G.HahnBlood loss during transurethral resection of the prostate as measured by the HemoCue photometerScand J Urol Nephrol271993501507
- R.G.HahnT.FagerstromT.L.TammelaO.Van Vierssen TripH.O.BeislandA.Dugganet alBlood loss and postoperative complications associated with transurethral resection of the prostate after pretreatment with dutasterideBJU Int992007587594
- C.MamoulakisI.EfthimiouS.KazoulisI.ChristoulakisF.SofrasThe modified Clavien classification system. A standardized platform for reporting complications in transurethral resection of the prostateWorld J Urol292011205210
- D.S.FinleyS.BeckR.J.SzaboBipolar saline TURP for large prostate glandsScientific World J7200715581562
- M.BhansaliS.PatankarS.DobhadaS.KhaladkarManagement of large (>60 g) prostate gland: PlasmaKinetic Superpulse (bipolar) versus conventional (monopolar) transurethral resection of the prostateJ Endourol232009141145
- J.S.KwonJ.W.LeeS.W.LeeH.Y.ChoiH.S.MoonComparison of effectiveness of monopolar and bipolar transurethral resection of the prostate and open prostatectomy in large benign prostatic hyperplasiaKorean J Urol522011269273
- C.F.KanH.L.TsuY.ChiuH.C.ToB.SzeS.W.ChanA prospective study comparing bipolar endoscopic enucleation of prostate with bipolar transurethral resection in saline for management of symptomatic benign prostate enlargement larger than 70 g in a matched cohortInt Urol Nephrol462014511517