
Abstract
Malignant pleural mesothelioma (MPM) is a rare and highly aggressive intrathoracic neoplasm that typically offer poor prognosis. In general, development of MPM is linked with a history of asbestos exposure. Herein we report a 56-year-old female patient with MPM, who presented with complains of chest pain, cough, shortness of breath and weight loss. The patient’s radiological work-up demonstrated right sided plural effusion with circumferential plural thickening and loss of lung volume. Histopathological features in tandem with immunohistochemical (IHC) study were consistent with the diagnosis of MPM. Our study illustrate that MPM is an uncommon and highly aggressive malignancy associated with poor prognosis.
1 Introduction
Malignant pleural mesothelioma (MPM) is a rare intrathoracic neoplasm that typically offer poor prognosis. Early diagnosis of MPM is primarily compromised by the extremely long latency period pertaining to the development of the tumor [Citation1]. Radiological features such as unilateral pleural effusion, nodular thickening of pleura and interlobar fissure thickening are suggestive of MPM [Citation2,Citation3] . Histopathology in tandem with immunohistochemical (IHC) staining is essentially required to confirm the diagnosis. Distinguishing MPM from other malignancies such as metastatic adenocarcinoma can be highly confounding, particularly for small amount of tissue samples (e.g., sample from needle biopsies) [Citation4]. Similarly, identifying the histopathological subtypes of MPM i.e., the epithelial, the sarcomatoid (fibrous), and biphasic (mixed) also presents a diagnostic challenge [Citation5,Citation6] . For IHC, expression of calretinin, WT-1 and cytokeratin 5/6 in the absence of Ber-EF4 is considered as most sensitive markers for diagnosis of MPM [Citation6,Citation7] . Beside diagnostic challenges, effective treatment of MPM is also limited for most patients [Citation4,Citation6] . Multimodality therapeutic approach comprising of surgery followed by radiation therapy and/or chemotherapy has shown limited survival benefit [Citation8].
Herein, we have presented a case of 56-year-old female MPM patient, with emphasis on the radiological and histopathological features of this uncommon malignancy.
2 Case report
A 56-year-old female presented to us complaining of chest pain, cough, shortness of breath, weight loss and headache. Hematology analysis revealed marked decrease in platelets (i.e., 94,000/mm3). The patient performance status on the scale of Eastern Cooperative Oncology Group (ECOG) was one. Initial chest x-ray of the patient showed right pleural thickening and obliteration of cardio-phrenic and costo-phrenic angles. Additional radiological work-up, i.e., Computed Tomography (CT) study of chest revealed right sided plural effusion with circumferential plural thickening and loss of lung volume, as shown in A. Soft tissue density area in retro-areolar region of left breast was also observed. Surgery (radical or pleurectomy) was not possible due to high tumor burden. The patient remained at home without any management for 03 months. Thereafter, CT-guided plural incisional biopsy (specimen size = 2.5 × 2 × 1 cm) revealed infiltrating neoplastic lesion composed of sheets, nests and cluster of cells with focal glandular pattern having cells with round to polygonal morphology and having moderate to abundant eosinophilic cytoplasm and hyperchromatic, pleomorphic nuclei with prominent nucleoli. Scattered multinucleated cells were also identified. Special stain PAS/AB highlighted glycogen in the tumor cells. IHC staining showed the following patterns: calretinin, cytokeratin 5/6, cytokeratin CAM 5.2, Wilms tumour antigen-1 (WT-1) and cytokeratin 7 were positive while cytokeratin 20, CDX2, MR and P63 were negative. All these morphologic and IHC features (), in tandem with radiological findings, (summarized in ) were indicative of MPM. Additional analysis showed that other biochemical measures were within normal limits. Pelvic ultrasound also demonstrated no abnormality.
Fig. 1 Illustrative CT scan images of chest region showing the MPM tumor; (A) initial images illustrating right sided plural effusion with circumferential plural thickening and loss of lung volume indicated by the green arrows, (B) images after 03 months showing evidence of disease progression indicated by the red arrows.
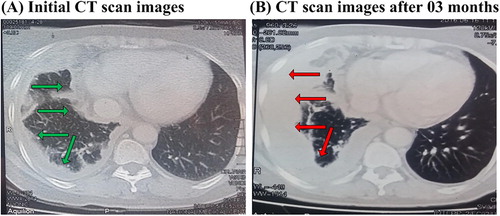
Fig. 2 Illustrative histopathology and IHC images of the pleural incisional biopsy specimen. (A) H&E stain (100X) demonstrating neoplastic lesion of focal glandular pattern having cells with round to polygonal morphology and moderate to abundant eosinophilic cytoplasm and hyperchromatic, pleomorphic nuclei with prominent nucleoli, (B) and (C) shows positive the patterns of calretinin and cytokeratin 5/6, respectively.
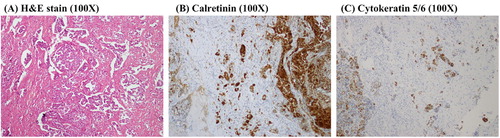
Table 1 Summary of clinical features of the MPM patient, tumor characteristics and status of immunochemical staining.
3 Discussion
Malignant pleural mesothelioma (MPM) is a rare tumor, with highest incidence rates reported from UK (i.e., for men ∼3.3–3.6 per 100,000 and for women ∼0.5–0.7); the trends of global MPM epidemics has been reported comprehensively [Citation9,Citation10] . However, no cohort of MPM has been reported from Pakistan yet [Citation9]. In this context, we have initiated a centralized registry program for rare tumors, such as MPM. Indeed, we have begun to implement the program [Citation11,Citation12] ; this study which reports the first case of MPM from Pakistan is part of the mentioned project. We believe that this program would ascertain a reliable database of rare tumors, enabling the assessment and comparison of our rare tumor epidemics. Moreover, the project would ultimately provide insight into the treatment protocols of these rare tumors and their outcomes, with particular emphasis on the local and individual patient circumstances, and patient values.
Asbestos exposure presumably remains the major factor that modulates the pathogenesis of MPM [Citation13], particularly in older patients while younger patients have been reported to exhibit higher susceptibility of non-asbestos related MPM [Citation14,Citation15] . However, there was no history of asbestos exposure in our 56-year-old patient. Alternatively, it is likely that genetic predisposition may increase the risk of MPM manifestation. Indeed, the risk of MPM development has been previously linked with mutations in the germline BRCA1 associated protein-1 (BAP1) [Citation16Citation[17]–Citation18] . Our patient did not cooperated to carry out a comprehensive study of genetic susceptibility. Nevertheless, we found that the two most sensitive markers of MPM (i.e., calretinin and cytokeratin 5/6) were positive on IHC [Citation6,Citation7] . Overall, it appears that the diagnosis of MPM can be difficult and requires knowledge of the clinical presentation of the disease.
The prognosis of MPM is usually very poor, most probably due to the long latency period [Citation1] and highly aggressive nature of the disease. The reported crucial prognostic factors for MPM includes performance status, age, sex, white blood cell (WBC) and platelet counts, lactate dehydrogenase (LDH), weight loss, etc. [Citation19Citation[20]Citation[21]–Citation22] .
It has been recommended that the decision of a particular clinical intervention (e.g., surgery, chemotherapy, radiotherapy or any combination of them) for the management of MPM should be correlated with the individual patient values and the local circumstances [Citation1,Citation23] . In particular, multimodality therapeutic approach comprising of surgery followed by radiation therapy and/or chemotherapy has shown limited survival benefit [Citation8]. Specifically, the recommended first line chemotherapy agents are pemetrexed and cisplatin, while gemcitabine and carboplatin may be used as second line agents [Citation7,Citation24Citation[25]–Citation26] . Carboplatin has been accepted as an alternative to cisplatin and, more importantly, may be better tolerated in the elderly patients [Citation27,Citation28] .
4 Conclusion
In this study, we presented a case report of malignant pleural mesothelioma (MPM). Many studies have suspected a correlation between the history of asbestos exposure and development of MPM; however, our patient had no history of asbestos exposure. MPM is speculated to be a highly aggressive disease with poor prognosis, as seen in this study. Specifically, the patient remained at home without any management for 03 months, which substantially deteriorated the prognosis. Thereby, early diagnosis of MPM followed by a multimodality therapeutic approach may improve the prognostic index.
5 Conflict of interest
None
References
- A.ScherpereelP.AstoulP.Baaset al.Guidelines of the European respiratory society and the European society of thoracic surgeons for the management of malignant pleural mesotheliomaEur Respir J352010479495
- N. VanZandwijkC.ClarkeD.Hendersonet al.Guidelines for the diagnosis and treatment of malignant pleural mesotheliomaJ Thorac Dis52013E254E307
- Z.J.WangG.P.ReddyM.B.Gotwayet al.Malignant pleural mesothelioma: evaluation with CT, MR Imaging, and PETRadioGraphics242004105119
- T.J.BarreiroP.J.KatzmanMalignant mesothelioma: a case presentation and reviewJ Am Osteopath Assoc1062006699704
- S.C.KaoT.D.YanK.Leeet al.Accuracy of diagnostic biopsy for the histological subtype of malignant pleural mesotheliomaJ Thorac Oncol62011602605
- M.MiettinenJ.LimonA.NiezabitowskiJ.LasotaCalretinin and other mesothelioma markers in synovial sarcoma analysis of antigenic similarities and differences with malignant mesotheliomaAm J Surg Pathol252001610617
- P.BaasD.FennellK.M.Kerret al.Malignant pleural mesothelioma: ESMO clinical practice guidelines for diagnosis, treatment and follow-upAnn Oncol262015v31v39
- Weder W, Opitz I. Multimodality therapy for malignant pleural mesothelioma. Ann Cardiothorac Surg. 2012:502–507.
- C.BianchiT.BianchiGlobal mesothelioma epidemic: trend and featuresIndian J Occup Environ Med1820148288
- S.J.HenleyT.C.LarsonM.Wuet al.Mesothelioma incidence in 50 states and the District of Columbia, United States, 2003–2008Indian J Occup Environ Med192013110
- M.SadiqI.AhmadJ.ShujaK.AhmadPrimary Ewing sarcoma of the kidney: a case report and treatment reviewCEN Case Reports62201713213510.1007/s13730-017-0259-0
- J.ShujaI.AhmadK.Ahmadet al.Pleuropulmonary blastomaJ Cancer Res Pract432017111114
- D.H.YatesB.CorrinP.N.StidolphK.BrowneMalignant mesothelioma in south east England: clinicopathological experience of 272 casesThorax521997507512
- J.BrennerP.P.SordilloG.MagillMalignant mesothelioma in children: report of seven cases and review of the literatureMed Pediatr Oncol91981 967-373
- S.TunesiD.FerranteD.Mirabelliet al.Gene-asbestos interaction in malignant pleural mesothelioma susceptibilityCarcinogenesis36201511291135
- J.XuY.KadariyaM.Cheunget al.Germline mutation of Bap1 accelerates development of asbestos-induced malignant mesotheliomaCancer Res74201443884397
- M.CheungJ.TalarchekK.Schindeleret al.Further evidence for germline BAP1 mutations predisposing to melanoma and malignant mesotheliomaCancer Genet2062013206210
- J.R.TestaM.CheungJ.Peiet al.Germline BAP1 mutations predispose to malignant mesotheliomaNat Genet43201110221026
- B.D.CurranT.SahmoudP.Therasseet al.Prognostic factors in patients with pleural mesothelioma: the European Organization for Research and Treatment of Cancer experienceJ Clin Oncol161998145152
- J.E.HerndonM.R.GreenA.P.ChahinianJ.M.CorsonY.SuzukiN.J.VogelzangFactors predictive of survival among 337 patients with mesothelioma treated between 1984 and 1994 by the cancer and leukemia group B∗Chest1131998723731
- B.GrigoriuA.ScherpereelP.Devoset al.Utility of osteopontin and serum mesothelin in malignant pleural mesothelioma diagnosis and prognosis assessmentClin Cancer Res13200729282936
- R.SpirtasR.R.ConnellyM.A.TuckerSurvival patterns for malignant mesothelioma: the SEER experienceInt J Cancer411988525530
- G.GuyattD.GuttermanM.H.Baumannet al.Grading strength of recommendations and quality of evidence in clinical guidelines; report from an American College of ChestChest1292005174181
- J.P. VanMeerbeeckR.GaafarC.Manegoldet al.Randomized phase III study of cisplatin with or without raltitrexed in patients with malignant pleural mesothelioma: an intergroup study of the European organisation for research and treatment of cancer lung cancer group and the national cancer instituteJ Clin Oncol23200568816889
- N.J.VogelzangJ.J.RusthovenJ.Symanowskiet al.Phase III study of pemetrexed in combination with cisplatin versus cisplatin alone in patients with malignant pleural mesotheliomaJ Clin Oncol21200326362644
- G.ToyokawaM.TakenoyamaF.Hiraiet al.Gemcitabine and vinorelbine as second-line or beyond treatment in patients with malignant pleural mesothelioma pretreated with platinum plus pemetrexed chemotherapyInt J Clin Oncol192014601606
- A.SantoroM.E.O.BrienR.A.Stahelet al.Pemetrexed plus cisplatin or pemetrexed plus carboplatin for chemonaıve patients with malignant pleural mesothelioma: results of the international expanded access programJ Thorac Oncol32008756763
- G.L.CeresoliB.CastagnetoP.A.Zucaliet al.Pemetrexed plus carboplatin in elderly patients with malignant pleural mesothelioma: combined analysis of two phase II trials Study designBr J Cancer9920085156