
Abstract
Primary testicular diffuse large-B cell lymphoma (DLBCL) is an uncommon and aggressive disease with predominant manifestation in the older age. Herein, we report a case of 47-year-old male patient who presented with three months history of left testis swelling. The patient underwent unilateral (left) radical orchiectomy. Histopathological examination revealed extensive involvement and replacement of testicular parenchyma by a tumor composed of large discohesive sheets of cells with pleomorphic, hyperchromatic nuclei and prominent nucleoli. Immunohistochemical (IHC) staining showed reactivity for LCA & Pan B (CD20) and negativity for OCT 3/4, SALL4 and Inhibin. Moreover, Pan T (CD3) highlighted reactive T-cells. These features rendered the diagnosis of DLBCL of testis. The hybrid 2-[fluorine-18] fluoro-2-deoxy-d-glucose (FDG) positron emission tomography/computed tomography (PET/CT) demonstrated two para-aortic FDG avid lymph nodes on the left side at the level of L2 vertebra. Presently, the patient has been planned for doxorubicin-based chemotherapy (i.e., cyclophosphamide, doxorubicin, vincristine and prednisone; CHOP) along with intrathecal Methroxate (MTX), which would presumably improve the prognosis. Our study would expand the pool of this uncommon tumor towards its better understanding.
1 Introduction
Primary testicular lymphoma (PTL) is a group of uncommon neoplasms, with the subtypes of diffuse large B-cell lymphoma (DLBCL), follicular lymphoma and Burkitt's lymphoma [Citation1,Citation2] . In general, primary testicular DLBCL, the frequent subtype among all, arises in old age (i.e., >60 years) [Citation3Citation[4]–Citation5] . The typical clinical signs of testicular DLBCL include testicular swelling, B-symptoms and elevated lactate dehydrogenase (LDH) levels [Citation6]. In general, testicular DLBCL tumors are classified based on Cotswold modification of Ann Arbor staging system, where crucial disease parameters like tumor size, lymphadenopathy and regions of lymph node involvement are considered towards the assessment of overall clinical stage of the disease [Citation7]. Primary testicular DLBCL has been reported to exhibit aggressive clinical behavior, poor prognosis and high tendency to disseminate to the central nervous system (CNS) and thereby related to high morbidity and mortality rates [Citation3,Citation8] . The hybrid 2-[fluorine-18] fluoro-2-deoxy-d-glucose (FDG) positron emission tomography/ computed tomography (PET/CT) has become the standard imaging tool for initial staging and assessment of the treatment response in lymphoma patients [Citation9Citation[10]Citation[11]–Citation12] .
Herein, we present a case of 47 year old male diagnosed with primary testicular DLBCL. Specifically, the patient and underwent unilateral (left) radical orchiectomy for both diagnostic and therapeutic purposes. PET/CT was performed for the assessment of disease extension. Our study would expand the pool of this uncommon tumor towards its better understanding.
2 Case report
A 47 years old male presented with three month history of left testicular swelling. No B-symptoms were present. The patients underwent unilateral (left) orchiectomy. Histopathology revealed extensive involvement and replacement of testicular parenchyma by a tumor composed of large discohesive sheets of cells with pleomorphic, hyperchromatic nuclei and prominent nucleoli. Necrotic foci were also identified. Immunohistochemical (IHC) staining showed the following reactivity pattern in tumor cells: positivity for LCA & Pan B (CD20) and negativity for OCT 3/4, SALL4 and Inhibin. Moreover, Pan T (CD3) highlighted reactive T-cells. All these features rendered the diagnosis of DLBCL according to WHO classification of lymphoid neoplasms (see and ).
Fig. 1 Illustrative histopathology and IHC images of the resected testicular tumor. Extensive involvement and replacement of testicular parenchyma by a tumor composed of large discohesive sheets of cells with pleomorphic, hyperchromatic nuclei and prominent nucleoli at low (10×) (A) and high (40×) (B) magnification power, and (C) Pan B (CD20) immunostain positive reactivity (10×).
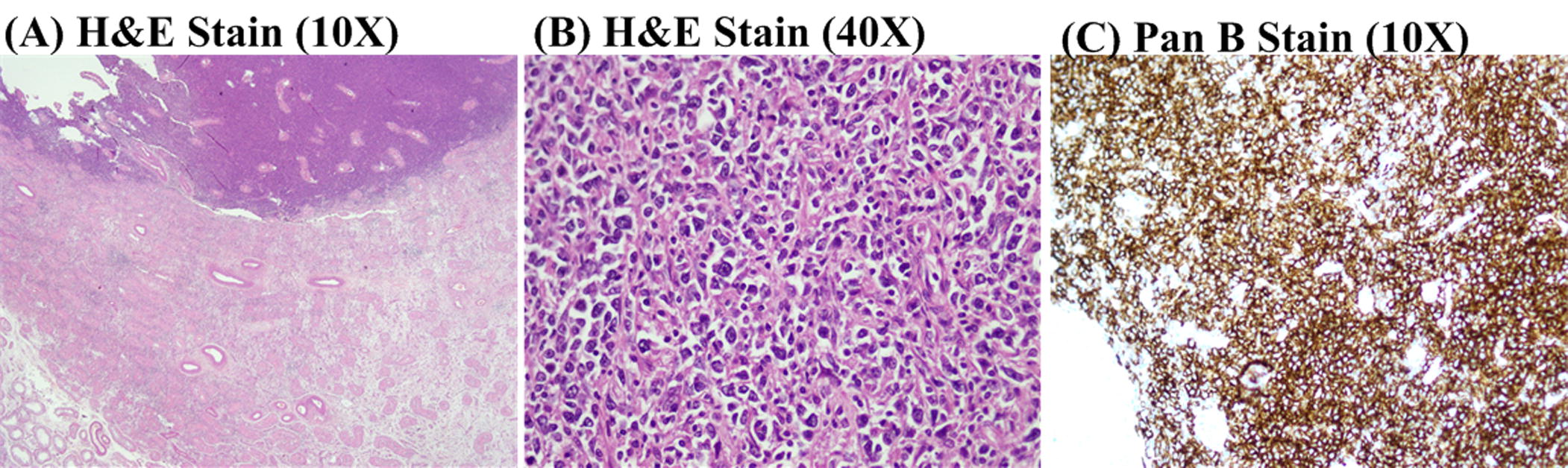
Table 1 Summary of clinical features of the patient with primary testicular DLBCL, tumor characteristics and status of immunochemical staining.
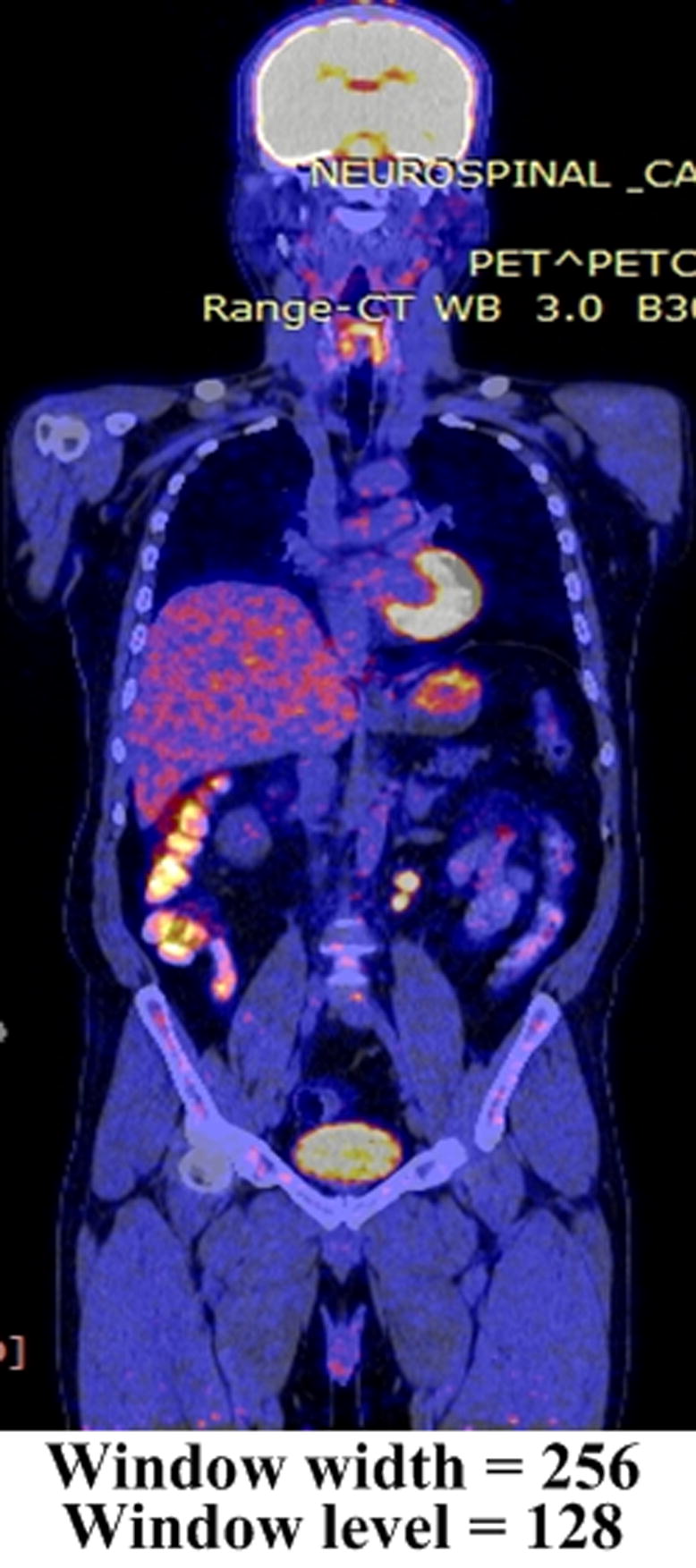
To accurately assess the disease extension and evaluate the stage, FDG PET/CT was performed which demonstrated two para-aortic FDG avid lymph nodes on the left side at the level of L2 vertebra, as shown in . The range of maximum standardized uptake value (SUVmax) was up to 9.79 and size of 1.1 × 1.5 cm along the left external iliac vessel. FDG avid lymph nodes were also seen with SUVmax ranges up to 5.65 and subcentimeter in size. Faint FDG uptake was seen along the surgical tract, possibly because of post-surgical changes. Soft tissue density lesion was seen in the upper part of the scrotal sac with SUV ranging up to 5.98 and subcentimeter in size.
Fig. 2 Illustrative FDG PET/CT image demonstrating two para-aortic FDG avid lymph nodes on the left side at the level of L2 vertebra, as indicated by the yellow arrow.
The Eastern Cooperative Oncology Group (ECOG) performance status for the patient was zero, serum lactate dehydrogenase (LDH) was elevated (303 U/L) and international prognostic index (IPI) score was zero, signifying the low risk of the disease. Consequently, the clinical stage of the disease was Stage IIAE.
3 Discussion
Primary testicular DLBCL is a rare neoplasm with typical manifestation in the older age. This study documents the first case of primary testicular DLBCL from Pakistan, as part of the centralized registry program for uncommon tumors project, a recent but fast spreading project focused at the comprehensive study (and database) of rare tumors in Pakistan [Citation13Citation[14]–Citation15] .
Primary testicular DLBCL are usually related to high morbidity and mortality rates. The clinical presentation of primary testicular DLBCL includes swelling of testis, B-symptoms (i.e., fever, night sweats and weight loss) and elevated LDH levels [Citation4]. Typically, these tumors are characterized by a high risk to disseminate to the CNS, thereby warranting routine CNS prophylaxis with chemo- or radio-therapy [Citation3,Citation8] .
Imaging of tumor metabolism with FDG PET/CT for the initial staging, follow up, treatment response monitoring and assessment of disease relapse in lymphomas has become a valuable molecular technique [Citation9Citation[10]Citation[11]–Citation12] . Indeed, PET has been recommended for evaluating the initial staging of patients presented with DLBCL [Citation16], as carried out in this study. Specifically, two para-aortic FDG avid lymph nodes exhibiting SUVmax of up to 9.79 and size of 1.1 × 1.5 cm were seen, which rendered the clinical stage to IIAE. Moreover, the intensity of FDG uptake, and consequently SUVmax values, in lymphoma patients is a multifactorial process, comprising of histologic type, grade, tumor proliferative index, upregulation of glucose metabolism, the presence of hypoxia, etc. [Citation16]. For instances, several studies have shown that high-grade lymphomas (e.g., DLBCL) are more FDG avid (i.e., threefold higher SUV) than are low-grade lymphomas [Citation16,Citation17] .
Our patient presented with three months history of left testis swelling, and underwent unilateral (left) radical orchiectomy for both diagnostic and therapeutic purposes [Citation6,Citation18,Citation19] . Indeed, radical orchiectomy appears the primary intervention to achieve favorable outcomes of the treatment [Citation18]. However, orchiectomy alone should not be considered as the sole treatment of DLBCL, as indicated by several studies. Specifically, patients treated with orchiectomy alone would mostly experience disease relapse within two years; 5–35% in the contralateral testis [Citation20]. Additionally, relapses to distant extranodal sites, particularly to CNS, also remains a major therapeutic challenge [Citation3,Citation8] . In this context, we have planned doxorubicin-based chemotherapy for our patient. In particular, six courses of cyclophosphamide (750 mg/m2), doxorubicin (50 mg/m2), vincristine (1.4 mg/m2) and prednisone (100 mg/m2) (CHOP) along with intrathecal Methroxate (MTX; 12 mg) have been planned on day one with three weeks interval, which would presumably improve the prognosis [Citation21]. Importantly, the patient is non-affording for rituximab.
4 Conclusion
We presented an uncommon but aggressive case of primary testicular diffuse large-B cell lymphoma (DLBCL), whose diagnostic work-up was carried out with surgery and FDG PET/CT. Specifically, histopathology findings from the tissue samples obtained from unilateral (left) radical orchiectomy rendered DLBCL of testis. Thereafter, PET/CT demonstrated two FDG avid lymph nodes in the para-aortic region. Presently, the patient has been planned for doxorubicin-based chemotherapy (i.e., cyclophosphamide, doxorubicin, vincristine and prednisone; CHOP) along with intrathecal Methroxate (MTX), which would presumably improve the prognosis. Our study demonstrated that DLBCL of testis is a rare disease where PET/CT plays an important role towards the assessment of local or distal spread of the disease.
Source(s) of support in the form of grants, equipment, drugs, or all of these
None.
References
- P.De PaepeC.De Wo-PeetersDiffuse large B-cell lymphoma: a heterogeneous group of non-Hodgkin lymphomas comprising several distinct clinicopathological entitiesLeulemia2120073743
- Y.XieS.PittalugaE.S.JaffeThe histological classification of diffuse large B-cell lymphomasSemin Hematol52220155766
- W.ChenJ.KuoC.LinH.ChungW.J.S.HuangH.H.H.Wuet al.Primary testicular lymphoma – a single center experience and review of literatureUrol Sci201615 Elsevier Taiwan LLC
- J.D.GundrumM.A.MathiasonD.B.MooreR.S.GoPrimary testicular diffuse large B-cell lymphoma: a population-based study on the incidence, natural history, and survival comparison with primary nodal counterpart before and after the introduction of rituximabJ Clin Oncol2731200952275232
- Y.KemalF.TekerG.DemiragI.YucelPrimary testicular lymphoma: a single center experienceExp Oncol3732015223226
- K.N.LokeshV.SathyanarayananL.KuntegowdanahalliT.M.SureshL.DasappaG.B.K.KanakasettyPrimary diffuse large B-cell lymphoma of testis: a single centre experience and review of literatureUrol Ann632014231234
- J.O.ArmitageStaging non-Hodgkin lymphomaCA Cancer J Clin5561993368378
- P.SindhuP.LinH.SonD.RosenfeldM.LinTesticular fluorine-18 fludeoxyglucose uptake on positron emission tomography CT in patients with lymphoma: clinical significance and management impactBr J Radiol8720140472
- S.H.KwonD.R.KangJ.KimJ.YoonS.J.LeeS.H.Jeonget al.Prognostic value of negative interim 2-[18F]-fluoro-2-deoxy-D-glucose PET/CT in diffuse large B-cell lymphomaClin Radiol1–72015
- N.NabilL.M.AlotaifyM.ShakerPET/CT in initial staging and therapy response assessment of lymphomaEgypt J Radiol Nucl Med474201616391647 Egyptian Society of Radiology and Nuclear Medicine
- B.D.ChesonR.I.FisherS.F.BarringtonF.CavalliL.H.SchwartzE.Zuccaet al.Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classificationJ Clin Oncol3227201430593068
- S.F.BarringtonA.A.KirkwoodA.FranceschettoM.J.FulhamT.H.RobertsE.Brunet al.PET-CT for staging and early response: results from the response-adapted therapy in advanced Hodgkin lymphoma studyBlood12712201615311539
- M.SadiqI.AhmadJ.ShujaK.AhmadPrimary Ewing sarcoma of the kidney: a case report and treatment reviewCEN Case Rep201714
- J.ShujaI.AhmadK.AhmadH.ManzoorS.KakarM.Sadiqet al.Pleuropulmonary blastomaJ Cancer Res Pract201714
- S.IftikharI.AhmadI.M.QasmiK.AhmadH.ManzoorTuberous sclerosis complex with sub-ependymal giant cell astrocytomas; a case reportJ Cancer Res Pract201714
- F.M.PaesD.G.KalkanisP.A.SiderasA.N.SerafiniFDG PET/CT of extranodal involvement in non-hodgkin lymphoma and hodgkin diseaseRadiographics3012010269291
- R.ElstromL.GuanG.BakerK.NakhodaJ.VergilioH.Zhuanget al.Utility of FDG-PET scanning in lymphoma by WHO classificationBlood10110200338753876
- I.ParkJ.KimD.H.YoonI.ParkS.KimJ.S.Parket al.Treatment of primary testicular diffuse large B cell lymphoma without prophylactic intrathecal chemotherapy: a single center experienceBlood Res4932014170176
- L.R.ScalcioneD.S.KatzM.S.SantoroS.MahboobR.L.BadlerE.Y.YungPrimary testicular lymphoma involving the spermatic cord and gonadal veinClin Nucl Med3442009222223
- H.G.MorenoG.PinottiG.MartinelliR.MozzanaS.GrisantiM.Provencioet al.Patterns of outcome and prognostic factors in primary large-cell lymphoma of the testis in a survey by the International Extranodal Lymphoma Study GroupJ Clin Oncol21120032027
- U.VitoloA.ChiappellaA.J.M.FerreriM.MartelliI.BaldiM.Balzarottiet al.First-line treatment for primary testicular diffuse large B-cell lymphoma with rituximab-CHOP, CNS prophylaxis, and contralateral testis irradiation: final results of an international phase II trialJ Clin Oncol2920201127662772