
Abstract
Objective:
To assess the effect of diuretics with shockwave lithotripsy (SWL) on the treatment of renal and upper ureteric calculi.
Patients and methods:
Adult patients with a solitary non-obstructive radio-opaque renal or upper ureteric calculus with normal renal function were included. They were prospectively randomised to receive either SWL with placebo or SWL with diuretics (40 mg parenteral furosemide) in a double-blind manner with a sample size of 48 patients in each arm. The primary outcomes were the SWL success and failure rates. The secondary outcomes were the number of shocks and sessions.
Results:
Complete fragmentation was achieved in 89.6% of the patients in the furosemide arm as compared to 81.3% in the placebo arm. Clearance was achieved in 77.1% of the patients in the furosemide arm as compared to 70.8% in the placebo arm. The number of shocks and the number of sessions were higher in the placebo arm. These differences were not statistically significant.
Conclusion:
The use of diuretics along with SWL treatment of renal and upper ureteric calculi does not show a statistically significant improvement in fragmentation or clearance.
Introduction
The introduction of shockwave lithotripsy (SWL) treatment for renal and ureteric calculi in 1983 changed the treatment of smaller stones. Over time the indications and techniques have been constantly redefined in the pursuit of better outcomes. With the advent of minimally invasive surgical procedures, e.g., ureterorenoscopy (URS), percutaneous nephrolithotomy (PCNL), and retrograde intrarenal surgery (RIRS), the status of SWL has become all the more threatened. But, the unique nature of SWL, as a practically ‘no touch’ approach in the treatment of urolithiasis scores over these minimally invasive techniques [Citation1]. It is therefore imperative, that a continuous effort is made to identify novel methods that can improve the treatment outcome of SWL. One such method proposed is to provide diuresis during the shockwave session to enhance fragmentation and clearance.
Patients and methods
This hospital-based prospective randomised double-blinded placebo-controlled trial was conducted between June 2011 and December 2012. Institutional Review Board (Ethics committee) clearance was obtained as per protocol (IRB Min. No. 7386 dated 27.01.2011).
All patients aged >18 years with non-obstructive (obstruction was defined as no contrast seen beyond the calculus up to the 1 h film on IVU) radio-opaque renal and upper ureteric calculi up to 15 mm, with sterile or treated urine culture, and normal renal function (creatinine up to 1.4 mg/dL), were included after a detailed informed consent. Those with any anatomical abnormality, distal obstruction, coagulopathy, history of any previous intervention on the same side, significant cardiac history or who were morbidly obese (body mass index >40 kg/m2), were excluded.
All underwent SWL as an out-patient procedure. They were allocated by block randomisation to either SWL or SWL with diuretics (placebo or 40 mg furosemide parenteral at the start of SWL). A Dornier Compact Delta 2 electromagnetic lithotripter (Dornier MedTech GmbH, Weßling, Germany) was used. As per protocol they received shocks at 80/min starting at 7 kV with dose escalation up to 16 kV until the stone fragmented or up to a maximum of 1500/2000 shocks/session for renal and upper ureteric calculi respectively, up to a maximum of three sessions for stones up to 10 mm and four for stones 10–15 mm. Imaging was repeated at 4–14 days and sessions repeated if required (failure of fragmentation, fragments >5 mm or lead fragment >4 mm). All patients were given a minimum target fluid intake value (volume in mL = weight in kg × 50) to adhere to and followed up with frequency–volume charts.
Stratified block randomisation was carried out by the Department of Biostatistics. The patients were divided into two strata with calculi ≤10 mm and those within 11–15 mm. Sealed opaque envelopes were prepared and sent to the pharmacy for drug allocation. The drug and the placebo were packed into similar vials by the Pharmacy Department as per the code provided by the Department of Biostatistics. Thus, the patients and the investigators were totally blinded regarding the allocation.
The primary outcomes were SWL failure (no fragmentation after the designated sessions) and success rates (stone free after the allotted sessions). For renal calculi, clinically insignificant residual fragments were included as a successful outcome in calculating the success rate. However, any ureteric calculi residual fragments were considered as a failure for the calculation of success rate. The number of shocks and the number of sessions required were analysed as secondary outcomes. The target sample size with 80% power, 5% α error and −20% estimated risk difference was 48 in each arm. The difference between the two groups on the proportion of fragmentation and clearance and the 95% CIs for the difference were computed. A proportion test was used to compare the two groups on the outcomes. The mean total number of shocks and sessions between the two groups were compared using the Student’s t-test. The difference between means and the 95% CIs for the differences were evaluated. Statistical analyses were done using the Statistical Package for the Social Sciences (SPSS® version 16.0; SPSS Inc., IBM Corp., Armonk, NY, USA).
Results
Out of a total of 101 patients, five were excluded due to protocol violation or loss to follow-up. Thus, a total of 48 patients were allocated to each arm (). Both arms included 21 renal and 27 upper ureteric calculi and were evenly matched for patient and stone factors. Similarly, the site of the calculi had a similar distribution ().
Fig. 1 Consolidated Standards of Reporting Trials (CONSORT) flow diagram.
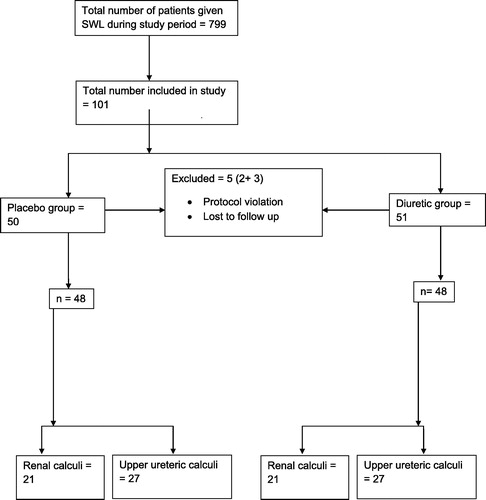
Table 1 Distribution of baseline characteristics and site of calculi.
Efficacy analyses
The percentage of complete fragmentation was 81.2% in the placebo arm and 89.5% in the furosemide arm. The mean difference in fragmentation was 8.3% (95% CI −22.3, 5.7), although higher for the furosemide arm this was not statistically significant. Similarly the mean clearance difference of 6.2% suggested more clearance for the furosemide arm with the upper limit of the 95% CI reaching up to 23%; however, this again did not reach statistical significance ().
Table 2 Primary and secondary outcomes.
The mean difference in the total number of shocks was 233 (95% CI −620, 1086). This was not statistically significant; however, it suggests that on an average the placebo arm will have 233 shocks more as compared to furosemide arm. Similarly, the total number of sessions would be 0.13 sessions more in the placebo arm as compared to furosemide arm ().
Discussion
SWL has established itself as a frontline treatment method for renal and ureteric calculi since its inception in the early 1980s. However, the constant rise in technology and the challenge offered by newer techniques, such as URS, PCNL and RIRS, highlights the need to develop novel strategies to improve its outcomes and thus for SWL to continue to play an important role as a treatment option [Citation1].
Various attempts have been made in the past to enhance the effectiveness of SWL, which have become a part of the standard treatment protocol today. These include lower shockwave rate, power ramping, percussion inversion, and diuresis for lower calyceal calculi, and medical expulsion therapy using α-blockers [Citation2–Citation6].
One such method proposed and commonly used, although never studied in a randomised trial, is to provide diuresis during the shockwave session to enhance fragmentation and clearance. Fragmentation is facilitated by a fluid film interface between the stone and the ureteric wall. Once the initial shockwaves break the outer shell of the calculus, further disintegration of the core may be enhanced by the seepage of fluid below the cracks, creating an interface. Thus, the effect of the collapsing cavitation bubble is accentuated. It is also proposed that diuretics reduce the requirement of the total number of shocks and sessions [Citation7–Citation10].
Our present results were in concordance with an earlier study by Azm and Higazy [Citation7], which reported an overall fragmentation rate of 87% for ureteric calculi in the control group vs 96.2% in the furosemide arm. Stone clearance rates were reported as 87% vs 92.3%, respectively.
A much higher difference in both stone fragmentation and clearance for ureteric calculi using 40 mg furosemide before the start of SWL was reported in another study. Fragmentation was achieved in 93.1% vs 81% in the furosemide and control groups, respectively. Clearance was reported as 88.4% vs 68.2% for the above groups [Citation8].
For lower calyceal calculi, Tahir et al. [Citation9] reported a clearance rate of 73.3% using 20 mg furosemide vs 60% in the control arm.
In a Cochrane review that included two randomised controlled trials, where diuresis was one of the interventions along with percussion and hydration with SWL for lower pole renal calculi, it was found that the stone-free rates were higher in the intervention group. It was felt that the finding was based on limited evidence as the methodological quality of both studies was moderate [Citation11].
Although our present results correspond to published data; the differences between the placebo and furosemide arm were not large enough to achieve statistical significance. As the present study is the only randomised controlled trial, the commonly used practise of diuretics along with SWL needs further study.
The sample size was determined based on the presumption that the difference between the two groups would be ∼20%. Our observations showed that the difference obtained was ∼8% for fragmentation and 6% for clearance. However, considering both outcomes as a composite outcome (that is, either fragmentation or clearance) the present study has provided a power of 71%. Moreover, the lower limit of the 95% CI for fragmentation, 22% suggested that the difference would be as high as 22% as compared to the placebo group in the long run. Similarly the difference in the outcome of clearance would be as high as 24% in the furosemide group as compared to the placebo group. Despite statistically non-significant results, these findings suggest that furosemide might be beneficial.
Conclusion
The use of diuretics with SWL in the treatment of renal and upper ureteric calculi improved fragmentation and clearance, although the difference was not statistically significant. The number of shocks and the number of sessions were also lower in the group that received diuretics.
Conflicts of interest
None.
Source of funding
None.
Notes
Peer review under responsibility of Arab Association of Urology.
References
- C.BachN.BuchholzShock wave lithotripsy for renal and ureteric stonesEur Urol Suppl102011423432
- K.MadboulyA.Moneim el-tiraifiM.SeidaS.R.El-faqihR.AtassiR.F.TalicSlow versus fast shock wave lithotripsy rate for urolithiasis: a prospective randomized studyJ Urol1732005127130
- J.E.LingemanJ.A.McAteerE.GnessinA.P.EvanShock wave lithotripsy: advances in technology and techniqueNat Rev Urol62009660670
- C.BachT.KaraolidesN.BuchholzExtracorporeal shock wave lithotripsy: what is new?Arab J Urol102012289295
- E.ChiongS.T.HweeL.M.KayS.LiangR.KamarajK.EsuvaranathanRandomized controlled study of mechanical percussion, diuresis, and inversion therapy to assist passage of lower pole renal calculi after shock wave lithotripsyUrology65200510701074
- S.K.BhagatN.K.ChackoN.S.KekreG.GopalakrishnanB.AntonisamyA.DevasiaIs there a role for tamsulosin in shock wave lithotripsy for renal and ureteral calculi?J Urol177200721852188
- T.A.AzmH.HigazyEffect of diuresis on extracorporeal shockwave lithotripsy treatment of ureteric calculiScand J Urol Nephrol362002209212
- A.ZomorrodiJ.GolivandanJ.SamadyEffect of diuretics on ureteral stone therapy with extracorporeal shockwave lithotripsySaudi J Kidney Dis Transpl192008397400
- M.M.TahirM.U.KhanS.GhauriExtracorporeal shockwave lithotripsy; impact of diuresis on the clearance of lower pole renal calculiProfessional Med J152008193199
- D.DoddamaniT.SinhaS.C.KaranG.SethiA.PrasadD.V.SinghForced diuresis during extracorporeal shockwave lithotripsy to enhance clearance: a prospective randomised controlled studyIndian J Urol242008s28s29
- L.R.LiuQ.J.LiQ.WeiZ.H.LiuY.XuPercussion, diuresis, and inversion therapy for the passage of lower pole kidney stones following shockwave lihotripsyCochrane Database Syst Rev8201312