
Abstract
Objective:
To determine the efficiency of the interscrotal approach to inguinoscrotal pathologies.
Patients and methods:
We report the use of the interscrotal approach in 21 boys, from September 2012 to November 2013, operated using an interscrotal access through a vertical incision on the median raphe.
Results:
The approach was used for bilateral inguinal hernia (48%), bilateral ectopic testis (19%), torsion of the spermatic cord (19%), testicular biopsy (10%) and webbing of the penis (5%).
Conclusion:
Inter-scrotal access is an option for inguinoscrotal pathologies, with the advantages of a single incision, much less dissection and disruption of tissue, and greater comfort for the ‘day-case’ child.
Keywords:
Introduction
We report our experience in 21 boys operated using a vertical incision on the median interscrotal raphe [Citation1], to determine the efficiency of this surgical approach in treating inguinoscrotal pathologies [Citation2].
Patients and methods
We used an interscrotal access in 21 boys from September 2012 to November 2013, operated by a vertical incision on the median raphe, for the pathologies listed in . Necessary approval was obtained from the institutional ethics committee and the patients provided informed consent for these procedures.
Table 1 The baseline characteristics and relevant pathologies of the 21 boys.
Technique
The patients were placed in a dorsal decubitus, with flexed thighs in abduction. The penis was compressed vertically in the midline and maintained by a compression dressing, an adhesive application to avoid mobility of the pelvis, with a soft padding around the iliac crests.
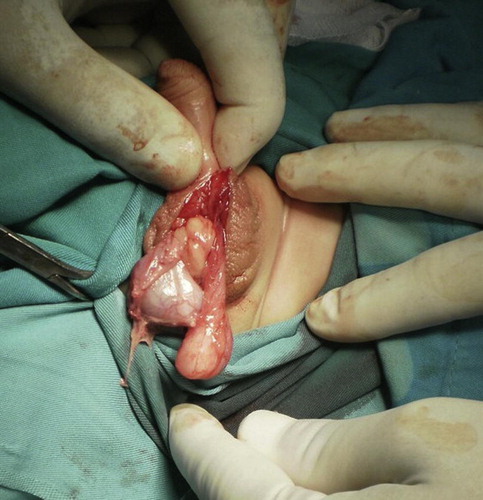
A vertical incision () was made on the median raphe of the scrotum [Citation3] (mono- and bipolar scalpel use is not desirable and was not used in this series) [Citation4] and then using a chisel and atraumatic clamp, the incision () was opened and dissected from the intrascrotal tunica up to the high subcutaneous inguinal region. At this level, the fascia of Scarpa is opened and dissected up to the anterior arch of the superficial inguinal ring [Citation5]. At this level, with an ecarteur of Farrabeuf it is lifted upwards [Citation6] and the anterior arch is incised with scissors, which allows entry to the deep inguinal ring (). The procedure then continues using the steps of classic surgery.
Figure 1 Vertical incision on the median interscrotal raphe.
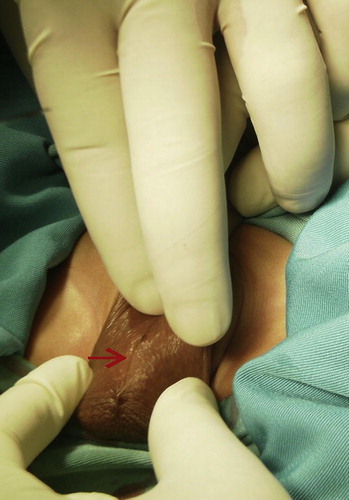
Figure 2 Exploration of the scrotum.

Figure 3 Full access to both testicles.
Results
In the 21 boys, of the 10 bilateral inguinal hernia repairs, seven were successful [Citation7], and the remaining three were unilateral recurrent hernia, either due to inadequate ligation of the hernia sac [Citation8], or a hernia sac that was too wide and friable [Citation9]. The surgeon should check that the sac has been excised at the level of the deep inguinal orifice next to the pre-hernia lipoma. Of the four bilateral ectopic testes, three were treated successfully and one had an infection of the wound [Citation10]. Of the four boys with torsion of the spermatic cord, all were treated successfully, and both the testicular biopsy and webbed penis repair were successful ().
The technique has the advantage of a single incision, much less dissection and disruption of tissue, and greater comfort for the ‘day-case’ child.
In conclusion, interscrotal access is an important approach that could eventually replace bilateral inguinal incisions, and is an option for approaches to inguinoscrotal pathologies.
Conflict of interest
None.
Source of funding
None.
Notes
Peer review under responsibility of Arab Association of Urology.
References
- A.BianchiB.R.SquireTransscrotal orchidopexy: orchidopexy revisedPediatr Surg Int41989189192
- K.R.IyerV.KumarS.N.HuddartA.BianchiThe scrotal approachPediatr Surg Int1019955860
- M.A.KoyleR.WalshA.CarusoE.WilsonScrotal (Bianchi) approach to patent processus vaginalis in childrenTech Urol519999599
- T.S.BasselH.C.ScherzA.J.KirschScrotal incision orchiopexy for undescended testes with or without a patent processus vaginalisJ Urol177200715161518
- J.K.ParsonsF.FerrerS.G.DocimoThe low scrotal approach to the ectopic or ascended testicle: prevalence of a patent processus vaginalisJ Urol169200318321833
- A.RajimwaleW.O.BrantM.A.KoyleHigh scrotal (Bianchi) single-incision orchidopexy: a ‘tailored’ approach to the palpable undescended testisPediatr Surg Int202004618622
- C.M.CalkinsS.D.St PeterA.BalcomP.J.MurphyLate abscess formation following indirect hernia repair utilizing silk suturePediatr Surg Int232007349352
- C.FearneM.AbelaD.AquilinaScrotal approach for inguinal hernia and hydrocele repair in boysEur J Pediatr Surg122002116117
- T.Y.ShihY.H.UenSingle scrotal incision for repair of bilateral inguinal hernias in boysPediatr Surg Int282012417420
- A.LaisF.FerroTrans-scrotal approach for surgical correction of cryptorchidism and congenital anomalies of the processus vaginalisEur Urol291996235238