
Abstract
Objectives:
To evaluate the effectiveness of laparoscopic pyelolithotomy (LP) for staghorn stones (>3–4 cm) in patients with chronic liver disease or coronary artery disease.
Patients and methods:
In all, 49 patients underwent LP; they were divided into four groups, with stones in group 1 in the renal pelvis only, in group 2 in the renal pelvis and one calyx, in group 3 in the renal pelvis and two calyces, and in group 4, in the renal pelvis and more than two calyces. Patient demography, stone characteristics, surgical outcomes and complications were evaluated.
Results:
The mean stone-free rate in one session was 90% among all groups. The mean (SD) stone size was 4.27 (1.72) cm. The stone-free rate decreased with greater stone burden, but the operative time, estimated blood loss and need for ancillary procedures increased with stone burden. No blood transfusion was required and one patient each in groups 2 and 4 had a urine leak.
Conclusion:
LP provides acceptable results in complex cases for managing renal stone disease with a larger stone burden in high-risk situations.
Introduction
Several methods have been established for managing different types of renal stones, based on stone location and distribution, e.g., ESWL, percutaneous nephrolithotomy (PNL) and ureterorenoscopy (URS) [Citation1]. The clearance rate of stones relies mainly on factors such as the stone bulk, location, composition and collecting system anatomy [Citation2–Citation6]. The complexity of stone distribution within the kidney can sometimes be a hindrance for clearing stones in one session with these established techniques. Several sessions are required in such cases and even a combination of different methods is required to completely clear the stones. Several sessions incur more expenditure and more complications. PNL, considered the standard for stones of >2 cm in complex situations, is associated with a greater risk of renal parenchymal injury or massive bleeding perioperatively. Alternatives are retrograde intrarenal surgery or laparoscopic pyelolithotomy (LP, introduced over 20 years ago [Citation7]), but the application of LP in clinical practice remains limited as it requires sufficient skill, more invasiveness, prolonged surgery, and an increased hospital stay [Citation8].
The standard indications for LP, especially in cases of ectopic kidneys, horseshoe kidney, concomitant PUJ obstruction, etc., have been reported but there is still no standardisation, as there are no specific guidelines for its use as a primary method in high-risk patients where PNL carries a considerable high risk, e.g., in patients with severe comorbidities such as coronary artery disease (CAD) or chronic liver disease (CLD).
LP in such patients with renal stones gives a satisfactory clearance rate comparable to PNL for similar stones in normal low-risk patients [Citation9–Citation12]. Thus in the present study we determined the effectiveness of LP as a primary method in high-risk patients with complex renal stones, e.g., those with CAD or CLD, assessing the stone-free rate (SFR) for one session and where PNL was risky. We also analysed whether the stone burden and stone distribution influenced the SFR after one session of LP.
Patients and methods
This retrospective study was done between August 2005 and February 2013. In all, 49 patients with high-risk factors (32 with CAD and on anticoagulation, and 17 with CLD, Child–Pugh criteria A), underwent LP as the primary treatment at our institution for large or multiple renal stones.
The anticoagulation in patients with CAD was stopped 1 day before surgery and overnight low molecular-weight heparin (enoxaparin 0.2 mL subcutaneously) was given as an institutional bridging-therapy protocol. Patients were assigned to four groups according to stone location, so that group 1 had stones only in the renal pelvis, group 2 in the renal pelvis and one renal calyx, group 3 in the renal pelvis and two calyces, and group 4 in the renal pelvis and more than two calyces.
Data were collected retrospectively from medical records after obtaining clearance from the institutional ethics review board. All patients had a preoperative evaluation with a haemogram, serum creatinine level, bleeding profile and urine analysis, with a urine culture and sensitivity report. A plain abdominal film and unenhanced CT were used to evaluate the stone location. Stone size was measured using the axial dimensions of renal stone(s) on the CT scan.
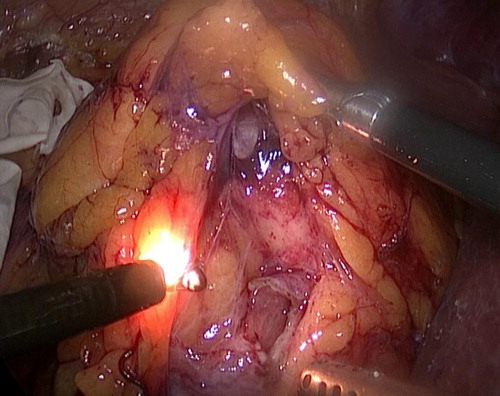
Patients underwent LP via the standard transperitoneal approach (modified flank position) as previously described by Salvado et al. [Citation7]; the port configuration is shown in . The large bowel was reflected medially after incising the peritoneum along the white line of Toldt. An avascular plane was created between the fusion fascia and Gerota’s fascia to trace the gonadal vessels and ureter, and to reach the hilum. Using the Gil-Vernet technique the renal hilum was explored, and the main renal vessels were identified and safeguarded. The classical modified Gil-Vernet technique was used for renal pelvic dissection, as shown in . A pyelotomy was done as in open surgery, in a V-shaped manner, and with the creation of a flap using needle electrocautery. Stones in the pelvis were then removed using stone-grasping forceps (). The entire pelvicalyceal system was evaluated using a flexible instrument (cystoscope) through one of the instrument ports, and calyceal stones were retrieved from the kidney using a tri-prong forceps, grasper or stone basket, through the cystoscope (). Retrieved stones were placed in a rubber-glove basket under vision (). Occasionally stones were found in calyces with a narrow infundibulum, which were accessed with the help of gentle dilatation using ureteric PTFE dilators from 8 to 12 F, sufficient to negotiate a flexible ureteroscope access sheath (9/11 F) and thus, with the use of minimal irrigation, stones can be fragmented to gravel or powder using the holmium-YAG laser (365 nm). In the initial few patients there was stone slippage, but stones were never lost in the peritoneal cavity. We routinely use a technique of pre-placing the handmade rubber-glove (No. 8) finger bag and safeguard the large pieces in that. Gravel was safely removed with suction.
Figure 1 Port placement for LP by the transperitoneal approach.
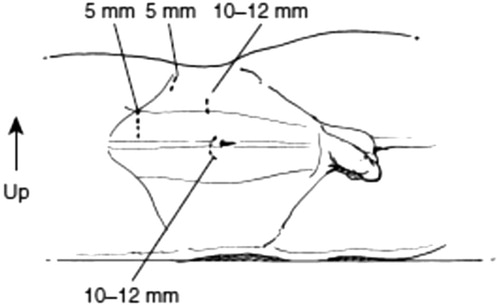
Figure 2 Using the Gil-Vernet technique for dissecting the renal parenchyma and proceeding with pyelotomy with hook cautery.
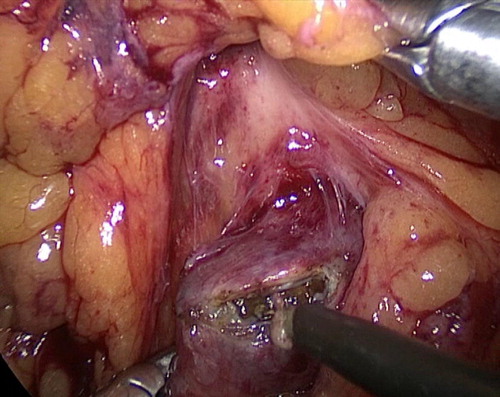
Figure 3 Placement of the retrieved stone in a glove-finger bag using a stone grasper after pyelotomy.
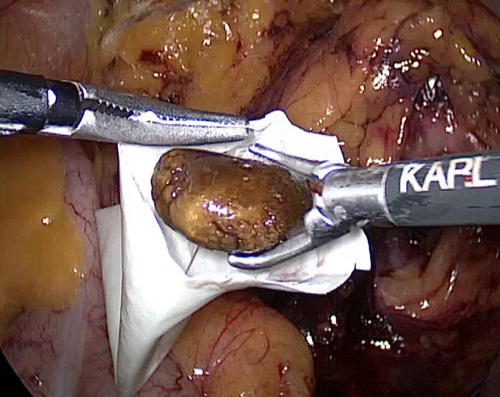
Figure 4 Using a flexible cystoscope through one of the ports for retrieving calyceal fragments.
A 6/24 F JJ stent was placed via the pyelotomy incision with a guidewire. The incision was closed using an interrupted 4/0 polyglycolic acid suture. A Jackson-Pratt #7 drain was placed in the pararenal space and removed when the drain output was <50 mL.
Clinical data were evaluated, including the demographic profile and stone characteristics. Surgical outcomes were assessed as the mean operating time, estimated blood loss (EBL), perioperative analgesic consumption and hospital stay. Patients were followed up after surgery with a plain abdominal film to assess the immediate SFR. Low-dose noncontrast CT (NCCT) was used to evaluate any residual stones after 6 weeks, before the JJ stent was removed, and at 3 months after surgery to assess the SFR. LP was undertaken by surgeons who regularly used laparoscopic renal surgery in patients considered unfit for PNL because of the risk of bleeding due to comorbidities. Also, single-session stone clearance was the aim when selecting LP, because of the high risk of repeated anaesthesia if several sessions were required for stone clearance.
In the present study the primary endpoint was to determine the single-session SFR and to compare the clearance rates in relation to the complexity of stone bulk in the four groups. The SFR was defined as no visible fragments or delayed excretion on low-dose NCCT at 3 months after surgery.
The results were analysed statistically using the Kruskal–Wallis test for continuous variables and Pearson’s chi-squared test for categorical variables, with P < 0.05 considered to indicate statistical significance. Values are presented as the mean (SD) for clinical variables.
Results
The characteristics of the patient and stones are shown in ; the mean (SD) age of the patients was 53.6 (14.10) years, and the age distribution was not statistically significantly different among the groups (P = 0.217). The gender distribution and side of the stone were also similar in all groups. The mean stone size was statistically significantly different among the groups, with smaller stones associated with a higher SFR in groups 1–3 vs. group 4 (P = 0.015).
Table 1 Demographic profile and stone characteristics, the surgical outcome.
The surgical variables are also compared in . All 49 LPs were undertaken with consent for open conversion. The SFRs (the primary endpoint) showed no obvious significant differences among the groups (P = 0.302), but the rates were 20/22 (91%), 9/9, 10/11 and 5/7 in groups 1–4, respectively. The lack of significance was probably a result of there being few patients in the study groups.
With increasing complexity in the location of renal stones there was an increase in the mean operative time, i.e., in group 4 the surgery took significantly longer (P = 0.011).
The mean EBL (% decline in haemoglobin level from before surgery) was significantly greater with increasing stone burden and complexity of location, e.g., in group 4 (P = 0.012). The stone number also affected the SFR significantly, with a greater SFR in groups 1–3 than in group 4 (P < 0.001). There was no statistically significant difference in the postoperative usage of analgesics and duration of hospital stay among the groups. (P = 0.139 and 0.175, respectively). During the procedure flexible URS was done in all patients through one port and this helped to clear residual stones in one patient in group 3 and in three in group 4, and there was then complete clearance. Three patients in group 1 and one each in groups 2–4 had associated PUJ obstruction that was managed with concomitant laparoscopic pyeloplasty. In all the patients the JJ stent was removed at the 6-week follow-up, except in one patient in group 1, one in group 3 and two in group 4, who had residual stones after surgery on NCCT after 6 weeks. Of these patients, one in group 1 and two in group 4 had the stone removed by URS and the patient in group 3 had one session of ESWL (2000 shock waves), with complete clearance of the stones.
The complications among the groups, graded according to modified Clavien–Dindo Grading System, are also shown in . None of the patients received a blood transfusion (grade II), and one each in groups 2 and 4 had a perirenal urine collection, which required percutaneous drainage (grade IIIa). However, the leak stopped after 10 days in both patients. One patient each in groups 1 and 3 had postoperative fever managed with antipyretics (grade I). One patient in group 3 had an upper ureteric stricture at 6 months that was managed with balloon dilatation (grade IIIb). None of the patients with CLD decompensated during the perioperative period.
Discussion
Clayman and Kavoussi were the pioneers in the development of ‘the art of laparoscopic surgery’ by performing the first laparoscopic nephrectomy in 1991 [Citation13]. Since then this approach has been used more frequently for many urological procedures. Minimally invasive surgery, especially robotic surgery, in urological practice gives easier manoeuvrability at tight angles during surgery. However, cost is a major consideration with the use of robotics. Laparoscopy has always been considered as a useful tool for managing many urological conditions, as it is less invasive, causes less pain and reduces the hospital stay. However, it is considered a little more invasive and less cosmetic than other more established procedures such as PNL for large stones [Citation8]. PNL is considered the standard for renal stones of >2 cm [Citation14], but some studies report the usefulness of LP in achieving SFRs of 88.9–100% for solitary renal pelvic stones in one session, especially when PNL is associated with multiple tracts and several sessions [Citation9–Citation12].
In the present study the SFR in group 1–4 was >90%, which is comparable to the results reported in many studies. LP can thus be considered an alternative and feasible method, as an adjunct to PNL in the management of renal stones in those with a large stone burden, especially in high-risk patients with multiple comorbidities, where making multiple punctures substantially increases the complications.
At our centre we routinely use PNL for large renal stones (>2 cm), but the SFR decreases when the stone burden and complexity of distribution increases. In our experience, after one session, the SFR at 3 months where the stone was >4 cm was ≈75% with PNL. Also, the multiplicity of procedures and additions to attain complete stone clearance incurs huge financial constraints, again emphasising that single-session stone clearance with minimal morbidity can be managed reasonably with the laparoscopic approach in these complex marginal patients.
Stone bulk and distribution have been considered important variables determining single-session SFRs. In general, ESWL is associated with a 45–99% clearance rate, based on stone distribution, bulk and fragility [Citation2–Citation4]. In a few series of patients treated with PNL, the single-session SFR was 51%, and upper calyceal stones and a greater bulk were associated with a lower SFR after one session in such settings [Citation5]. A SFR of 78.6% was also reported by Turna et al. [Citation6], which was again indicative of a diminished SFR with increasing stone bulk and a more complex distribution within the pelvicalyceal system.
Lee et al. [Citation13] reported the efficacy of LP in relation to stone distribution, and the results of their study were comparable to those in the present study. We also evaluated the single-session SFR with the safety of LP in high-risk patients, which is more critical from a surgical perspective.
Comparing the results of single-session SFRs in established studies that used PNL for complex stones with the present results showed excellent surgical outcomes for effectiveness and safety. In the present study, 44/49 (90%) patients were stone-free after LP for large renal stones, and five (10%) had residual stones after a one session, four of whom required secondary procedures, with one patient having spontaneous stone expulsion. Such rates are comparable to those in previous studies reporting SFRs of 51–100% after PNL [Citation14].
The present results are compared with those in previous series shown in [Citation9,Citation15,Citation16]. Overall SFRs of almost 90% were attained in one session for large staghorn calculi (>4 cm). Similarly, although the operation time, hospital stay and time to return to normal daily activity favours PNL over LP, the lower failure rate of the procedure, low blood transfusion rate and higher single-session SFRs for large/multiple complex renal stones favours LP [Citation17].
Table 2 A comparison of different series of LP with the present series.
Armitage et al. [Citation18] reported that the SFR at 1 day after surgery, according to stone size and characteristics, was 34% for complete staghorn stones, 56% for partial staghorn stones, 70% for stones of >2 cm, and 80–88% for stones of 1–2 cm, which are inferior results to those in the present series for LP, favouring LP for large renal stones as the procedure of choice.
A prospective study of PNL in 5803 patients reported complication rates of up to 11.1% [Citation19]. Also, Tefekli et al. [Citation20] reported a complication rate of 10.9% in 811 patients treated by PNL. In the present study the complications after LP were manageable, maintaining excellent effectiveness and safety of the procedure. Stone bulk and distribution are established factors in predicting the surgical outcome for ESWL and PNL. In the present study, group 4, with a greater diversity of stone distribution, had a lower single-session SFR. Hence, stone bulk and distribution also influence the outcomes for LP. In addition, with LP, using a flexible cystoscope the entire pelvicalyceal system can be explored and the results justify its more frequent use as a definitive procedure as an adjunct to PNL.
Similarly, in a 10-year experience of PNL in a tertiary-care centre, El Nahas et al. [Citation21] showed that several sessions were required in 30% and multiple punctures required in 35.5% of procedures. Similarly, the perioperative complication rate was 22% and the need for blood transfusion was 14%. The SFR with PNL monotherapy was only 56.6%, with an auxiliary procedure rate of 56.6%, finally attaining a 3-month SFR of 72.7% [Citation21], which was clearly inferior to the 3-month SFR of >90% in the present series, thus favouring LP over PNL for large renal calculi.
The present EBL in the different groups was related to the complexity of procedure (P = 0.012). With LP, removing the renal stones under vision avoids harm to the renal parenchyma. We found that LP can be a useful method for impacted pelvic or multiple calyceal stones within an extrarenal or dilated pelvis, in patients with borderline chronic kidney disease where the goal is to preserve the renal parenchyma, in those with coagulopathy, or CAD and on anticoagulation, and with CLD (Child–Pugh A) where bleeding can be a factor. Adequate renal sinus dissection using the Gil-Vernet technique adds further to facilitating the removal of remotely located calyceal stones if they are not accessible by flexible nephroscopy. Furthermore, LP is a reasonable option for complex renal stones, where ESWL, retrograde intrarenal surgery, or PNL might not be successful in one session.
Despite the few patients we believe that our results provide useful information on the role of LP and the predictive factors for the surgical outcome of LP for renal stone disease.
In conclusion, LP provides acceptable results, comparable with those from PNL in those with complex renal stones, especially in high-risk patients, with low morbidity and an early return to activity. The purpose of the present study was not to compete with endourological procedures, but to complement them in difficult situations of complexity for optimal patient outcomes with minimal morbidity.
Conflict of interest
None.
Source of funding
None.
Notes
Peer review under responsibility of Arab Association of Urology.
References
- K.KijvikaiThe role of laparoscopic surgery for renal calculi managementTher Adv Urol320111318
- T.EgilmezM.I.TekinM.GonenF.KilincR.GorenH.OzkardesEfficacy and safety of a new-generation shockwave lithotripsy machine in the treatment of single renal or ureteral stones: experience with 2670 patientsJ Endourol2120072327
- T.AbeK.AkakuraM.KawaguchiT.UedaT.IchikawaH.Itoet alOutcomes of shockwave lithotripsy for upper urinary-tract stones: a large-scale study at a single institutionJ Endourol192005768773
- M.TolonC.MirogluH.ErolJ.TolonD.AcarE.Bazmanogluet alA report on extracorporeal shock wave lithotripsy results on 1569 renal units in an outpatient clinicJ Urol1451991695698
- K.ShahrourJ.TomaszewskiT.OrtizE.ScottK.M.SternbergS.V.Jackmanet alPredictors of immediate postoperative outcomes of single-tract percutaneous nephrolithotomyUrology8020121926
- B.TurnaM.UmulS.DemiryoguranB.AltayO.NazliHow do increasing stone surface area and stone configuration affect overall outcome of percutaneous nephrolithotomy?J Endourol2120073443
- J.A.SalvadóS.GuzmánC.A.TruccoC.A.ParraLaparoscopic pyelolithotomy: optimizing surgical techniqueJ Endourol232009575578
- A.GoelA.K.HemalEvaluation of role of retroperitoneoscopic pyelolithotomy and its comparison with percutaneous nephrolithotripsyInt Urol Nephrol3520037376
- P.MeriaS.MilcentF.DesgrandchampsP.Mongiat-ArtusJ.M.DuclosP.TeillacManagement of pelvic stones larger than 20 mm: laparoscopic transperitoneal pyelolithotomy or percutaneous nephrolithotomy?Urol Int752005322326
- A.Al-HunayanH.AbdulhalimE.El-BakryM.HassaboE.O.KehindeLaparoscopic pyelolithotomy: is the retroperitoneal route a better approach?Int J Urol162009181186
- A.Al-HunayanM.KhalilM.HassaboA.HanafiH.Abdul-HalimManagement of solitary renal pelvic stone: laparoscopic retroperitoneal pyelolithotomy versus percutaneous nephrolithotomyJ Endourol252011975978
- A.TefekliA.TepelerT.AkmanM.AkçayM.BaykalM.A.Karadaget alThe comparison of laparoscopic pyelolithotomy and percutaneous nephrolithotomy in the treatment of solitary large renal pelvic stonesUrol Res402012549555
- S.W.LeeS.Y.ChoS.B.LeeLaparoscopic pyelolithotomy. Comparison of surgical outcomes in relation to stone distribution within the kidneyJ Endourol272013592597
- Türk C, Knoll T, Petrik A, et al., and members of the European Association of Urology (EAU) Guidelines Office. Guidelines on urolithiasis. In: EAU guidelines. 14th ed.; April 2014.
- R.SinhaN.SharmaRetroperitoneal laparoscopic management of urolithiasisJ Laparoendosc Adv Surg Tech A719979598
- J.ChanderM.SuryavanshiP.LalL.SinghV.K.RamtekeRetroperitoneal pyelolithotomy for management of renal calculiJSLS9200597101
- A.SkolarikosG.AlivizatosJ.J.de la RosettePercutaneous nephrolithotomy and its legacyEur Urol4720052228
- J.ArmitageS.IrvingN.BurgessPercutaneous nephrolithotomy in the United Kingdom. Results of a prospective date registryEur Urol61201211881193
- J.De la RosetteD.AssimosM.DesaiJ.GutierrezJ.LingemanR.Scarpaet alThe Clinical Research Office of the Endourological Society Percutaneous Nephrolithotomy Global Study: indications, complications, and outcomes in 5803 patientsJ Endourol2520111117
- A.TefekliM.Ali KaradagK.TepelerE.SariY.BerberogluM.Baykalet alClassification of percutaneous nephrolithotomy complications using the of percutaneous nephrolithotomy using the modified Clavien grading system: looking for a standardEur Urol532008184190
- A.El-NahasI.ErakyA.A.ShokeirA.M.ShomaA.M.El-AssmyPercutaneous nephrolithotomy for treating staghorn stones: 10 years of experience in a tertiary-care centreArab J Urol102012324329