
Abstract
Objective:
To report the first laparoscopic periprostatic implantation of an artificial urinary sphincter (AUS) after a transurethral resection of the prostate.
Background:
The implantation of an AUS is a standard procedure for severe urinary incontinence. In men it is usually implanted through a perineal approach, with the cuff placed around the bulbous urethra, bladder neck, or even around the prostate.
Method:
We report a laparoscopic periprostatic implantation of an AUS after a transurethral resection of a prostate in a 72-year-old-man with incontinence.
Results:
The operative duration was 180 min and the blood loss was 150 mL. There were no complications. After activating the AUS the patient was totally continent.
Conclusion:
The laparoscopic periprostatic implantation of an AUS is a safe, effective and considerably less invasive procedure.
Abbreviations:
Introduction
Urinary incontinence (UI) in men has been reported to have a variable overall prevalence of 5–39% and is more common in elderly men [Citation1,Citation2]. It can reduce the quality of life considerably, and cause emotional and psychosocial distress to the patient and their families. In the USA it was estimated that the financial costs of UI were >$10 billion/year [Citation3].
Although more common after radical prostatectomy, UI can also occur after TURP [Citation4], but Wasson et al. [Citation5] reported that they found no difference in the occurrence of UI between patients who were under ‘watchful waiting’ and those treated by TURP. Nevertheless, due to the increasing reduction in quality of life associated with UI, the surgical correction with an artificial urinary sphincter (AUS) has been advocated as the standard for UI caused by sphincter insufficiency [Citation6]. This is supported by studies suggesting that the AUS can produce continence rates of 73–90% in men with UI after TURP, and has a durability rate of 80% over 5 years [Citation4,Citation6–Citation8].
Traditionally, an AUS is inserted using an open procedure [Citation4]. With the increasing use of laparoscopic surgery in urology, we report our laparoscopic technique for implanting an AUS.
Case report
A 72-year-old man presented to our department in 2012 with severe UI. He had undergone a TURP 3 years before presentation due to troublesome LUTS secondary to benign prostatic enlargement. His UI was urodynamically confirmed as stress UI. Due to the irreversible intrinsic sphincter deficiency caused by the TURP, and bothersome involuntary leakage of urine which reduced his quality of life considerably, he was considered for surgical intervention. After thorough counselling the patient was keen to undergo a laparoscopic approach, knowing the high risk of conversion, as the procedure had not been attempted before.
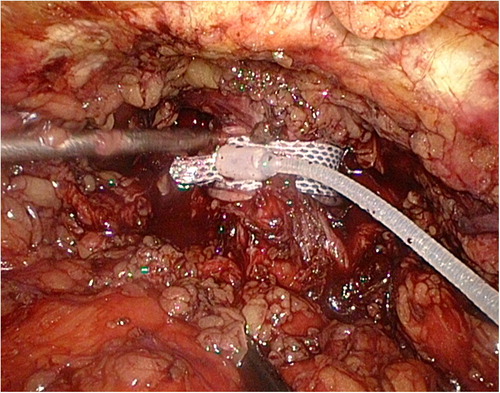
The patient was operated under general anaesthesia and placed in the Trendelenburg position. The trocar placements were similar to those for a laparoscopic radical prostatectomy. A 10-mm trocar was placed at the level of the umbilicus. Two 10-mm working trocars were inserted lateral to the rectus and just inferior to the umbilical trocar bilaterally. Two further 5-mm trocars were placed at the mid-clavicular line and medial to the anterior superior iliac spine bilaterally. The five-trocar configuration created a fan-shaped array (). Dissection was carried out from the superior part of the rectovesical pouch, then to the fascia posterior to the seminal vesicle, and down to Denonvilliers’ fascia (). After this, the endopelvic fascia was dissected bilaterally to gain access to the retropubic space. As a result, a ‘tunnel’ between the prostate and rectum is created in which a cuff with a specific length can be introduced (). The 0° laparoscope was used for most of the procedure, but a 30° laparoscope was necessary for the dissection of the prostate, for the measuring tape and the cuff. The diameter of the AUS that was required was measured using the measuring tape introduced via the right-sided 10-mm working port. The AUS (AMS 800) was subsequently implanted around the prostate (). A 5-cm lower midline incision was made to accommodate the insertion of the reservoir. All remaining parts of the AUS were placed and connected in a standard manner. The total duration of the procedure was 180 min and the estimated blood loss was 150 mL. There were no complications during or after the surgery. At 48 h after the procedure, the urinary catheter was removed and the patient was discharged from the hospital. The AUS was activated 1 month after surgery. After 1 year the patient maintained continence, with no accidental leakage reported and no malfunction problems with the device.
Figure 1 Port placement.
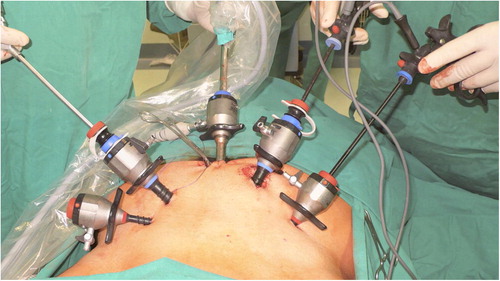
Figure 2 Start of the dissection of the rectovesical pouch.

Figure 3 A view of the ‘tunnel’.
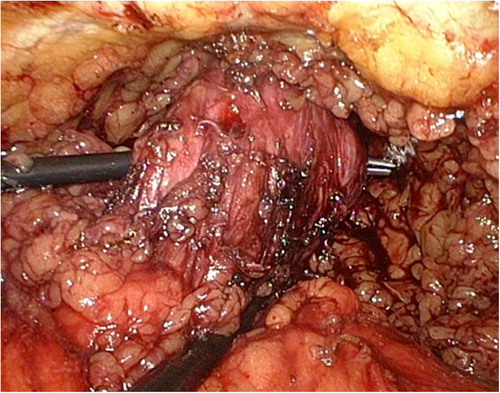
Figure 4 A laparoscopic view of the prostate with the AUS in place.
Discussion
The European Association of Urology (EAU) recommends that the treatment of choice for persistent moderate to severe UI is the implantation of an AUS [Citation9]. The implantation of an AUS laparoscopically was previously described in women [Citation10–Citation12], but as far as we are aware, our report represents the first case of laparoscopic AUS implantation after a TURP.
Roupret et al. reported the largest case series of laparoscopic AUS implantation in 12 women, achieving complete continence or a significant improvement in 11 of the patients [Citation10]. These results are comparable with that of the open approach, whereby long-term continence rates are maintained in >90% of patients [Citation13–Citation15].
Furthermore, Roupret et al. [Citation10] found that there was also an additional benefit of reduced postoperative pain with the laparoscopic approach. However, the hospital stay was not reduced. They also reported five cases of urinary retention after catheter removal, but there were no long-term consequences when the catheter was left for longer.
The laparoscopic technique has a benefit over the open procedure in that it gives better imaging and a direct view of the anatomy, which allows for a more meticulous dissection of the planes when in experienced hands. However, in patients with previous pelvic surgery or radiotherapy, these planes might become very difficult to dissect. Therefore, as most men with UI have had such surgery or therapy, the learning curve for AUS surgery might be quiet steep.
Nonetheless, unlike in the published series, the present patient was able to go home 2 days after surgery, with minimal complications, and the AUS was activated 1 month later [Citation10–Citation12]. We believe this allowed sufficient time for healing and the sling to take to its position around the prostate. After 1 year the patient remains continent with no complications.
We believe that the laparoscopic procedure can be offered to selected patients to treat UI, but only robust comparative trials can confirm the technique to be better than its open counterpart.
In conclusion, we report the first successful case of a laparoscopically implanted AUS in a man with severe UI secondary to a TURP. With a follow-up of 1 year, the patient remained fully continent with no sphincter-related complications. Nonetheless, larger series in similar patients are required to fully establish the feasibility of the laparoscopic approach. However, in the era of minimally invasive surgery we envisage that this will not take long and will soon replace the open technique as the standard.
Conflict of interest
None.
Source of funding
None.
Supplementary Data 1
Download JPEG Image (46.7 KB){kind=link}
Acknowledgements
We thank Dr. Isra Ashi for her support and advice. We obtained informed consent from the patient to write this case report, with full confidentiality of his identity provided.
Notes
Peer review under responsibility of Arab Association of Urology.
References
- A.BortolottiB.BernardiniE.ColliP.Di BenedettoG.Giocoli NacciM.Landoniet alPrevalence and risk factors for urinary incontinence in ItalyEur Urol3720003035
- R.M.BauerC.GozziW.HubnerV.W.NittiG.NovaraA.Petersonet alContemporary management of postprostatectomy incontinenceEur Urol592011985996
- D.S.ElliottD.M.BarrettMayo Clinic long-term analysis of the functional durability of the AMS 800 artificial urinary sphincter: a review of 323 casesJ Urol159199812061208
- M.HussainT.J.GreenwellS.N.VennA.R.MundyThe current role of the artificial urinary sphincter for the treatment of urinary incontinenceJ Urol1742005418424
- J.H.WassonD.J.RedaR.C.BruskewitzJ.ElinsonA.M.KellerW.G.HendersonA comparison of transurethral surgery with watchful waiting for moderate symptoms of benign prostatic hyperplasia. The Veterans Affairs Cooperative Study Group on Transurethral Resection of the ProstateNew England J Med33219957579
- C.TuygunA.ImamogluA.GucukG.GoktugF.DemirelComparison of outcomes for adjustable bulbourethral male sling and artificial urinary sphincter after previous artificial urinary sphincter erosionUrology73200913631367
- H.H.LaiE.I.HsuB.S.TehE.B.ButlerT.B.Boone13 years of experience with artificial urinary sphincter implantation at Baylor College of MedicineJ Urol177200710211025
- J.C.GundianD.M.BarrettB.G.ParulkarMayo Clinic experience with the AMS 800 artificial urinary sphincter for urinary incontinence after transurethral resection of prostate or open prostatectomyUrology411993318321
- A.SchroderP.AbramsK.-E.Anderssonet alGuidelines on urinary incontinence2010European Association of Urology
- M.RoupretV.MisraiC.VaessenV.CardotF.CourF.Richardet alLaparoscopic approach for artificial urinary sphincter implantation in women with intrinsic sphincter deficiency incontinence: a single-centre preliminary experienceEur Urol572010499504
- M.R.HodaA.Gauruder-BurmesterC.KummelT.NitzkeG.PopkenManagement of female stress urinary incontinence. Endoscopic extraperitoneal artificial urinary sphincter – early experienceDer Urologe Ausg A47200810048
- B.N.NgninkeuG.van HeugenM.di GregorioB.DebieA.EvansLaparoscopic artificial urinary sphincter in women for type III incontinence: preliminary resultsEur Urol472005793797
- P.CostaN.MottetB.RabutR.ThuretK.Ben NaoumL.WagnerThe use of an artificial urinary sphincter in women with type III incontinence and a negative Marshall testJ Urol165200111721176
- V.G.PeteroJrA.C.DioknoComparison of the long-term outcomes between incontinent men and women treated with artificial urinary sphincterJ Urol1752006605609
- K.ThomasS.N.VennA.R.MundyOutcome of the artificial urinary sphincter in female patientsJ Urol167200217201722
Appendix A
Supplementary data
Supplementary data associated with this article can be found, in the online version, at http://doi:10.1016/j.aju.2015.06.001.