
Abstract
Objective:
To describe a new technique for suprapubic urinary catheterisation that can be used in selected patients with high anaesthetic risk, and previous lower abdominal surgery and bowel adhesions.
Patient and methods:
In a 33-year-old woman, laparoscopic guidance with cystoscopic vision was used to ensure the safe passage of a suprapubic catheter.
Results:
The suprapubic catheter was successfully inserted in this challenging patient; release of adhesions allowed for the passage of the catheter without bowel injury.
Conclusion;
Laparoscopic and cystoscopic-assisted suprapubic catheter insertion is a novel technique to avoid significant morbidity and mortality in selected patients with high anaesthetic risk, and previous lower abdominal surgery and bowel adhesions.
Introduction
Long-term urinary catheterisation is usually employed for difficulty in storage with incontinence or difficulty in voiding with retention of urine. Urinary catheterisation is indicated to maintain a continuous outflow of urine for patients with voiding difficulties, as a result of neurological disorders that cause paralysis or loss of sensation affecting urination [Citation1–Citation4]. Intermittent catheterisation or an indwelling catheter can be used for long-term urinary catheterisation. The most commonly used indwelling catheters are urethral and suprapubic catheters.
Different techniques for suprapubic catheter insertion are described; including cystoscopic-guided, ultrasound-guided, open technique, and ‘blind’ technique for emergency suprapubic catheter insertion. However, suprapubic catheterisation can be technically challenging and simply contraindicated in certain cases.
In the present case report, we describe a new technique for suprapubic catheter insertion in a complicated case with previous abdominal surgeries and known abdominal adhesions associated with multiple co-morbidities.
Background
The patient was a 33-year-old woman with multiple co-morbidities. She was wheelchair bound after an emergency L5 laminectomy for cauda equina syndrome and had also had multiple cerebrovascular accidents. The patient had a permanent colostomy following a recto-sigmoid perforation 2 years before. She had bowel adhesions that were managed conservatively. Also, she was on long-term anticoagulant therapy for antiphospholipid syndrome.
Presentation
The patient had a long-term urethral catheter for 3 years secondary to cauda equina syndrome and multiple cerebrovascular accidents with poor bladder emptying. She decided to have suprapubic catheter after detailed consultation and considering alternative options.
Technical difficulty
A CT scan showed loops of the small bowel sitting on the dome of the bladder and impinging on the anterior bladder wall ( and ). The patient had multiple abdominal adhesions following her previous abdominal surgery and this was managed conservatively. After discussion with her gastrointestinal surgeon, a laparoscopic-assisted procedure was suggested as an alternative to open surgery to avoid significant morbidity and possible mortality associated with open surgery in such a high-risk patient.
Figure 1 CT showing small bowel on the dome and anterior bladder wall.
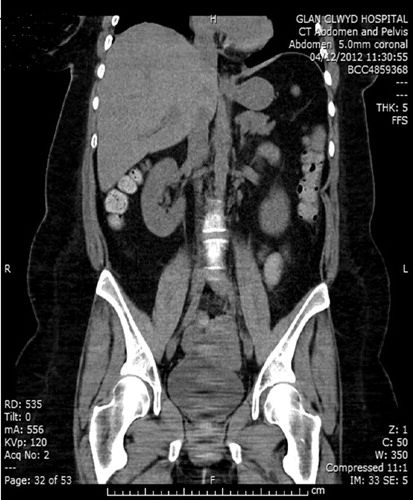
Figure 2 CT showing small bowel on the dome and anterior bladder wall.

Technical note
The procedure consisted of laparoscopic adhesiolysis and insertion of the suprapubic catheter under direct laparoscopic and cystoscopic vision.
With the patient in lithotomy position, a preliminary cystoscopy was performed to exclude bladder tumours. The open technique was used for insertion of the first laparoscopic port in the infra-umbilical region as access difficulty was encountered with bowel adhesions to the peritoneum. Pneumoperitoneum was established and the second port introduced under direct vision in the right iliac fossa.
There were severe adhesions between the bowels and peritoneum, and loops of bowel related to the anterior bladder wall. The surgeon managed to divide the adhesions on the anterior wall of the bladder allowing the bowel to move away. The suprapubic needle was inserted under direct vision, both on laparoscopy and cystoscopy, to avoid injury to the bowel and the position was confirmed in the bladder on cystoscopy. The Seldinger technique was used to insert the suprapubic catheter.
Discussion
‘Long-term’ use of a urinary catheter is defined by the National Institute for Health and Care Excellence (NICE) guidelines published in 2012 [Citation5], as a catheter being in situ for ⩾4 weeks. Long-term catheterisation may be necessary in cases of chronic retention, often as a result of neurological injury or disease, where intermittent catheterisation is not possible [Citation6]. It has beneficial effects for selected patients, which include patient comfort, family satisfaction, and nursing efficiency and effectiveness [Citation7].
In appropriate patients, the use of a suprapubic catheter, male external, or intermittent catheter is preferable to an indwelling urethral catheter [Citation8]. Suprapubic catheterisation is indicated for complications of long-term urethral catheterisation [Citation9] and also for patient’s preference due to patient needs e.g. wheelchair user [Citation1,Citation10]. There is a lower rate of infection in those with a suprapubic compared with those with urethral catheters [Citation11].
Suprapubic catheterisation is absolutely contraindicated in the absence of an easily palpable or ultrasonographically localised distended urinary bladder [Citation9,Citation10,Citation12]. It is also contraindicated in patients with previous lower abdominal surgery [Citation10] or patients with coagulopathy (until the abnormality is corrected) [Citation10,Citation12].
The most feared complication with suprapubic catheterisation is bowel perforation. Perforation of the abdominal viscera is well documented as a rare but important major complication of suprapubic cystostomy [Citation13]. The risk of bowel injury is significantly increased with previous lower abdominal surgery. Open cystostomy has been traditionally used for technically challenging suprapubic catheterisation in relation to previous abdominal surgery and bowel adhesions.
Laparoscopic and cystoscopic-assisted suprapubic catheter insertion is a novel technique to avoid significant morbidity and mortality in selected patients with high anaesthetic risk, and previous lower abdominal surgery and bowel adhesions.
Conflicts of interest
None declared.
Source of Funding
None.
Notes
Peer review under responsibility of Arab Association of Urology.
References
- D.D.CravensS.ZweigUrinary catheter managementAm Fam Physician612000369376
- K.GammackUse and management of chronic urinary catheters in long-term care: much controversy, little consensusJ Am Med Dir Assoc32002162168
- Gould CV, Umscheid CA, Agarwal RK, Kuntz G, Pegues DA; Healthcare Infection Control Practices Advisory Committee (HICPAC). Guideline for Prevention of Catheter-Associated Urinary Tract Infections 2009. Atlanta, GA: Centers for Disease Control and Prevention, 2009: p.34 and 47. Available at: <http://www.cdc.gov/hicpac/pdf/CAUTI/CAUTIguideline2009final.pdf>. Accessed August 2015.
- S.HartUrinary catheterisationNurs Stand2220084448
- National Institute for Health and Care Excellence (NICE). Infection: Prevention and control of healthcare-associated infections in primary and community care. Long-term use of urinary catheters. NICE guidelines [CG139], published date: March 2012. Available at: <http://https://www.nice.org.uk/guidance/cg139/ifp/chapter/long-term-use-of-urinary-catheters>. Accessed Augut st 2015.
- Cottenden A, Bliss DZ, Buckely B, Getliffe K, Paterson J, Pieters R., M et al. Management using continence products. In Abrams P, Carddozo L, Khoury S, Wein A eds, Incontinence. 4th edn. Paris: Health Publication Ltd, 2009: 1519-642. Available at: <http://www.icsoffice.org/Publications/ICI_4/files-book/comite-20.pdf>. Accessed August 2015.
- J.W.WarrenCatheter-associated urinary tract infectionsInfect Dis Clin North Am11987823854
- Grabe M, Bjerklund-Johansen TE, Botto H, H. Botto, Çek M, Naber KG, Pickard RS, et al. Guidelines on Urological Infections. European Association of Urology 2013. Available at: <http://uroweb.org/wp-content/uploads/18_Urological-infections_LR.pdf>. Accessed August 2015.
- Addison R, Foxley S, Mould C, Naish W, Oliver H, Sullivan J, et al. Catheter Care: RCN guidance for nurses. Royal College of Nursing. March 2008. Available at <http://www.rcn.org.uk/__data/assets/pdf_file/0018/157410/003237.pdf>. Accessed August 2015.
- Talbot K, AUNS Catheter Care SIG. Catheter Care Guidelines, 2006. The Australian and New Zealand Urological Nurses Society Inc. (ANZUNS). Available at: <http://www.anzuns.org/ANZUNS_catheterisation_document.pdf>. Accessed August 2015.
- Richard Wells Research Centre at Thames Valley University. Infection Control. Prevention of Healthcare-associated Infections in Primary and Community Care. NICE Clinical Guidelines, No. 2. National Collaborating Centre for Nursing and Supportive Care (UK). London: Thames Valley University; June 2003. Available at: <http://www.ncbi.nlm.nih.gov/books/NBK49292/>. Accessed August 2015.
- P.TenkeB.KovacsT.E.Bjerklund JohansenT.MatsumotoP.A.TambyahK.G.NaberEuropean and Asian guidelines on management and prevention of catheter-associated urinary tract infectionsInt J Antimicrob Agents31Suppl. 12008S6878
- K.L.NollerJ.H.PrattR.E.SymmondsBowel perforation with suprapubic cystostomy. Report of two casesObstet Gynecol4811976675695