
Abstract
Two cases of lipomatosis of the parotid salivary gland in two dogs are reported. Both dogs were presented with a slow growing unilateral non-painful mass in the parotid region. The mass measured 12 and 15 cm on the longest axis for case 1 and 2 respectively. Initial incisional biopsies were suggestive of infiltrative lipoma or salivary gland adenocarcinoma. Case 2 underwent head radiographs that showed a soft tissue opacity on the area of the right parotid gland followed by a computed tomography that showed a multi-lobulated infiltrative mass occupying the right parotid gland. Both cases underwent total parotidectomy with an excisional biopsy intent. Surgery on case 1 included total ear canal ablation (TECA). Histology revealed lipomatosis of the parotid gland with a similar admixture of adipocytes and well-differentiated salivary acini on both cases. No recurrence was reported by 4 years for case 1 and by 3 years for case 2. Case 1 developed long-term right-sided facial paralysis and palpebral reflex deficit due to damage of the facial and trigeminal nerve during surgery. The cases are described and the veterinary literature is reviewed in view of the most updated information available in human medicine on fat-containing salivary gland lesions. Considering this literature review, authors recommended these two cases to be classified as lipomatosis of the salivary gland. In conclusion, fat-containing salivary gland lesions should be considered in the list of differential diagnoses in dogs with an enlarged salivary gland and seem to be associated with an excellent prognosis after surgical excision.
Introduction
Primary salivary neoplasia is rare in dogs and clinical signs are usually non-specific. In most cases the neoplasm is malignant with adenocarcinoma being the most common histological subtype. Other primary salivary malignancies in dogs include osteosarcoma, mast cell tumour and malignant fibrous histiocytoma. Enlargement of the salivary gland in dogs can also be caused by benign neoplastic and non-neoplastic processes such as salivary adenoma, sialoadenosis, salivary cyst and salivary infarct [Citation1–Citation8].
In human patients the salivary gland can also be enlarged due to fat-containing lesions. These are uncommon and include sialolipoma, salivary lipomatosis, lipoadenoma, angiolipoma and adenoma with lipometaplasia [Citation9–Citation12]. In dogs there are few reported cases of fat-containing salivary gland lesions and most of these have been classified as either sialolipoma or salivary lipomatosis [Citation7,Citation13]. Sialolipoma and salivary lipomatosis are histologically similar and in human medicine the distinction between these two entities is based on the presence (sialolipoma) or absence (salivary lipomatosis) of a capsule at the periphery of the lesion [Citation11].
Unfortunately, this diagnostic criterion has not been strictly applied in all veterinary publications, leading to some confusion in the classification of these lesions in dogs.
The authors here describe two cases of parotid lipomatosis and discuss the veterinary literature in view of the most updated information available in human medicine for fat-containing salivary gland lesions.
Cases presentation
Case 1: A 6-year-old neutered male Border Collie dog was referred to the “Institution 1” with an over 8-month history of a progressively enlarging soft tissue mass in the right parotid region. The mass had been biopsied twice (incisional biopsies) 7 months and 4 weeks before referral. Histology of the first biopsy was suggestive of an infiltrative lipoma whilst the second examination suggested a well-differentiated salivary gland adenocarcinoma. Both biopsies were performed in a private veterinary diagnostic laboratory. Slides were not available for review.
Upon presentation, a well-defined approximately 12 cm in diameter dense soft tissue mass was observed in the right parotid region (). The mass was mobile and non-painful. On palpation, the mandibular lymph nodes were normal. Haematology and biochemistry were unremarkable. Inflated lateral and ventro-dorsal thoracic radiographs and abdominal ultrasound were unremarkable.

The owners declined further investigations and elected to proceed for exploratory surgery.
Exploratory surgery and total parotidectomy was performed using a right lateral approach to the parotid region. The mass was adherent to the right external ear canal and therefore, Total Ear Canal Ablation (TECA) of the right ear was performed. Part of the facial and trigeminal nerves had to be sacrificed. Right-sided facial paralysis and deficit of the palpebral reflex developed post-operatively.
Histological examination of the excised tissue performed by a board-certified pathologist showed expansion of the salivary gland by a non-capsulated mass composed of mature adipose tissue interspersed with well-differentiated salivary acini and ducts ().
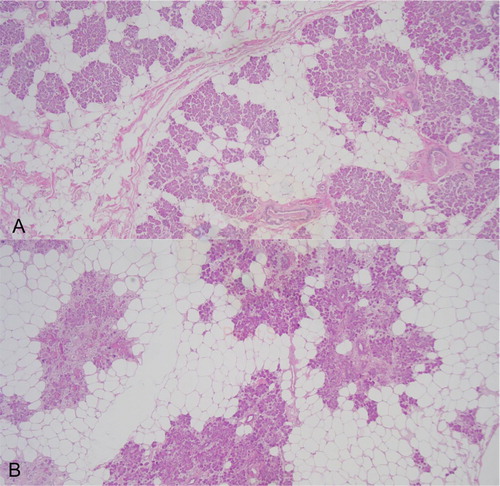
Adipocytes occupied approximately 50% of the mass. Given the lack of a capsule, this fat-containing lesion was classified as salivary lipomatosis.
Four years after surgery there was no evidence of recurrence or systemic disease. The facial paralysis and deficit on palpebral reflex persisted, although the owners reported the dog having a normal life.
Case 2: A 10-year old entire male English Setter was referred to “Institution 2” with a 3 years history of a progressively enlarging right retromandibular soft tissue mass. Two and half years before referral, incisional biopsy revealed glandular atrophy and fibrosis with mild chronic inflammation. Slides were not available for review.
Upon presentation, an approximately 15 cm in diameter dense soft tissue mass was observed in the right retromandibular region (). Physical examination was otherwise unremarkable.
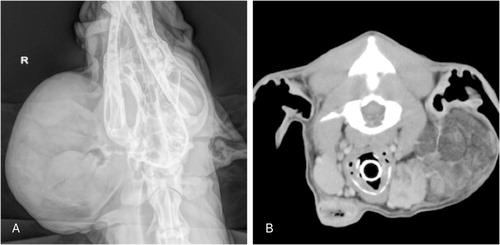
Dorso-ventral radiographs of the head showed a well-defined soft tissue opacity in the parotid area with no evidence of osteolysis (). Computed Tomography (CT) scan of the affected region showed a severe but not infiltrative irregular lobulation of the right parotid gland ().
Total parotidectomy was performed using a lateral approach with an incision parallel and caudal to the mandibular branch, over the vertical canal. The mass was dissected, sparing the horizontal canal and the facial nerve. A smaller adjacent mass was found during surgery and also excised from the right retro-parotid area. The right mandibulary salivary gland was also excised.
Histological examination of the excised tissue performed by a board-certified pathologist showed a non-capsulated expansion of the gland composed of lobules of mature adipocytes intermingled with lobules of salivary acini and ducts (). Adipocytes occupied approximately 60% of the mass. There was no evidence of concurrent inflammation or fibrosis. Given the lack of a capsule, this fat-containing lesion was classified as salivary lipomatosis. Histology of the right mandibulary gland was unremarkable.
The dog died 3 years later from non-related causes and no local recurrence was evident.
Discussion and review of literature
Fat-containing salivary gland lesions are uncommon in human patients and only few cases have been reported in dogs (). In dogs most of these lesions affect the parotid or submandibular salivary gland. There is a single report of a salivary angiolipoma (benign tumour composed of adipose tissue and blood vessels) within the parotid gland [Citation4], but all the other canine fat-containing salivary gland lesions (14 cases) have been described as consistent with either sialolipoma (3 cases) or salivary lipomatosis (also known as lipomatous/fatty infiltration of the salivary gland) (11 cases). Sialolipoma and salivary lipomatosis are histologically similar as they both consist of mature adipose tissue intermingled with well-differentiated salivary gland tissue. In human medicine the distinction between these two histopathological entities has been recently detailed [Citation9]. The most distinctive feature is the peripheral capsule, which is present in sialolipoma and absent in lipomatosis. The 3 cases described as sialolipoma in dogs were reported to have the typical peripheral capsule [Citation7,Citation8]. However, a peripheral capsule was also present in a case that was classified as lipomatosis [Citation14] and that, in the authors’ opinion, would need to be reclassified as sialolipoma. In addition, there are 3 published canine cases of lipomatosis/fatty infiltration of the salivary gland for which it is not described whether a capsule was present or not [Citation6].
able 1 Description of the cases of fat-containing salivary gland lesions found on a literature review, including original diagnoses and proposed diagnoses in the authors’ opinion.
We believe that a strict application in veterinary medicine of the human diagnostic histological criteria for classifying fat-containing salivary gland lesions would allow an easier comparison with the human literature and to more precisely determine the incidence of these lesions in dogs.
The reason why sialolipoma and salivary lipomatosis in human medicine are considered as separate entities is because sialolipoma is, by definition, a neoplastic process, whereas lipomatosis is suspected to represent a non-neoplastic condition, possibly secondary to an underlying obstructive or inflammatory disease of the gland [Citation9]. Interestingly, in one of the two canine cases of salivary lipomatosis presented here mild inflammation and glandular fibrosis/atrophy were noticed on an incisional biopsy performed two and a half years before the surgery and these changes might have favoured the development of the lipomatosis.
In human medicine the treatment of choice is surgical excision for sialolipoma as well as salivary lipomatosis and after surgery recurrence has not been described [Citation12]. This is in agreement with the clinical course observed for the two canine patients described here and for the other canine cases documented in the literature.
Although sialolipoma and salivary lipomatosis appear to be associated with an excellent prognosis after surgery, the diagnosis is challenging, as incisional biopsies are frequently misleading. Given the normal appearance of the adipose tissue and salivary gland tissue, cytology is also unlikely to be diagnostic. An increased awareness in veterinary medicine of the existence of these lesions could help pathologists and clinicians in recognizing them, especially when repeated incisional biopsies and fine needle aspirates keep showing a combination of normal adipocytes and salivary gland cells. Advanced imaging such as Computed Tomography or Magnetic Resonance Imaging scan could also be considered for sample guidance.
In conclusion, fat-containing salivary gland lesions should be considered in the list of differential diagnoses in dogs with an enlarged salivary gland and are associated with an excellent prognosis after surgical excision. Amongst these lesions, lipomatosis appears to be the most common, followed by sialolipoma. A strict application in veterinary medicine of the human diagnostic histological criteria for classifying fat-containing salivary gland lesions is advisable.
Competing of interests
No conflict of interests have been declared.
Notes
Peer review under responsibility of Faculty of Veterinary Medicine, Cairo University.
References
- C.A.CarberryJ.A.FlandersH.J.HarveyA.M.RyanSalivary gland tumours in dogs and cats: a literature and case reviewJ Am Anim Hosp Assoc241988561567
- A.HammerD.GetzyG.OgilvieM.UptonJ.KlausnerW.C.KisseberthSalivary gland neoplasia in the dog and cat: survival times and prognostic factorsJ Am Anim Hosp Assoc372001478482
- E.KarbeB.SchieferPrimary salivary gland tumors in carnivoresCan Vet J891967212215
- A.M.KitshoffI.R.MillwardJ.H.WilliamsS.J.CliftR.M.KirbergerInfiltrative angiolipoma of the parotid salivary gland in a dogJ S Afr Vet Assoc8142010258261
- A.KoestnerL.BuergerPrimary neoplasms of the salivary glands in animals compared to similar tumors in manPathol Vet21965201226
- W.L.SpanglerM.R.CulbertsonSalivary gland disease in dogs and cats: 245 cases (1985–1988)J Am Vet Med Assoc31991465469
- R.V.Rodinõ TilveM.FinckJ.D.G.LeachM.J.MacfarlaneSialolipoma of the parotid gland in two dogsVet Rec Case Rep52017e0037610.1136/vetreccr-2016-000376
- K.ClarkP.HannaR.BéraudSialolipoma of a minor salivary gland in a dogCan Vet J5452013467470
- A.AgaimyS.IhrlerB.MärklM.LellJ.ZenkA.HartmannLipomatous Salivary gland tumors: a series of 31 cases spanning their morphologic spectrum with emphasis on sialolipoma and oncocytic lipoadenomaAm J Surg Pathol372013128137
- L.BarnesJ.W.EvesonP.ReichartD.SidranskyWorld Health Organization classification of tumours: pathology and genetics of head and neck tumours2005IARC PressLyon p 276. Available from https://www.iarc.fr/en/publications/pdfs-online/pat-gen/bb9/BB9.pdf
- T.NagaoI.SuganoY.IshidaA.AsohS.MunakataK.YamazakiSialolipoma: a report of seven cases of a new variant of salivary gland lipomaHistopathology3820013036
- S.QayyumR.MeachamM.SebelikN.ZafarSialolipoma of the parotid gland: case report with literature review comparing major and minor salivary gland sialolipomasJ Oral Maxillofac Pathol17120139597
- P.J.BrownV.M.LuckeM.SozmenT.J.WhitbreadJ.M.WyattLipomatous infiltration of the canine salivary glandJ Small Anim Pract381997234236
- E.BindseilJ.S.MadsenLipomatosis causing tumour-like swelling of a mandibular salivary glandVet Rec1401997583584