
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background
Dexmedetomidine is an α-2 adrenoceptor agonist with sedative and analgesic properties. Desflurane is the most rapidly washed volatile anesthetic agent allowing rapid recovery with minimal metabolism. Having a MAC of 6 vol % made it important to look for an adjuvant that would minimize its consumption. This study was undertaken to analyze desflurane consumption when combined with dexmedetomidine infusion guided by bispectral index as well as calculating intraoperative fentanyl requirements and recording hemodynamic changes associated with this technique.
Methods
Forty adult patients ASA class I and II of either sex scheduled for elective laparoscopic cholecystectomy were included in this study. Patients were randomized to one of two groups: Group ‘D’ (Dexmedetomidine group) receiving 1μg/kg over 10 minutes followed by an infusion at 0.5 μg/kg/hr and Group ‘P’ (Placebo group) who received same volumes of normal saline. Desflurane was started at a concentration of 6% then adjusted to keep BIS level within the range of 40-50. Desflurane consumption, fentanyl requirements as well as hemodynamics were either calculated or recorded.
Results
Desflurane consumption and total fentanyl usage were significantly lower in group D versus group P with P value < 0.001. As regards hemodynamics, group D showed statistically significant lower readings versus the preoperative levels (P<0.05) as well as versus group P at the same timings (P<0.05) for most of the readings.
Conclusions
Continuous intravenous administration of dexmedetomidine resulted in significant reduction of desflurane consumption and intraoperative fentanyl requirements with attenuation of hemodynamic response to intubation, pneumoperitoneum and extubation.
1 Introduction
Dexmedetomidine is an active pharmacological d-isomer of medetomidine. It is a potent selective agonist of α2 adrenoceptor compared to clonidine and having sedative, amnestic, sympatholytic and pain-relieving properties [Citation1,Citation2]. Thus it can be used in relatively high doses for sedation and analgesia without hemodynamic derangements [Citation3].
Desflurane exhibits very low solubility in water with a corresponding low blood/gas partition coefficient. It is the most rapidly washed volatile anesthetic agent allowing rapid recovery with more flexibility in controlling the anesthetic depth. It undergoes minimal metabolism (0.02%) and is eliminated via the lungs [Citation4]. Having a MAC of 6 vol.%, adding an adjuvant is beneficial to minimize its consumption and reduce adverse effects.
Laparoscopic cholecystectomy is considered as the “gold standard” treatment of cholelithiasis. Carbon dioxide (CO2) is the gas of choice to produce pneumoperitoneum (PP) during laparoscopic surgical procedures [Citation5]. Hypercapnia and PP lead to stimulation of the sympathetic nervous system, with release of catecholamine and vasopressin [Citation6], leading to alteration in acid-base balance as well as cardiovascular and pulmonary physiology. These cardiovascular changes lead to decrease in cardiac output which is further aggravated by the reverse Trendelenburg position during laparoscopic surgery. The hemodynamic derangement compromises tissue perfusion, increases mean arterial pressure and predisposes to myocardial ischemia in susceptible patients [Citation7]. Hence, α2 adrenergic receptor agonist can be a good choice for prevention of hemodynamic responses associated with laparoscopic surgery [Citation8].
Previous studies reported the usage of dexmedetomidine with sevoflurane, isoflurane and total propofol intravenous anesthesia [Citation9–Citation13] but no researches were performed to calculate desflurane consumption on using dexmedetomidine adjuvant in laparoscopic cholecystectomy.
Thus we hypothesized that the use of dexmedetomidine infusion can decrease desflurane consumption and preserve hemodynamic stability during laparoscopic cholecystectomy. The primary outcome of the present study was to calculate desflurane consumption when combined with dexmedetomidine infusion guided by bispectral index (BIS). Secondary objectives were calculating intraoperative fentanyl requirements and monitoring intraoperative hemodynamic changes.
2 Patients and methods
This randomized prospective double blind controlled study was performed at Theodor Bilharz Research Institute (TBRI) in the period from 07/2016 till 11/2016, after obtaining the institutional board ethics committee approval and patient informed written consent. The study was registered in a public trial register (http://www.clinicaltrials.gov) under the identification number: http://ctgov:NCT02652312. Forty patients aged from 15 to 60 years American Society of Anesthesiologists status I and II of either sex enlisted for elective laparoscopic cholecystectomy were recruited in the study. Patients with cardiovascular, neurological, psychiatric disorder and hypertension were excluded.
Randomization was performed using computer generated random numbers that patients were alienated to one of two groups: Group ‘D’ (Dexmedetomidine group) and Group ‘P’ (Placebo group). Intravenous 0.15 mg/kg ondansetron was administered as a pre-medication. Fluid regimen consisted of Ringer's acetate solution was given at a rate of 6–8 ml/kg/h infusion throughout the procedure.
Monitoring was achieved by continuous electrokardiogram (EKG), pulse oximetry (SpO2), non-invasive blood pressure (NIBP), end tidal CO2 (ETCO2), desflurane inspired fraction (FIdes), and desflurane expired fraction (ETdes) (Infinity Kappa, Dräger, Lübeck, Germany) as well as BIS for detection of consciousness level (Infinity® BISx™ Smart Pod®, VF5).
All patients received 3 L/min oxygen using a nasal cannula as preoxygenation. Group D, patients received IV dexmedetomidine in a dose of 1 μg/kg over 10 min using a syringe pump prior to anesthetic induction (2 ml; 200 µg dexmedetomidine diluted with saline in 20 ml syringe) so the patient was given 0.1 ml/kg while group P, patients received similar volume of normal saline over 10 min. Both study drug and placebo infusions were set by an anesthetist not involved in the study.
Anesthetic induction was obtained via I.V. fentanyl 1.5 μg/kg followed by propofol titration (10 mg every five seconds) until BIS value decreased to 60 and confirmed with loss of verbal response. Then, atracurium 0.5 mg/kg IV was injected slowly followed by tracheal intubation. Fresh gas flow was started at a rate of 3 L/min mixture of 30–40% O2/air for 10 min then decreased to 1 L/min through closed system while ventilation was controlled to keep ETCO2 at 30–35 mmHg.
Patients in both groups received desflurane at a concentration of 6% which was then adjusted to keep BIS level within the range of 40–50. A maintenance dose of dexmedetomidine 0.5 μg/kg/h (0.05 ml/kg/h) was infused to group D while Group P received a similar volume of normal saline. Fifteen to twenty minutes before the end of the procedure, the infusion was stopped. A top up dose of atracurium 0.1 mg/kg was repeated every thirty minutes to maintain the neuromuscular block. Any rise in heart rate (HR) and mean arterial blood pressure (MABP) exceeding 20% of the preoperative level in spite of adequate anesthetic level guided by BIS was treated with fentanyl 0.5 μg/kg while any decrease of MABP or HR exceeding 20% was treated by IV ephedrine 5 mg or atropine 0.5 mg respectively. At the end of the procedure, desflurane was discontinued and diclofenac sodium 1 mg/kg was given IM. Neostigmine 0.05 mg/kg and atropine 0.02 mg/kg were given to reverse residual neuromuscular blockade which was followed by extubation and transfer to the recovery room.
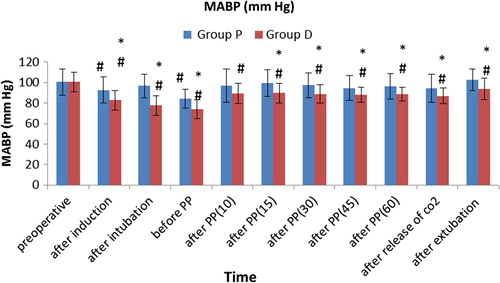
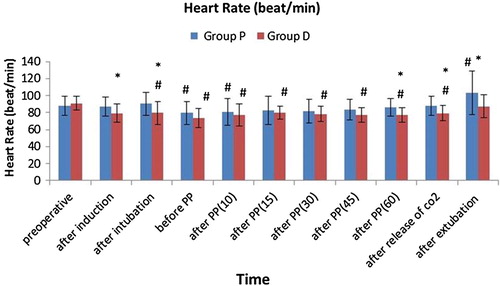
The following parameters were studied: demographic data as age, height, weight, body mass index, gender and ASA classification a well as duration of surgery and anesthesia. HR and MABP values were documented before and after induction, after intubation, before pneumoperitoneum (before pp), 5 min (after pp 5), 10 min (after pp 10), 15 min (after pp 15), 30 min (after PP 30), 45 min (after pp 45), 60 min after pneumoperitoneum (after pp 60), after release of CO2 and after extubation. Total intraoperative fentanyl requirement was also recorded. The calculation of desflurane consumption was done as follows [Citation14]:
Duration of volatile anesthesia was detected from starting time of ET control (t = 0) till the end of procedure as the vaporizer was switched off (t = end).
A conversion factor is the resultant of the amount of vapor derived from every ml volatile anesthetic fluid: 209 for desflurane, obtained as follows [Citation15]:
A total volatile anesthetic fluid used was calculated by adding the multiplying product of usage rate by the period of each instance.
3 Statistical analysis
As no previous study up the time of registering this work was available to evaluate the anesthetic consumption of desflurane co-administered with dexmedetomidine to calculate sample size, we considered this research as a pilot study and 20 patients in each group was suitable.
Data were analyzed via the statistical enclose SPSS version 22. Data were presented using mean and standard deviation in quantitative data and using frequency (count) and relative frequency (percentage) for categorical data. Unpaired t-test was used to compare between groups [Citation16]. For comparison of serial measurements within each group, ANOVA repeated measures were done with simple contrast used to assess significant difference between preoperative value and each other value measured at different times [Citation17]. Chi square (χ2) test was done to compare categorical data. When expected frequency is <5, exact test was performed instead [Citation18]. Result was considered statistically significant when P-value was less than 0.05.
4 Results
Concerning age, height, weight, BMI, ASA status, sex prevalence as well as the surgical and anesthetic duration, they were comparable in both groups ().
Table 1 Demographic data and surgical & anesthetic time.
The average consumption of desflurane and intra operative fentanyl were significantly less in group D versus group P with P value <0.001 ().
Table 2 Intraoperative consumption of desflurane and fentanyl.
In placebo group, MABP values were significantly decreased after induction of anesthesia and before pneumoperitoneum (PP) while in dexmedetomidine group, all MABP readings throughout the procedure were lower versus the preoperative reading (P < 0.05) being significantly lower in dexmedetomidine group versus placebo group (P < 0.05) at all timings except 10 min after PP ().
As regards HR, placebo group showed significantly lower values before PP and 10 min after PP but was higher after extubation while in dexmedetomidine group, they were significantly lower throughout the procedure versus the preoperative value (P < 0.05), except after extubation. The reductions were significantly greater in group D versus group P after induction, after intubation, and one hour after PP up to after extubation (P < 0.05) (). Only one patient out of 20 (5%) in group D had bradycardia that necessitated intravenous administration of 0.5 mg atropine.
5 Discussion
The current study estimated the impact of dexmedetomidine infusion on consumption of desflurane and intraoperative fentanyl as well as hemodynamics during laparoscopic cholecystectomy.
This study revealed that the average consumption of desflurane was significantly lower by 27% being 16.47 ml/h in group D compared to 22.47 ml/h in group P. Similar results were obtained by Harsoor et al. [Citation10] who found 28% reduction in the mean hourly sevoflurane requirement when using dexmedetomidine as an adjuvant with entropy-guided general anesthesia during abdominal surgery. This similarity could be due to applying the same regimen of dexmedetomidine bolus and infusion rate despite different inhalational anesthetic agent. Also Kim et al. [Citation19] found significant reduction of end tidal sevoflurane by 23.8–67% when using dexmedetomidine in children undergoing ambulatory surgery. The discrepancy in reduction values from the current study may be attributed to different age group, type of surgery as well as supplemental caudal block.
Other studies showed that continuous intra-operative infusion of dexmedetomidine decreased isoflurane requirements by 32–90% in healthy patients [Citation20,Citation21]. This wide range of reduction compared to the present study may be due to different anesthetic agent, type of surgery or variable drug regimens.
In this study, intraoperative fentanyl consumption was significantly lowered by 23% in dexmedetomidine group as compared to placebo group. Scheinin et al. [Citation22] found that dexmedetomidine combined with 70% N2O/O2 and additional enflurane produced 31% reduction of intraoperative fentanyl requirements during various surgical procedures. Vora et al. [Citation21] reported fewer patients (1%) needed intra-operative fentanyl on using dexmedetomidine combined with isoflurane versus placebo group (31%).
Tufanogullari et al. [Citation23] evaluated different IV infusions of dexmedetomidine 0.2, 0.4 or 0.8 µg/kg/h IV during laparoscopic bariatric surgery. They concluded that fentanyl requirement in the post anesthesia care unit (PACU) was reduced by 36–42%versus the placebo group. Their study was unlike ours being conducted on morbidly obese patients with different pharmacokinetic effects on drugs, ASA physical status II and III, dissimilar regimen of dexmedetomidine infusion rate as well as they calculated fentanyl consumption on admission to PACU.
El Tahan et al. [Citation24] studied dexmedetomidine effects on hemodynamic response in parturients scheduled for elective caesarean delivery. They used varying infusion doses of dexmedetomidine (0.2, 0.4 or 0.6 μg/kg/h) or placebo infusion 20 min before induction of anesthesia. They reported minimal increases in heart rate compared to placebo after anesthetic induction. However, higher doses of dexmedetomidine (0.4 and 0.6 μg/kg/h) resulted in slower heart rates and lower mean arterial pressures which matched with the results of the present study. In addition, Vora et al. [Citation21] noted significant lowering of MABP and HR with dexmedetomidine when compared to control group in patients undergoing elective laparoscopic surgeries. Moreover, an exaggerated effect of dexmedetomidine on heart rate (episode of bradycardia) occurred in three patients with the need of rescue drug administration. In this study, hemodynamic parameters were within clinically acceptable range except one patient had bradycardia that necessitated intravenous atropine administration. This bradycardia may be referred to the effect of dexmedetomidine on the ventrolateral medulla via α2-adrenoceptors, imidazoline receptors, or both of them [Citation25].
The results of Lawrence and De Lange [Citation11] study agreed with this study in the attenuation of hemodynamic response to both intubation and extubation on using dexmedetomidine. They used a single dose of dexmedetomidine 2 μg/kg given over five minutes before induction of anesthesia. They observed bradycardia after 1 and 5 min, which may be due to rapid administration of high bolus dose since cardiovascular side effects correlate to both the dosage and speed of drug administration. Song et al. [Citation26] studied the effect of various infusion rates of dexmedetomidine 0.25, 0.5, 1 μg/kg, or saline infused intravenously in pediatric patients undergoing elective strabismus and found that the mean systolic pressure was not significantly different among groups. The highest dose of dexmedetomidine showed significantly lower HR readings than the control group after PACU arrival but not to the extent of requiring medication.
Ghodki et al. [Citation27] results were more or less similar to the present study as they used 1 μg/kg dexmedetomidine intravenously over 15 min before induction of general anesthesia in laparoscopic cholecystectomy and continued by infusion of 0.2 μg/kg/h and reported attenuation in vasopressor response during laryngoscopy with minimal changes in blood pressure after pneumoperitoneum.
Limitation of this study is the small sample size as it is considered as a pilot study so larger number may be required to verify such results.
6 Conclusion
This study concluded that intravenous administration of dexmedetomidine in a dose of 1 μg/kg over 10 min before induction of anesthesia followed by intraoperative infusion of 0.5 μg/kg/h resulted in statistically significant reduction of desflurane consumption and intraoperative fentanyl requirements as well as attenuation of hemodynamic response to intubation, pneumoperitoneum and extubation.
Further study on larger scale is required to prove the advantage of this combination and also revise its financial benefit.
Conflict of interest
The authors declare that there is no conflict of interest.
Fund
Internal Project of Anesthesia Department, Theodor Bilharz Research Institute, Egypt. Project number 110.
Notes
Peer review under responsibility of Egyptian Society of Anesthesiologists.
References
- D.S.CarolloB.D.NossamanU.RamadhyaniDexmedetomidine: a review of clinical applicationsCurr Opin Anaesthesiol212008457461
- R.M.VennC.J.BradshawR.SpencerD.BrealeyE.CaudwellC.NaughtonPreliminary UK experience of dexmedetomidine, a novel agent for postoperative sedation in the intensive care unitAnaesthesia5412199911361142
- R.GertleC.BrownD.MitchellE.N.SilviusDexmedetomidine: a novel sedative-analgesic agentProc (Bayl Univ Med Cent)14120011321
- Wenker O. Review of currently used inhalation anesthetics; Part I. Int J Anesthesiol 1999;3(2). http://www.ispub.com/journals/IJA/Vol3N2/inhal1.htm.
- M.BlobnerA.R.FelberS.GoglerJ.S.EsselbornCarbon-dioxide uptake from the pneumoperitoneum during laparoscopic cholecystectomyAnesthesiology771992A37
- E.O’LearyK.HubbardW.TormeyA.J.CunninghamLaparoscopic cholecystectomy: haemodynamic and neuroendocrine responses after pneumoperitoneum and changes in positionBr J Aaesth761996640644
- S.WilcoxL.D.VandamAlas, poor trendelenburg and his position! A critique of its uses and effectivenessAnesth Analg671988574578
- S.ChiruvellaB.DonthuJ.V.SivaS.D.BabuControlled hypotensive anaesthesia with dexmedetomidine for functional endoscopic sinus surgery: a prospective randomized double blind studyJ Evol Med Dental Sci3201495569563
- A.G.BoteroL.RodríguezF.A.PérezA.V.SaavedraUse of dexmedetomidine in total intravenous anesthesia (TIVA)Rev Colomb Anestesiol392012514526
- S.S.HarsoorD.D.RaniS.LathashreeS.S.NethraK.SudheeshEffect of intraoperative dexmedetomidine infusion on sevoflurane requirement and blood glucose levels during entropy-guided general anesthesiaJ Anaesthesiol Clin Pharmacol3020142530
- C.J.LawrenceS.De LangeEffects of a single preoperative dexmedetomidine dose on isoflurane requirements and peri-operative haemodynamic stabilityAnaesthesia521997736744
- M.YildizA.TavlanS.TuncerR.ReisliA.YosunkayaS.OtelciogluEffect of dexmedetomidine on haemodynamic responses to laryngoscopy and intubation: perioperative haemodynamics and anaesthetic requirementsDrugs R D720064352
- C.DholakiaG.BeversteinM.GarrenC.NemergutJ.BoncykJ.C.GouldThe impact of perioperative dexmedetomidine infusion on postoperative narcotic use and duration of stay after laparoscopic bariatric surgeryJ Gastrointest Surg11200715561559
- S.SingaraveluP.BarclayAutomated control of end-tidal inhalation anaesthetic concentration using the GE Aisys Care stationBr J Anaesth11042013561566
- M.J.LasterZ.FangE.I.EgerSpecific gravities of desflurane, enflurane, halothane, isoflurane, and sevofluraneAnesth Analg78199411521153
- Y.H.ChanBiostatistics 102: quantitative data – parametric & non-parametric testsSingapore Med J4482003391396
- Y.H.ChanBiostatistics 301: repeated measurement analysisSingapore Med J4582004354368
- Y.H.ChanBiostatistics 103: qualitative data –tests of independenceSingapore Med J44102003498503
- N.Y.KimS.Y.KimH.J.YoonH.K.KilEffect of dexmedetomidine on sevoflurane requirements and emergence agitation in children undergoing ambulatory surgeryYonsei Med J5512014209215
- V.M.KeniyaS.LadiR.NaphadeDexmedetomidine attenuates sympathoadrenal response to tracheal intubation and reduces perioperative anaesthetic requirementIndian J Anaesth5542011352357
- K.S.VoraU.BarandaV.R.ShahM.ModiG.P.ParikhB.P.ButalaThe effects of dexmedetomidine on attenuation of hemodynamic changes and there effects as adjuvant in anesthesia during laparoscopic surgeriesSaudi J Anaesth942015386392
- H.ScheininM.L.JaakolaS.SjövallT.Ali-MelkkiläS.KaukinenJ.TurunenIntramuscular dexmedetomidine as premedication for general anesthesia. A comparative multicenter studyAnesthesiology786199310651075
- B.TufanogullariP.F.WhiteM.P.PeixotoD.KianpourT.LacourJ.GriffinDexmedetomidine infusion during laparoscopic bariatric surgery: the effect on recovery outcome variablesAnesth Analg1066200817411748
- M.R.El-TahanH.A.MowafiI.H.Al SheikhA.M.KhidrR.A.Al-JuhaimanEfficacy of dexmedetomidine in suppressing cardiovascular and hormonal responses to general anaesthesia for caesarean delivery: a dose–response studyInt J Obstet Anesth2132012222229
- Z.P.KhanC.N.FergusonR.M.JonesΑ-2 and imidazoline receptor agonists: their pharmacology and therapeutic roleAnaesthesia541999146165
- I.A.SongK.S.SeoA.Y.OhJ.S.BaikJ.H.KimJ.W.HwangDexmedetomidine injection during strabismus surgery reduces emergence agitation without increasing the oculocardiac reflex in children: a randomized controlled trialPLoS ONE1192016e016278510.1371/journal.pone.0162785
- P.S.GhodkiS.K.ThombreS.P.SardesaiK.D.HarnagleDexmedetomidine as an anesthetic adjuvant in laparoscopic surgery: an observational study using entropy monitoringJ Anaesthesiol Clin Pharmacol2832012334338