Abstract
Objectives
Postspinal shivering is a frequent complication following spinal anesthesia. The aim of this study was to compare the effectiveness of nefopam with that of ketamine plus midazolam and placebo in the prevention of postspinal shivering.
Methods
We studied 226 patients undergoing elective orthopedic surgery. Patients were located to one of three groups, group N (n = 76) received 0.2 mg kg−1 nefopam, group K (n = 75) received ketamine 0.25 mg plus midazolam 40 μg kg−1 and group S (n = 75) received saline 0.9% as placebo.
Results
We found a significant reduction in the incidence of shivering in group N and group K in comparison to group S. There were no significant differences in hypotenion and bradycardia in all groups. Sedation was significant in group K in comparison with group N and S.
Conclusion
The results of our study showed that nefopam (0.2 mg kg−1) is as effective as ketamine 0.25 mg plus midazolam 40 μg kg−1 in the prophylaxis of postspinal shivering and not accompanied by sedation or hemodynamic side effects.
1 Introduction
Shivering frequently follows regional anesthesia. It is considered as one of the most common complications of anesthesia. Shivering is defined as an involuntary movement of one or more muscle occurring during the early phase following regional or general anesthesia [Citation1].
Postspinal shivering may lead to patient discomfort and can cause more severe complications in patients with history of cardio-respiratory diseases. These complications include increased oxygen consumption, hypoxemia, increased carbon dioxide production and lactic acidosis [Citation2], also, during shivering patients’ intracerebral and intraocular pressure increase, in addition, interference with the monitoring of ECG and blood pressure may occur [Citation3–Citation5].
Many studies have been done for the detection of drugs or methods to prevent and treat shivering, which recommended certain drugs to be used for the control of shivering, such as meperidine, ketamine plus midazolam, neostigmine and ketanserin [Citation6,Citation7].
Ketamine which is a competitive receptor antagonist of N-methyl-d-aspartic acid (NMDA) has a role in thermoregulation by different means [Citation9]. NMDA receptor acts by modulating the noradrenergic and serotoninergic neurons in the locus ceroleus. Also, NMDA receptors modulate ascending nociceptive transmission at the dorsal horn of the spinal cord [Citation10]. Ketamine controls shivering by non-shivering thermogenesis either by the action on the hypothalamus or by the B-adrenergic effect of Norepinephrine [Citation11].
Benzodiazepines have been found to reduce repetitive firing in response to depolarizing pulses in mouse spinal cord neurons [Citation12]. This function may be responsible for suppressing shivering. Among benzodiazepines, diazepam has been found to be effective in the prevention of postspinal shivering [Citation13]. It produces minimal impairment of thermoregulatory control [Citation14].
Nefopam hydrochloride is a non-sedative benzoxazocine analgesic compound (3,4,5,6-tetrahydro-5-methyl-l-phenyl-1H-2.5-benoxazocine hydrochloride), which prevents the synaptic reuptake of dopamine, nor epinephrine and serotonin in an amphetamine like fashion [Citation8]. It is a non-opioid analgesic drug that is safe and effective in preventing shivering after general and neuraxial anesthesia with little effect on the sweating and vasoconstriction thresholds [Citation15–Citation18].
In this study we shall compare the anti-shivering effect of nefopam with that of ketamine plus midazolam in comparison with placebo after spinal anesthesia, in addition to evaluating any side effect of such medications.
2 Methods
Following approval of the local ethical committee and written informed consents, we studied 226 patients (ASA physical status, I, II or III) scheduled to undergo knee arthroscopy (diagnostic and therapeutic), reduction and fixation of tibia and fibula fractures. The surgeries were done in Demerdash Surgical Hospital (orthopedic unit). Patients were randomly allocated to one of three groups:
Group N: received 0.2 mg kg−1 nefopam (n = 76).
Group K: received 0.25 mg ketamine plus 40 μg kg−1 midazolam (n = 75).
Group S: received same volume of saline 0.9% as placebo (n = 75).
Participants were allocated to the study group by a computer-generated random number assignment before the study started using sealed envelopes that were opened just before the patients entered the study. The studied drugs were diluted with normal saline 0.9% in 20 ml fixed volume and administered intravenously 5 min before spinal anesthesia using a double blind protocol. All the studied drugs were given to the patients by staff anesthesiologist, blind to the study hypothesis.
The following patients were excluded from the study:
Those with a known allergy to any study medication, patients with a fever (temperature > 37.5 °C), those with known muscle diseases, Parkinson’s disease, impaired hepatic or renal disease, patients taking MAOI or tricyclic antidepressants, those who take alpha 2 agonist or beta receptor blockers as medication, those with cardiac arrhythmias or heart failure (NYHA III or IV), those with urinary retention, glaucoma or known alcohol abuse.
All patients fasted for at least 6–8 h pre-operatively and just before the spinal anesthesia were pre-hydrated with lactated Ringer’s solution (15 ml kg−1).
Standard monitoring including continuous electrocardiogram and heart rate, pulse oximetry, non-invasive automated blood pressure measurement were recorded by anesthesia resident blind to the patient group.
After complete aseptic technique, spinal anesthesia was induced in all cases in the lateral decubitus position. Lumbar puncture was done at L 3–4, with a 22 gauge Quincke spinal needle via a midline approach after local infiltration of the area with alkalinized 1% lidocaine (0.5 ml NaHCO3 for each 10 ml lidocaine).
The cerebrospinal fluid was aspirated, and 3 ml of heavy bupivacaine (heavy marcaine, AstraZeneca®) with 25 μg fentanyl was injected through a spinal needle over a period of 15 s. The spinal needle was withdrawn and the patients were repositioned supine with slight elevation of the head (15–20°) for comfort. Patients wore a cotton gown and were draped with a single blanket. During the intra-operative period, all patients were completely covered in surgical drapes except for the head and neck area. No means of active warming were used. Ambient temperature of the operating rooms was maintained at 22–25 °C with constant humidity (a room humidity of approximately 55–65%). The sensory level was tested by pinprick sensation and the maximum level of sensory block was the highest level of disappearance of pinprick sensation reached during the study period. Systolic arterial pressure (SAP), heart rate (HR), peripheral oxygen saturation (SpO2), and sedation score (0 = alert, 1 = awake but drowsy, 2 = asleep but arousable, 3 = unarousable) were measured. All measurements were recorded at baseline and then at 5, 10, 15, 20, 25, 30, 40, 50, 60, and 90 min after spinal anesthesia. Ephedrine 5–10 mg i.v. was administered if SAP decreased less than 90 mm Hg and may be repeated if needed. HR under 50 beats/min was treated with atropine 0.5 mg i.v. Tympanic temperature was monitored every 20 min using an ear thermometer (Insta-Temp 9000; Welch Allyn, San Diego, CA). A tourniquet was placed on the thigh to minimize blood loss. Fluid resuscitation was given as follows as maintenance: first 10 kg → 4 ml/kg/H, second 10 kg → 2 ml/kg/H, then remaining body weight → 1 ml/kg/H of lactated ringer solution. As fasting: maintenance volume X fasting hours. 50% in the first hour and 50% in the second hour.
The severity of post anesthetic shivering was assessed according to a 5 point scale similar to that used by Wrench et al. [Citation19]: 0 = no shivering; 1 = one or more of the following symptoms, piloerection, peripheral vasoconstriction, peripheral cyanosis without other cause, but without visible muscular activity; 2 = visible muscular activity confined to one muscle group; 3 = visible muscular activity in more than one muscle group; 4 = gross muscular activity including the entire body. The evaluation of patients’ shivering score was carried out by an independent anesthetist unaware of patients’ grouping.
Patients in all groups were given intravenous dose of meperidine (10–25 mg) if the drug under investigation failed to prevent shivering.
Following surgery, patients were transferred to the post anesthesia care unit (PACU) with continuous monitoring of blood pressure, heart rate and oxygen saturation.
The number of patients required in each group was calculated using a power calculation based on data obtained from a previous clinical study on the incidence of post anesthetic shivering following orthopedic surgery. These data suggest that we could expect an incidence of shivering in the placebo group of at least 40% and a reduction in the incidence to about 15% with an effective anti-shivering medication. So this study was powered to detect a reduction in the incidence from 40% to 15% with α error equal 0.05. With this assumption 71 patients per group were required. That is why we included 80 patients in each of the three groups.
Demographic data, duration of surgery, anesthesia and time spent in PACU were analyzed using Student’s test, the incidence of shivering and sedation was analyzed using Fisher’s exact test or χ2-test. The ranked sum test of Raatz [Citation20] was used to analyze the severity of shivering (shivering score). All values are expressed as mean (SD) or as median (range). A p-values of <0.05 was considered significant.
3 Results
240 patients were included in this study, 14 patients were excluded either due to refusal of the patient for regional anesthesia or failure of anesthesia due to patient factor or medications. So, 226 patients were included in the study.
All groups were similar with respect to demographic data, duration of surgery and anesthesia and baseline tympanic temperatures ().
Table 1 Demographic characteristics, perioperative data and lowest vital signs.
The time to highest sensory level and maximal number of segments blocked showed no differences among the groups. Complete motor blockade of the lower extremities was observed in all patients.
In patients treated with nefopam 0.2 mg kg−l, 65 of 76 patients (85.5%) had no symptoms of shivering but 11 patients (14.5%) showed signs of piloerection peripheral vasoconstriction (shivering score grade 1). No patient in this group showed any muscular activity (shivering score grade 2–4). In the ketamine plus midazolam treated patients, 63 of 75 were symptom free (84%). 10 patients showed signs of piloerection, peripheral vasoconstriction (13%), two patients reached shivering score grade 2 (3%) and no patient reached score 3 or score 4. In the placebo group 44 of 75 patients (59%) had no symptoms of shivering but 31 patients (41%) showed signs of shivering. Nine patients showed piloerection, peripheral vasoconstriction (shivering score grade 1). 13 patients scored 2 & 3 and 9 scored 4 ().
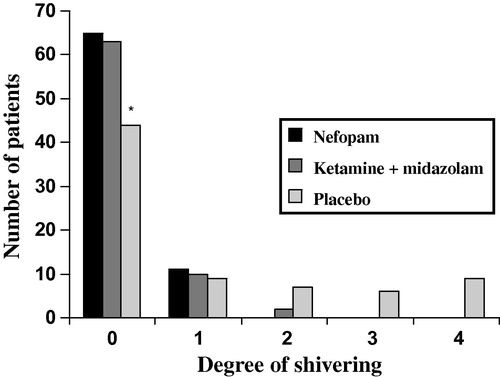
By analyzing the shivering score, we found a significant higher grading in the placebo group compared to all other groups (P < 0.01). The consumption of meperidine was significantly lower in the N and K groups compared to group S ().
Table 2 Perioperative consumption of meperidine.
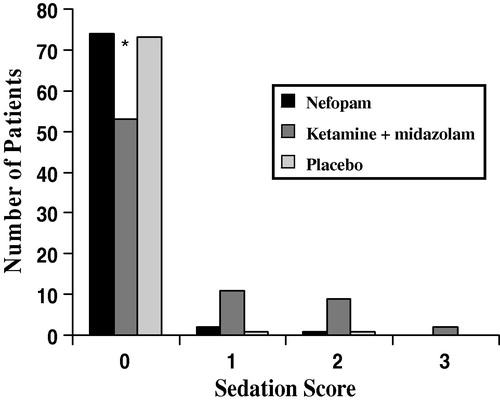
The patients in group K were more sedated than the other two groups (). SAP and HR decreased significantly after spinal anesthesia in all groups, and the lowest SAP and HR showed approximately 13–18% reduction compared with baseline values, showing no differences among the three groups (). SAP decreased to less than 90 mm Hg in seven patients in group K, six patients in group N and seven patients in group S, respectively. Three patients in group K, four patients in group N and four patients in group S had HR between 43 and 45 beats/min. Oxygen saturation exceeded 94% in all patients.
4 Discussion
Shivering associated with spinal and epidural anesthesia is a common and uncomfortable side effect. It develops in up to 60% of patients. Redistribution of heat from core to periphery, loss of thermoregulatory vasoconstriction below the level of blockade resulting in an increased heat loss from body surfaces [Citation21,Citation22], and altered thermoregulation characterized by a decrease in vasoconstriction threshold [Citation23] are considered to be the possible contributing factors to shivering.
Shivering causes patient distress and also lead to other adverse effects, including increased oxygen consumption, lactic acidosis, raised carbon dioxide production and increased left ventricular systolic work index [Citation24,Citation25]. Prevention seems essential especially in vulnerable patients and should be effective, simple, in noxious and inexpensive.
In this study we compared the efficacy of nefopam to ketamine plus midazolam and placebo for the prevention of shivering. The major finding was that nefopam 0.2 mg kg−1 significantly reduced the incidence of shivering as ketamine plus midazolam compared to placebo.
Nefopam is a non-narcotic analgesic that shares no properties with the nonsteroidal anti-inflammatory agents and, in contrast with narcotic analgesics, significant opiate receptor binding does not occur [Citation26,Citation27]. The relation between shivering and the effects of drugs on vasoconstriction means that it is possible to interpret our finding. The efficacy of the drug in the prevention of shivering is through its effect on patient shivering threshold and on the vasoconstriction threshold [Citation28]. In our study the tympanic temperature was not significantly different between all groups at any time. Alfonsi et al. [Citation29] has demonstrated that nefopam causes a small increase in the core temperature by decreasing the shivering threshold and not by modifying sweating and vasoconstriction threshold so they concluded that nefopam possesses a specific anti-shivering effect.
A gold standard for the treatment and prevention of shivering has not been defined [Citation25]. However, ketamine increases arterial pressure, heart rate and cardiac output because of direct sympathetic stimulation so it may be logical to use ketamine in patients who are at risk of hypothermia [Citation30].
Sagir and colleagues [Citation31] showed that ketamine 0.5 mg kg−1 intravenously prevents postspinal shivering but patients may develop postoperative hallucinations and nausea or vomiting. In our study, we used midazolam + ketamine so patients didn’t suffer from hallucinations postoperatively. Goold and Colleagues [Citation32] studied patients undergoing brachytherapy for cancer cervix and found that midazolam administration towards the end of anesthesia hasten the gain of core temperature and prevent shivering postoperatively and this is similar to the results in this study.
Kurz and colleagues [Citation14] found that the reduction in heat production after administration of midazolam is less than that after induction of anesthesia with clinical doses of volatile anesthetics, propofol and opioids.
Kinoshita and colleagues [Citation33] showed that infusion of a low dose ketamine prevents decrease in body temperature of patients during spinal anesthesia which is similar to the results of the present study.
Honarmand and Safayi [Citation9] found that the prophylactic use of ketamine + midazolam i.v. was more effective than ketamine i.v. or midazolam i.v. in preventing postspinal shivering.
5 Conclusion
From this study we conclude that nefopam 0.2 mg kg−1 significantly decreases the incidence of postspinal shivering as ketamine 0.25 mg plus midazolam 40 μg kg−1 in comparison to placebo. The better prophylactic anti-shivering efficacy of nefopam 0.2 mg kg−1 and the sedative effects of ketamine plus midazolam suggest that nefopam is an equal to ketamine plus midazolam for the prevention of postspinal shivering.
Further studies are needed to confirm this result.
Notes
Available online 26 January 2011
References
- P. Alfonsi The effects of meperidine and sufentanil on the shivering threshold in postoperative patients. [email protected] Anesthesiology 89 I 1998 43 48
- S.C. Yu W.D. Nogan kee S.K. Kwan Addition of meperidine to bupivacaine for spinal anesthesia for cesarean sections Br J Anaesth 88 3 2002 379 383
- A. Monso J. Riudeubas F. Barbal J.R. Laporte J.M. Arnau A randomised, double-blind, placebo-controlled trial comparing pethidine to metamizol for treatment of postanaesthetic shivering Br J Clin Pharmacol 42 1996 307 311
- A.W.A. Crossley Peri-operative shivering Anaesthesia 47 1992 193 195
- G. Rosa G. Pinto P. Orsi Control of postanesthetic shivering with nefopam hydrochloride in mildly hypothermic patients at neurosurgery Acta Anaesthesiol Scand 39 1995 90 95
- Y. Zhang K.C. Wong Anesthesia and postoperative shivering: its etiology, treatment and prevention Acta Anesthesiologica Scand 37 1999 115 120
- J. De Witte D.L. Sessler Perioperative shivering: physiology and pharmacology Anesthesiology 9C 2002 467 484
- J.L. Rosland K. Hole The effect of nefopam on the uptake of 5-hydroxy tryptamine, nor-adrenaline and dopamine in crude rate brain preparations J Pharm Pharmacol 42 1990 437 438
- A. Honarmand M.R. Safayi Comparison of prophylactic use of midazolam, ketamine and ketamine plus midazolam for prevention of shivering during regional anesthesia: a randomized double-blind placebo controlled trial Br J Anaesth 101 4 2008 557 562
- D. Dal A. Kose M. Honca B. Akinci E. Basgul U. Aypar Efficacy of prophylactic ketamine in preventing postoperative shivering Br J Anaesth 95 2005 189 192
- D.R. Sharma J.R. Thakur Ketamine and shivering Anaesthesia 45 1990 252 253
- R.D. Adam M. Victor A.H. Ropper Motor paralysis R.D. Adam M. Victor A.H. Ropper Principles of neurology 6th ed. 1997 McGraw Hill, Inc. New York 45 63
- D.A. Hopkin Postoperative spasticity and shivering Anaesthesia 39 1984 725 726
- A. Kurz D.I. Sessler R. Annadata M. Dechert R. Christensen A.R. Bjorksten Midazolam minimally impairs thermoregulatory control Anesth Analg 81 1995 393 398
- J.E. Goold Postoperative spasticity and shivering Anaesthesia 39 1984 35 38
- D.I. Sessler J. Ponte Shivering during epidural anesthesia Anesthesiology 72 1990 816 821
- J.A. Kaplan A.V. Guffin Shivering and changes in mixed venous oxygen saturation after cardiac surgery Anesth Analg 64 1985 235
- 1. Vanderstappen E. Vandermeersch B. Vanacker M. Mattheussen P. Herijgers H. Van Aken The effect of prophylactic ketamine plus midazolam on postoperative shivering Anaesthesia 51 1996 351 355
- I.J. Wrench G. Cavill J.E. Ward A.W. Crossley Comparison between alfentanil, pethidine and placebo in the treatment of postoperative shivering Br J Anaesth 79 1997 541 542
- U.Die. Raatz Modification des white – Tests bei groberen stichproben Biometrische Zeitochrift 8 1996 42 54
- T. Matsukawa D.I. Sessler R. Christensen M. Ozaki M. Schroeder Heat flow and distribution during epidural anesthesia Anesthesiology 83 1995 961 967
- A. Kurz D.I. Sessler M. Schroeder M. Kurz Thermoregulatory response thresholds during spinal anesthesia Anesth Analg 77 1993 721 726
- M. Ozaki A. Kurz D.I. Sessler R. Lenhardt M. Schroeder A. Moayeri Thermoregulatory thresholds during epidural and spinal anesthesia Anesthesiology 81 1994 282 288
- S.C. Yu Intrathecal meperidine and shivering in obstetric anesthesia response Anesth Analg 99 2004 1272 1273
- P. Kranke N. Roewer M.R. Tramer Pharmacological treatment of post operative shivering Anesth Analg 94 2002 453 460
- P.I. Pillans D.J. Woods Adverse reactions associated with nefopam New Zealand Med J 108 1995 832
- M. Convvay S. Lipton A comparison of a new analgesic nefopam hydrochloride, with morphine sulphate, pentazocine and pethidine hydrochloride in post-operative pain Curr Med Res Opin 7 1982 580 597
- F. Bilotta R. Sanita C. Rosa Nefopam and tramadol for the prevention of shivering during neuroaxial anesthesia Reg Anesth Pain Med 27 2002 380 384
- P. Alfonsi F. Adam D.I. Sessler Nefopam inhibits thermoregulation and possesses a specific anti shivering effect Anesthesiology 96A 2002 257
- T. Ikeda T. Kazama D.I. Sessler Induction of anesthesia with ketamine reduces the magnitude of redistribution hypothermia Anesth Analg 93 2001 934 938
- O. Sagir N. Gulhas H. Toprak A. Yucel Z. Begec O. Ersoy Control of shivering during regional anaesthesia: prophylactic ketamine and granisetron Acta Anaesthesiol Scand 51 2007 44 49
- J.E. Goold Postoperative spasticity and shivering. A review with personal observations of 500 patients Anaesthesia 39 1984 35 38
- T. Kinoshita M. Suzuki Y. Shimada R. Ogawa Effect of low-dose ketamine on redistribution hypothermia during spinal anesthesia sedated by propofol J Nippon Med Sch 71 2004 92 98