
Abstract
Malaria remains a major threat to public health. Long-Lasting Insecticide-treated Nets (LLINs) and Indoor Residual Spraying (IRS) have been widely adopted as important malaria prevention and control interventions and have contributed to significant reduction in malaria incidence. However, recently malaria resurgence has been reported in different countries, including Rwanda, indicating that current attempts to control and eliminate malaria may be failing due to environmental changes and changes in human behaviour. Engaging citizens in malaria prevention and control would help them to identify and prioritize their own health concerns and be able to make appropriate decisions. A citizen science approach to monitor ecological changes by providing timely information is likely to support more effective and consistent use of malaria prevention and control interventions. However, the application of citizen science in malaria prevention and control has lagged behind when comparing with areas of disease diagnosis and treatment. In addition, the determinants of participation in such a citizen science program have not been fully analyzed. This paper presents a conceptual model of likely determinants of participation in connective action (sharing and exchange of malaria-related information), effective and consistent use of malaria preventive and control measures (LLINs and IRS) and collective action (participating in public goods for malaria prevention). The model will guide future research on behavioural and contextual factors and may enhance the effective and consistent use of malaria preventive and control interventions.
1 Introduction
According to the World Health Organization (WHO), malaria is one of the most important parasitic and infectious diseases worldwide (CitationWHO, 2016) and contributes heavily to the global disease problem. The Sub-Saharan Africa region, including Rwanda, carries the heaviest malaria burden (CitationWHO, 2016). While Rwanda’s entire population is considered at risk of malaria, 19 of the 30 districts are classified as high malaria endemic areas of which 11 account for more than 76% of the malaria cases (CitationPresident’s Malaria Initiative, 2017). During the last decade, much progress has been made in reducing malaria transmission in Rwanda. This has led the Ministry of Health to set a target of entering the pre-elimination phase (a phase between control and elimination) by 2018 (CitationPresident’s Malaria Initiative, 2015). The malaria reduction was associated with the deployment of malaria prevention and control strategies, early diagnosis, and treatment. Malaria prevention and control measures include the use of Long-Lasting Insecticide-treated Nets (LLINs) and Indoor Residual Spraying (IRS), destruction of breeding sites through environmental management, use of repellents and chemoprophylaxis (CitationAtieli et al., 2011; CitationCréach et al., 2016; CitationGimnig et al., 2016) as well as the use of intermittent preventive treatment among pregnant women (CitationTobin-West & Asuquo, 2013). However, on a large scale, malaria prevention depends most heavily on insecticide-based interventions (LLINs and IRS) (CitationOkumu et al., 2013) to reduce human-vector contact.
Although there has been a significant global reduction in malaria prevalence, many developing countries have recently see a resurgence in the number of malaria cases reported, including countries where malaria preventive measures (i.e., LLINs and IRS) were in place, such as Indonesia, Senegal, Kenya, and Rwanda (CitationMurhandarwati et al., 2014; CitationPresident’s Malaria Initiative, 2016; CitationWotodjo et al., 2015; CitationZhou et al., 2011). This indicates that availability of these measures alone may not be sufficient for achieving continuous malaria reduction (CitationObala et al., 2015). Rwanda has seen an eleven-fold increase in reported malaria since 2011, leading the government of Rwanda to prioritize malaria to achieve the target of pre-elimination (CitationPresident’s Malaria Initiative, 2017).
Malaria prevention and control displays features of a ‘wicked’ public health problem. As first introduced by CitationRittel and Webber (1973), characteristics of a wicked problem are that it is difficult to define, is influenced by complex political and social factors, involves multiple stakeholders, and is managed but not solved. Similarly, as an infectious disease, malaria can be considered a multifactorial problem, involving multiple actors with various needs, and requires a holistic approach integrating many ecological and social factors (Citationvan Woezik et al., 2016). Ecological factors include the variation in space and time of the number of malaria mosquitoes as well as the malaria parasite. This variation is influenced by many environmental variables (e.g., weather, vegetation) (CitationCohen et al., 2012), societal activities (e.g., rice farming) and socio-economic factors (e.g., quality of housing). There is a need to have a coherent monitoring system for malaria vectors, parasites, malaria episodes in humans, and environmental factors. CitationIngabire, Hakizimana et al. (2016) also revealed that as malaria transmission dynamics change, there is a need to establish and continue a regular monitoring of mosquitoes and malaria incidence to sustain the gains from previous malaria prevention interventions.
Although changes in ecological and environmental factors also contribute to malaria resurgence (CitationHay et al., 2002; CitationTong et al., 2017), changing behaviours of the human population at risk is often considered as one of the key factors (CitationDlamini et al., 2017; CitationHay et al., 2002; CitationSetbon & Raude, 2009). The disuse of preventive measures is mainly influenced by people’s beliefs about the seriousness of malaria (CitationDlamini et al., 2017), the perceptions about the protective benefits of malaria preventive measures (CitationGalvin et al., 2011), and various other social and cultural factors. However, human behaviour and its determinants are often not considered in malaria control and prevention (CitationDlamini et al., 2017; CitationGryseels et al., 2015). Malaria preventive and control interventions will remain ineffective unless the same effort is put into understanding human behaviour and the contexts that influence these behaviours as in understanding malaria vectors (CitationDlamini et al., 2017; CitationMwenesi, 2005).
Several studies have indicated that engaging citizens in malaria prevention and control interventions can stimulate their consistent and effective application (CitationBamidele et al., 2012; CitationWatanabe et al., 2015). Community engagement is key as the community members have the best understanding of their barriers to effective interventions and can propose related possible solutions. Engagement empowers citizens and may create ownership in preventive activities. CitationRickard et al. (2011) found that engaging individuals and the community in the creation and implementation of malaria prevention intervention helps in achieving and sustaining almost 100% of bed net usage rates. In their study in rural western Ghana, a community-based participatory approach was used through assistance in the hanging of bed nets and provision of related instructions, the creation of in-home small group education, and a regular home visit for follow-up by trained community members (CitationRickard et al., 2011). The community-based projects consist of involving people affected by a disease or a health event and include them as key partners in the discussion and development of strategies for their protection. However, there is no element of active engagement of citizens in collecting and analysis of observation under study.
A community-based project implemented in the eastern province of Rwanda with the involvement of Community Malaria Action Teams (CMATs) to distribute malaria messages in the community by home visit or through community meetings showed a successful contribution to health literacy to improve the use of preventive measures (CitationIngabire, Hakizimana et al., 2016). These CMATs had received malaria-related trainings throughout the project and some of them especially community health workers had prior malaria-related knowledge. Engaging citizens creates a bidirectional communication flow and interaction within and between communities where individuals are invited to share their views and provide feedback on a particular matter of interest, malaria prevention in this case (CitationWatanabe et al., 2015). In particular, Rwanda plans to support social and behavioural change communication strategies through the use of interpersonal communication, community radio with a focus on community mobilization and engagement in the use of LLINS and early diagnosis and treatment (CitationPresident’s Malaria Initiative, 2017). On this base, Rwanda would be a good place to test the application of a citizen science approach. In a citizen science approach, citizens are actively involved in the collection, and possibly interpretation and analysis of scientific data, in this case for example information about mosquito habitats, mosquito nuisance, and the history of specific malaria episodes. Such a citizen science approach may improve the perceptions related to malaria, malaria vectors, and malaria preventive measures, and thereby stimulate the effective and consistent use of these measures. In addition, Rwanda has implemented the RapidSMS initiative throughout the country, which shows that community health workers can already be actively involved in monitoring malaria incidence in children under the age of five.
Generally, most research projects and studies that are being conducted involve health workers in reporting of health-related events and do not involve the general public (CitationIngabire, Hakizimana et al., 2016; CitationRickard et al., 2011). There is no system to which the health of the larger population can be monitored on a regular basis. Involving citizens in monitoring mosquito dynamics, mosquito habitats, mosquito nuisance, and malaria episode, potentially creates more sustainable malaria interventions, promotes effective use of these interventions and thereby could decrease malaria incidence. However, thus far no studies have been published that evaluate how the involvement of citizens in the monitoring of mosquito dynamics and malaria episode can be set up in an efficient way in rural areas of a country such as Rwanda. It is unclear what factors would determine the participation of people in such a citizen science program. It is also unclear how different levels of engagement or the accuracy and timing of information provided and the communication channels used will determine the number of people reached and influence the human behaviour regarding malaria prevention and control. Therefore, this paper explores potential determinants of two of the most important malaria preventive measures: the use of LLINs and acceptance of IRS. We then describe the potential impact of a citizen science approach to malaria-related behaviour. Afterwards, we present an integrated conceptual model with both individual and collective factors to predict the use of both malaria preventive measures and being actively involved in a citizen science platform which will be described later in the paper and will guide future research. We finally present the key features of a citizen science platform that we aim to implement in Ruhuha, malaria endemic area in Rwanda.
2 Use and adoption barriers to malaria preventive and control measures
The WHO indicated that between 2010 and 2015, the proportion of people sleeping under bed nets has almost doubled in Sub-Saharan Africa (CitationWHO, 2016). CitationEisele et al. (2010) estimated the protective efficacy of LLIN and IRS on the reduction of malaria-attributable mortality among children under the age of five at 55%. Therefore, the WHO Global Technical Strategy for malaria 2016–2030 (2016) stresses that these malaria prevention and control measures should be available and accessible to people at risk (CitationWHO, 2016). Furthermore, these measures should be used effectively and consistently (CitationRussell et al., 2015).
2.1 Consistent, effective use and non use of Long Lasting Insecticide Treated Nets (LLIN)
LLIN provide individual protection by reducing the biting rate and thereby reducing both malaria incidence and malaria mortality (CitationRickard et al., 2011; CitationYasuoka et al., 2014). Together, the availability, acceptability, ownership, and the regular and effective use of LLIN are cardinal to malaria infection-prevention worldwide (CitationLindblade et al., 2015). However, consistent and effective use of LLIN faces major social, economic and cultural challenges (CitationNg’ang’a et al., 2009; CitationWidmar et al., 2009). Many studies have shown a gap between ownership and actual use of LLIN (CitationAtieli et al., 2011; CitationErnst et al., 2016; CitationKateera et al., 2015; CitationMoon et al., 2016). For example, LLIN have been used for constructing chicken pens, fishing or agriculture (CitationHonjo & Satake, 2014; CitationIngabire et al., 2015). Heat and discomfort were reported as barriers to effective use of bed nets (CitationIngabire et al., 2015; CitationRickard et al., 2011). Other studies, however, report low rates of misuse, e.g. only about 3% of study participants in Zambia (CitationMacintyre et al., 2012) and less than 5% in Sierra Leone (CitationBennett et al., 2012). While these studies did not support the assumption that bed nets are diverted for alternative purposes, they confirmed a gap between bed net ownership and use.
These findings suggest that future empirical studies should aim to identify the determinants of effective use and of misuse of malaria preventive and control measures. Understanding the factors that shape behaviour will also help to design effective interventions to close the gap between bed net ownership and use.
To achieve malaria elimination, individual perception and behaviour related to malaria and malaria prevention are important factors that should be addressed in malaria prevention and control programs. Individual perceptions about the seriousness of malaria and related exposure encourage individuals to consistently and effectively use LLIN (CitationMukhopadhyay et al., 2016). In addition, CitationGalvin et al. (2011), found that individuals’ motivation to use LLIN depends on their perceptions related to bed nets’ effect to reduce mosquito nuisance and other protective benefits. Those who use LLIN appear to perceive more malaria preventive benefits of LLIN than preventing mosquito nuisance (CitationBerthe et al., 2014). Comfort (not being annoyed by mosquitoes) while sleeping under bed nets was also reported to encourage people to use LLIN.
The consistent use of LLIN is determined by behavioural factors such as diverting nets to other purposes, using LLIN only during the seasons with a higher risk of mosquito bites (rainy season) and sleeping outdoor (CitationBirhanu et al., 2015; CitationRicotta et al., 2015). Sleeping location (bed versus floor), sleeping arrangements (the number of people sleeping in one bed) and availability of suitable locations for hanging the LLIN were reported to influence the use of LLIN (CitationErnst et al., 2016; CitationIwashita et al., 2010; CitationKateera et al., 2015). Sleeping on the floor mostly occurs in rural areas where beds are rarely available for all household members. The lack of a bed frame makes it difficult to hang the LLIN correctly, (CitationIwashita et al., 2010). Sometimes sleeping locations vary by night depending on weather or evening social activities such as alcohol consumption, particularly for men (CitationAtkinson et al., 2009), and attending particular events like funerals (CitationDunn et al., 2011). Some people even prefer to take malaria preventive medicine because it is easier than sleeping under bed nets (CitationErnst et al., 2016).
At the community level, social support, social pressure, and social norms can influence the consistent and effective use of LLINs by community members (CitationDunn et al., 2011; CitationGraves et al., 2011; CitationRickard et al., 2011; CitationStrachan et al., 2016). Studies have confirmed the importance of encouragement, interpersonal influences, and support from local leaders, village health teams, family members and neighbors to the consistent use of LLIN (CitationErnst et al., 2017; CitationErnst et al., 2016; CitationStrachan et al., 2016). Encouragement and support may be provided through regular home visits for reminding people to use these measures or through direct assistance in case of need, for example by offering assistance in hanging bed nets (CitationStrachan et al., 2016; CitationWatanabe et al., 2015). Interpersonal influences were significantly associated with the use of LLIN in studies in Tanzania (CitationRicotta et al., 2015) and Ghana (CitationErnst et al., 2017). In addition, a study conducted in Nigeria found that individuals who receive information and assistance from their friends and family members were more likely to use bed nets (CitationRussell et al., 2015).
Mosquito density varies over the seasons and this, in turn, affects the way people use LLIN depending on their perceptions of mosquito biting and nuisance. Although LLIN were generally perceived as having a protective effect against malaria, these perceptions differed between the rainy and dry seasons (CitationBeer et al., 2012). During the rainy season, people perceived mosquito nuisance to be high, which increases the likelihood of using LLIN, whereas during the dry season mosquito nuisance is low and the consistent use of LLIN decreases (CitationBeer et al., 2012; CitationMukhopadhyay et al., 2016). Apparently, the belief that bed nets should be used only during the rainy season is widespread (CitationErnst et al., 2016). CitationToé et al. (2009) showed that also in Burkina Faso people tend to use LLIN only when feeling disturbed by mosquitoes. When they are not bothered by mosquitoes, even during the rainy season when high transmission rates of malaria are expected, they do not use LLIN. In addition to mosquito nuisance, comfortability influences the use of LLIN. Sleeping under bed nets during the dry season increases warmth and reduces comfortability. This issue is less prominent during the rainy season when temperatures are lower (CitationErnst et al., 2016; CitationIngabire et al., 2015). CitationWatanabe et al. (2015) showed, however, that with greater perceived seriousness of malaria, people consistently use bed nets even in the dry season. These findings suggest a need to address cognitive perceptions that underestimate the risk of malaria transmission during all seasons as well as the seriousness of a malaria infection (CitationToé et al., 2009).
2.2 Acceptance of Indoor Residual Spraying
In Africa, Indoor Residual Spraying is among the primary malaria vector control interventions (CitationPluess et al., 2010). Many studies have indicated the effectiveness of IRS in decreasing malaria vector densities and malaria transmission (CitationKleinschmidt et al., 2009; CitationPluess et al., 2010; CitationSteinhardt et al., 2013). However, the share of the population at risk of malaria that is protected by IRS has declined globally from 5.7% in 2010 to 3.1% in 2015, and from 10.5% to 5.7% in Sub-Saharan Africa (CitationWHO, 2016). The reduction in IRS coverage is mainly due to lack of financial means to sustain this effort over the long term. IRS is usually used only in particular areas where malaria is endemic and causing outbreaks. For example, in Rwanda, IRS is being executed in only five districts which have been classified as high malaria prevalence and high-risk districts (CitationPresident’s Malaria Initiative, 2017). The effectiveness of IRS decreases when not all rooms in a habitation are sprayed. Bedrooms and storerooms are usually not sprayed (CitationIngabire et al., 2015; CitationKaufman et al., 2012). The main challenge with the implementation of IRS is that in Rwanda it is broadly considered a government responsibility, which creates the perception that targeted individuals are not able to use it (CitationMontgomery et al., 2010). Consequently, the attribution of IRS to the reduction of malaria is still limited and people associate IRS more with reduction of insects rather than seeing it as a malaria control strategy (CitationMunguambe et al., 2011).
The acceptance of IRS is positively associated with cognitive perceptions about its effectiveness in the reduction of insects, decrease of malaria incidence, past experience, and a reduction in the need for medical treatment (CitationKaufman et al., 2012; CitationMunguambe et al., 2011). CitationAtkinson et al. (2010) found that adherence involves a complex interaction between intervention acceptability, malaria risk perception, and socio-cultural factors. Similarly, CitationMontgomery et al. (2010) found that the acceptability of IRS is more influenced by the broader spectrum of the social-cultural and political context such as identity, citizenship, and rights, and is not limited to the physical effects of the spraying activities. For example, participants would criticize their neighbors if they refuse the spraying of insecticide in their house and these neighbors change their attitudes and accept the spraying activity (CitationMontgomery et al., 2010). Interestingly, a citizen reported that he authorized the sprayers to go into their neighbors’ house to spray when they are not around since he considered it his responsibility to support their neighbors in malaria control (CitationMontgomery et al., 2010). Lack of acceptance to IRS due to a weak perception of both malaria risk and effectiveness of IRS was reported (CitationMunguambe et al., 2011). In their study, CitationMontgomery et al. (2010) found that regardless of having accepted the IRS and willingness to accept the future spraying activities, many people don’t believe that IRS is effective against the malaria vector. This is mainly the results of group-based citizenship, hence it becomes a passive form of acceptance through a sense of lack of empowerment to refuse it (). The reported factors that may hinder acceptance of IRS include ignorance of the measure, doubt about the effectiveness and the appearance of other insects such as mites, flies and bed bugs shortly after spraying (CitationIngabire et al., 2015; CitationKaufman et al., 2012; CitationMunguambe et al., 2011).
Table 1 Structured overview of links between malaria problem dimensions, potential causes, and proposed interventions.
Resistance against IRS is also motivated by cognitive believes about the presence of undesirable effects of spraying. These were for example expressed in a report about swelling of the face, itching, rash, asthma, and death of animals that are near the home (CitationIngabire et al., 2015; CitationKaufman et al., 2012). Similarly, the (expected) discomfort during the spraying process, including moving belongings, may reduce acceptance of IRS (CitationIngabire et al., 2015). While community leaders seem to be the most influential in relation to the acceptance of IRS, their eventual non-acceptance of IRS could also reduce the acceptance among community members (CitationMunguambe et al., 2011). Socially shared beliefs about malaria risks may also affect people’s ability to accept IRS. Lack of information and communication around spraying activity could lead to skepticism to the spraying procedures. For example absence of advance notification leads people to refuse spraying upon arrival of the sprayers at their homes (CitationIngabire et al., 2015; CitationMunguambe et al., 2011). Sprayers’ attitudes or conduct towards household members also may cause mistrust and affect the IRS acceptance (CitationIngabire et al., 2015). Generally, household members prefer sprayers whom they know in the community over newcomers, as the latter are considered strangers in their community.
Overall, the evidence suggests that acceptance and consistent use of malaria prevention and control measures are determined by a number of factors at both individual and collective level. Therefore, if individuals are more engaged (example: through citizen science) in malaria prevention and control interventions, then the above-mentioned factors could be affected in a desirable manner.
3 Impact of citizen science approach on malaria-related behaviours
According to CitationRickard et al. (2011), malaria interventions that are embedded in the community and that involve citizens allow more discussion and in-depth analysis on the benefits of those interventions hence may obtain a high level of acceptance and use. Not involving the general public/community members is a missed opportunity because, in the end, they are the receivers of public health programs. Citizen science refers to involving volunteers in observations, classification, and collection of data, which in turn are used by researchers (CitationCohn, 2008; CitationKullenberg & Kasperowski, 2016). Other authors consider citizen science as public engagement in scientific research with members of public joining scientists together to collect and analyze large quantities of data (CitationBonney et al., 2016). Citizen science comprises a wide range of projects involving citizens in the practice of science, varying from participatory action research to a large web-enabled effort that involves multiple fields around the world (CitationCrain et al., 2014). Besides the collection of scientifically sound data, the goal of citizen science is also to engage citizens in conversation and decision making about environmental threats and related issues (CitationBonney et al., 2016) (see ).
Apart from increasing public awareness, citizen science reinforces people’s intentions towards an intervention under study (CitationBonney et al., 2016; CitationCrall et al., 2012). Examples, attending community events, removing local invasive species, and educating peers about invasive species (CitationCrall et al., 2012). However, in some projects, there may not be a noticeable behaviour change mainly due to self-selection of the participants who may already have positive behaviour towards the intervention under study at the start of the project (CitationBonney et al., 2016). Due to its ability to provide quality controlled information (CitationAceves-Bueno et al., 2015), a well-designed citizen science program can enhance human-nature relationships () and provide feedback loops (CitationCrain et al., 2014), which in turn contributes to the effective and consistent use of malaria prevention and control measures.
Citizen science projects such as Allergy Radar (Citationde Weger et al., 2014), Tick Radar (CitationGarcia-Martí et al., 2017) and Mosquito radar (CitationKampen et al., 2015) in the Netherlands show that thousands of people can be actively engaged in reporting a broad range of health-related and ecological observations over several years. CitationAceves-Bueno et al. (2015) argue that citizen science is an appropriate method to collect and monitor information and can also lead to a high level of community engagement. This engagement creates new social-ecological interactions (e.g. reflection on observed environmental changes and exposure to different social norms) (CitationCrain et al., 2014). In turn, this exposure to different social norms may influence dynamic interactions, may develop new community norms and values, or change, reinforce and further develop the existing norms and values (CitationDen Broeder et al., 2016; CitationDen Broeder et al., 2017) (). CitationDen Broeder et al. (2017) also argue that being a participant in citizen science extends one’s social network, improves social cohesion, and increases participation in collective activities. presents the link between the different dimensions of the malaria problem, different barriers to use malaria preventive measures, and the potential role of citizen science to overcome these barriers.
The technological possibilities of engaging the public and specific stakeholders in scientific research are increasing because of the increased availability and adoption of mobile phone technology and the increasing access to the internet (CitationCole-Lewis & Kershaw, 2010).
Many studies involving mobile phone technology have been conducted in developed countries that have involved citizens in collecting and analyzing data. However, in the extant literature, only few projects focus on African countries with much emphasis on HIV/AIDS and non-communicable diseases (CitationBloomfield et al., 2014; CitationForrest et al., 2015). Yet, Zurovac, Talisuna, & Snow (2012) identified several studies that used mobile phone text messaging in the areas of malaria surveillance (mainly case detection), management, and monitoring. For example, in Rwanda, mHealth (RapidSMS) has been used for early reporting of pregnancies, diagnosing, and treating diseases among children under the age of five (CitationNgabo et al., 2012). mSpray, a mobile phone-based project to increase malaria control through the use of IRS in South Africa showed the importance of timely and accurate data provision, monitoring of spray activities and improving opportunities for more location-targeted mosquito control (CitationEskenazi et al., 2014). Such projects provide real-time information to individuals and allow accurate and efficient disease monitoring, prevention and control (CitationHounmanou et al., 2016). Most of these projects used mobile phone SMS reminders to increase treatment adherence, but a few projects have also targeted the promotion of preventive health behaviours (CitationFjeldsoe et al., 2009), such as the anti-obesity behaviour modification project in Korea (CitationJoo & Kim, 2007), and a college smoking cessation project in Washington DC (CitationObermayer et al., 2004). However, there is a little-published inquiry into the success factor of such projects.
Other studies have highlighted that implementation of digital technology-based projects in disease control and prevention would improve the care that the existing health system could not address, particularly for people at risk (CitationAsiimwe-Kateera et al., 2015). According to CitationZurovac et al. (2012), health service delivery and health outcomes could be improved by the use of mobile phone applications or platforms. CitationCole-Lewis and Kershaw (2010) argued that digital technology-based projects provide an interactive two-way communication, which in turn stimulates information sharing. CitationMeankaew et al. (2010) showed that the integration of mobile technology in malaria prevention and control programs can improve real-time malaria case investigation and active follow-up of those which may be positive. Another example comes from Ruhuha, Rwanda, where CMATs were formulated to identify malaria-related problems and find solutions to these problems. These teams facilitated both connection between the community malaria action teams and the community at large as well as knowledge exchange (CitationIngabire, Kateera et al., 2016). This, in turn, increased the acceptance and the use of available malaria preventive measures as well as participation in community activities aimed at malaria elimination.
The spread and broad availability of new communication technologies such as mobile phones and internet enable novel communication approaches to enhance the frequency, interactivity, and quality of citizen engagement and this may also be used to enhance malaria prevention strategies. However, engagement of all actors in new communication technologies in malaria prevention requires that different domains should be interested and convinced about its usefulness. This engagement also needs a clear and explanatory model that looks at the various levels of malaria prevention. Such a model is currently still lacking. Having an explanatory model for malaria prevention and control remains crucial, as it would show factors that need to be considered when targeting malaria elimination. In the next section, we work out an integrated model of determinants of malaria prevention behaviour. The model proposes that by participation in a citizen science platform through collection and reporting of information related to ecological data and history of possible malaria episode, there may be an increase of connective action (i.e. interaction, sharing and exchange of malaria-related information among the participants) and collective action.
4 Conceptual model to predict use of malaria preventive measures and the citizen science platform
We put forward the idea that both individual and socio-cultural factors need to be a central component of malaria prevention and control strategies. Therefore, our model shows clearly how these factors are connected to each other () and how leaving these factors out of the malaria control plan might affect the success of the implementation of the interventions
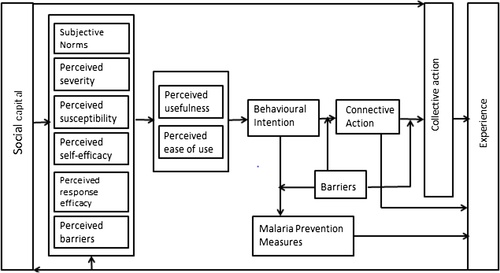
Table 2 Source of the concepts presented in .
4.1 Underlying theories
Given the complexity of behavioural research, no single theory exists that covers all important individual and social factors, and thoughtful selection and combination of theories may result in more robust interventions. Therefore, three well-established theories, the Health Belief Model (HBM), the Theory of Planned Behaviour (TPB), and the Unified Theory of Acceptance and Use of Technology (UTAUT) were selected from the field of social psychology and technology adoption. The HBM and the TPB were selected as they are among the first theories that focus on individual health behaviour and remain the most widely used nowadays especially in disease prevention and health promotion. The UTAUT was selected among other technology related models as it is the predominant model deployed in predicting the use of information technology and related products and services. Importantly, it accounts for the influence of social factors on the adoption of technological services. All three theories aim to explain almost similar outcomes from different perspectives. That is, they use behavioral intention as the key predictor of the use of a new practice, product or behaviour and separately each has different determinants of behavioural intention.
As the concepts in different theories may be different but their conceptualization across theories may be similar, we considered the complementarity of these theories, independence, and relationships between concepts, as well as avoiding overlaps when selecting concepts. Therefore some of the concepts were omitted. At the end, we included those selected concepts together into an integrated model of determinants of malaria prevention behaviour that may be used in other behavioural research and other issues related to vector-borne or other infectious diseases. This proposed model is more than combining the selected concepts from three mentioned theories, as other concepts (not from the mentioned three theories) were added based on their theoretical relevance () which demonstrate the originality of this integrated model of determinants of malaria prevention behaviour. In the following section, we briefly explain the three theories used in our conceptual model.
4.1.1 Health belief model
The Health Belief Model (HBM) is one of the best-known social cognition models on individual health-related behaviour (CitationOlsen et al., 2008). Our conceptual model used the following concepts: perceived severity, perceived susceptibility, perceived self-efficacy, and perceived barriers ().
4.1.2 Theory of planned behaviour
The Theory of Planned Behaviour (TPB) is an extension of the Theory of Reasoned Action and the most predictive persuasion theory (CitationMunro et al., 2007). However, it does not account for factors that are beyond individual voluntary control. In our model, we included subjective norms and behaviour intention ().
4.1.3 Unified theory of acceptance and use of technology
The Unified Theory of Acceptance and Use of Technology (UTAUT) is an expansion of the Technology Acceptance Model and is used to describe and predict the acceptance of new information technology and ways of stimulating the use of technology (CitationVenkatesh et al., 2003). In our model, we included perceived usefulness and perceived ease of use. Social influence was not included as it overlaps both with ‘social networks/interactions’ as one dimension of social capital and with ‘subjective norms’. In the following sections, we define each of these concepts and give a theoretical rationale for the relationships presented in the model.
4.2 Description of the concepts/determinants of behaviour
4.2.1 Social capital
Social capital is defined as forms of social organization such as social networks/interactions, norms of reciprocity and generalized trust that facilitate cooperation and coordination for common benefits (CitationPutnam, 1995). Social capital has been described as rooted in social relationships and can serve as a resource that allows individuals to achieve objectives that they could not achieve otherwise (e.g., by people paying each other favours) (CitationColeman, 1988). With regard to malaria prevention, learning from other community members plays a big role in changing perceptions towards acceptance and use of malaria prevention measures. For example, in Rwanda, involving rice farmers in the planning of mosquito larval source management as a malaria control strategy contributed to the change of their perceptions related to the importance of larval source management in malaria control and increased their level of ownership of this action (CitationIngabire, Kateera et al., 2016). In addition, community health workers that are located in all villages of Rwanda play a major role in community mobilization towards malaria prevention. In Bangladesh, CitationAhmed et al. (2014) found this interpersonal communication (with relatives, friends, and neighbors) to be more effective in disseminating and acquiring malaria-related information and in changing perceptions compared to other forms of communication, including mass media and radio. However, in Rwanda, especially in rural areas, radio is among the most powerful sources of information for the citizens as most of the households have at least one radio. Use of social media is less common.
According to CitationPanter-Brick et al. (2006), interventions seem to be most effective when they are linked to cultural narratives (which serve to discuss proper behaviour) and can be strengthened through community support, networks, and interactions. The increase of social interaction and trust can dispel negative perceptions that create individual and community resistance towards engagement in malaria prevention and control measures (CitationAtkinson et al., 2010). Regarding trust in health-related matters, individuals seem to be influenced by those who are well known in the community including local leaders and health workers (CitationAtkinson et al., 2010). Similarly, in Rwanda, CitationIngabire, Hakizimana et al. (2016) found that interpersonal community meetings led by CMATs, CHWs, or village leaders helped to change negative perceptions towards the use of malaria preventive measures and to increase the use of these measures. Therefore, it is hypothesized that social capital has an influence on individual perceptions (perceived severity, perceived susceptibility, perceived self-efficacy, perceived response efficacy and perceived barriers) and subjective norms.
Several studies have indicated that elements of social capital can facilitate collective action, i.e. activities that individuals contribute together with the aim of realizing a public or common good, for example the clearing of mosquito breeding sites (CitationFujiie et al., 2005; CitationIngabire, Hakizimana et al., 2016; CitationRamos-Pinto, 2006). This is also applicable to Rwanda, as citizens engage in monthly community work at the village level (governed by the Rwandan Law) where they gather together in their villages, clean their environment and after that gather to discuss on different topics including malaria. Therefore, it is clear that individuals who obtain information from their interpersonal networks would decide to participate in the creation of public goods if they trust the source of information. Thus, it is predicted that social capital has a positive influence on collective action.
4.2.2 Subjective norms
Subjective norms refer to the perceived social pressure to execute or not execute a behaviour (CitationAjzen, 1991). The theory of planned behaviour developed by CitationAjzen (1991) indicated that although subjective norms influence directly intention to perform behaviour it also importantly influence perceived behaviour control which is similar to perceived ease of use in our model. CitationMunro et al. (2007) also defined subjective norms as a degree to which a person believes that other people in the community think that he/she should participate in a certain behaviour. In their study testing, a theoretical extension of the Technology Acceptance Model (TAM) using longitudinal data collected from four different systems at four organizations, CitationVenkatesh and Davis (2000) found that subjective norms influenced perceived usefulness of information technology in the workplace. This indicates that people integrate social influences in their own usefulness perceptions. In the context of our research model, if a member within a personal environment suggests that a system or a platform might be useful and easy to use, then it is more likely that another person may come to believe the same. This was supported by CitationTeo (2010) who studied the influence of subjective norms on intention to use technology in education and found that subjective norms were direct predictors of perceived usefulness and ease of use. It was also in agreement with a study conducted in Korea by CitationKim and Park (2012) who indicated that the indirect effect of subjective norms on behavioural intention was mediated by perceived usefulness. In contrast, a study conducted among University students in Spain did not find the subjective norm to be a predictor of perceived usefulness (CitationAgudo-Peregrina et al., 2014). This was probably because, in their study, perceived usefulness was used in two dimensions including performance and flexibility. Therefore, we predict that subjective norms positively influence perceived usefulness and perceived ease of use of a citizen science platform.
4.2.3 Perceived severity
Perceived severity is defined as an individual’s beliefs about how serious a disease and its related consequences are. These consequences may range from medical and clinical (disability, pain, death) to social and economic consequences (effect of the disease on family life, work, financial and social relations) (CitationChampion & Skinner, 2008). If people think that malaria could harm them seriously, they are more likely to assign a high value to malaria prevention measures (CitationAnkomah et al., 2012) or to adopt a technology related to malaria prevention and control. In their study conducted among female internet users in Malaysia investigating the influence of perceived health risk on health-related internet use, CitationAhadzadeh et al. (2015) found a positive relationship between perceived severity and perceived usefulness and the latter was a mediating variable towards the internet use. In Korea, CitationKim and Park (2012) developed and tested the extended TAM by analyzing health consumers’ behavioural intention of using health information technology in healthcare. They found a significant effect of perceived severity on perceived usefulness of health information technology. This indicates that perceived severity is essential for people to see the usefulness and perceived ease of use for a particular intervention. Also in the Ruhuha sector in Rwanda, some citizens see the consequences of malaria and are likely to see the usefulness of a citizen science platform as long as it is clearly explained.
Our research model predicts that if an individual perceives the negative effects of malaria, then will consequently perceive the usefulness of malaria preventive and control measures and that using them requires no efforts. Hence, it is hypothesized that perceived severity of malaria positively influences the perceived usefulness of malaria preventive and control measures and related perceived ease of use.
4.2.4 Perceived susceptibility
Perceived susceptibility refers to the beliefs about the likelihood of experiencing or getting a disease (CitationChampion & Skinner, 2008). Individuals who perceive themselves to be at high risk of getting malaria, have higher malaria risk appraisal and are more likely to appreciate the usefulness of malaria prevention interventions. For example, a study done in Nigeria among pregnant women indicated that if pregnant women do not see themselves or their unborn babies at risk of getting malaria, then they are less likely to see the usefulness of malaria prevention and control interventions (CitationAnkomah et al., 2012). The relationship between perceived susceptibility and perceived usefulness was also found in Malaysia (CitationAhadzadeh et al., 2015) and Korea (CitationKim & Park, 2012). If an individual perceives to be at risk of contracting malaria, this will lead to a positive perception of the usefulness of these interventions and that using them requires no or little effort. Thus, it is proposed that perceived susceptibility has a positive influence on both perceived usefulness and ease of use.
4.2.5 Perceived self-efficacy
Perceived self-efficacy refers to people’s beliefs about their capability to use preventive measures. In this paper, perceived self-efficacy is defined as the ability to participate in a citizen science platform and make use of malaria preventive measures through recognition of their usefulness and ease of use. Many technology acceptance related studies including CitationAgudo-Peregrina et al. (2014) conducted in Spain, CitationWang et al. (2006) conducted in Taiwan, and CitationZhang et al. (2016) conducted in China revealed the effect of perceived self-efficacy on perceived ease of use. Others conducted in US, Korea, and Australia found the effect of perceived self-efficacy on both perceived usefulness and ease of use (CitationLee & Mendlinger, 2011; CitationRose & Fogarty, 2006). CitationKim and Park (2012) also found that the greater the self-efficacy the higher the perceived usefulness and perceived ease of use of health information technology. This shows that if an individual perceives being able to use malaria interventions, then it is more likely that he/she will perceive the usefulness of these interventions and that using them requires little to no effort. It is proposed that perceived self-efficacy has a positive influence on perceived usefulness and perceived ease of use.
4.2.6 Perceived response efficacy
Perceived response efficacy is defined as individuals’ beliefs about the effectiveness of recommended behaviour in preventing a threat (CitationWitte, 1992). The association between response efficacy and perceived ease of use of mobile health services was revealed by CitationZhang et al. (2016). In our paper, when individuals believe that a citizen science platform will contribute to the reduction of malaria through information provision, then they find it useful and easy to use. Therefore, the research model proposes that response efficacy is positively associated with the perceived usefulness and perceived ease of use.
4.2.7 Perceived barriers
Perceived barriers refer to people’s evaluation of what would prevent them from using a certain measure while emphasizing on potential negative aspects of a particular health intervention (CitationChampion & Skinner, 2008). If individuals perceive that use of malaria preventive measures has negative side effects, such as increased nuisance of bed bugs or that reporting through the citizen science platform is time-consuming, costly or difficult, then they are less likely to see the usefulness of those interventions. This is also a challenge in Rwanda because past studies indicated that citizens reported bed bugs and warmth to impede the use of bed nets (CitationIngabire et al., 2015). Consequently, we propose that the perceived barriers have a negative influence on the perceived usefulness and perceived ease of use.
4.2.8 Perceived usefulness and perceived ease of use
Perceived usefulness is defined as the extent to which a person believes that using a technology or other measures will improve his/her health outcome (CitationVenkatesh & Bala, 2008). In a malaria prevention context, it may be defined as the extent to which an individual believes that malaria preventive measures may help to prevent getting malaria by reducing human-vector contact. Studies conducted in malaria endemic areas of Nigeria and Burkina Faso indicated that perceived effectiveness and usefulness of LLIN influence the intention to use them (CitationAnkomah et al., 2012; CitationToé et al., 2009). Other mHealth related studies conducted in Uganda (CitationCampbell et al., 2017) and Bangladesh (CitationHoque, 2016) found a positive effect of perceived usefulness on behavioural intention. Therefore, perceived usefulness predicts behavioural intention to participate in a citizen science platform and also to use malaria preventive measures by community members.
Perceived ease of use refers to the degree to which a person believes that the use of a system (CitationDavis, 1989) or a technology CitationVenkatesh and Bala (2008), requires little effort. In their study, CitationAgudo-Peregrina et al. (2014) found that a high level of system complexity and particularly in the case of users with low experience may reduce the intention to use the system. Other mHealth related studies found a positive association between perceived ease of use and behavioural intention (CitationCampbell et al., 2017; CitationHoque, 2016). Thus, in our study, perceived ease of use positively influences the behavioural intention to participate in a citizen science platform and also to use malaria prevention measures by community members.
4.2.9 Behavioural intention
Behavioural intention is defined as the degree to which a person plans to perform a specific behaviour (CitationVenkatesh & Bala, 2008). Behavioural intention is a key predictor of behaviour adoption, here referred to as malaria prevention measures and connective action – a technologically organized process that results in joint action within and between communities and stakeholder groups (CitationBennett & Segerberg, 2012).
Malaria preventive measures include those at individual or community level (use of the LLIN and cleaning of the home environment) as well as those performed by the government (use of IRS). People are likely to use the malaria preventive measures and or share the information via citizen science platform if they have the plan to do so. Following this rationale, our model proposes that behavioural intention has a positive influence on both connective action and use of malaria preventive measures.
By using these malaria preventive measures, people gain experience, which in its turn facilitates the regular and continued use of these measures. Therefore, using malaria preventive measures influences gaining of experience.
4.2.10 Connective action
Connective action is defined as a technologically organized process that may result in joint action (CitationBennett & Segerberg, 2012). CitationDessewffy & Nagy (2016) argued that use of a digital platform has a potential role in spreading information and increasing communication. They added that the use of social media influences collective action. In Rwanda, especially rural areas, the use of social media is less common. Additionally, CitationDiMaggio et al. (2001) revealed that the use of internet provides opportunities to share and exchange information as well as increases socialization. Though the internet is less common in rural areas of Rwanda, this platform can be a channel for building the capacity of the community members in terms of effectiveness of the malaria preventive measures. In turn, this may improve interaction within and between communities and different stakeholders. Example: if a citizen sends information related to malaria and mosquitoes it is likely that first, his/her participation in malaria prevention may increase as a result of improved malaria-related perceptions. CitationDessewffy & Nagy (2016) also revealed the effect of using social media on collective action and extending one’s social network. Secondly, he/she may increase her interaction with neighbours which in turn also increases the chance of this neighbours to participate in sending this type of information. Thirdly, the information shared, perceptions, and behaviour of people who participate in the platform may influence neighbours’ behaviour (using preventive measures). By participating in the platform, there may be an increase in the cleaning of mosquito breeding sites. Consequently, we propose that connective action has a positive influence on collective action. By participating in the platform, there may be an increase in sharing and exchange of malaria-related information which leads to the rise of experience. Accordingly, the model proposes that connective action increases experience.
4.2.11 Barriers
Barriers such as lack of or inadequate malaria prevention measures, on one hand, lack of mobile phones or phone credits to report malaria-related observations on the other hand, as well as the lack of information on usability and productivity of a citizen science platform, may prevent the execution of intended behaviour. While developing an adoption readiness model, CitationWeidman et al. (2015) also identified lack of information about available technology, its usability, productivity, and the associated cost to hinder innovation adoption. In rural areas of Rwanda, most citizens have simple mobile phones and sometimes with no credits and in turn, this may hinder their participation in the citizen science platform. Accordingly, our model proposes that these barriers moderate the effect of behavioural intention on both connective action and use of malaria preventive measures.
Other barriers like resistance to change, ignorance, or lack of motivation may limit the participation in public activities. These barriers may affect the distribution of the potential risks and benefits among community members following the introduction of a citizen science platform at both individual and collective level. Consequently, we propose that these barriers moderate the effect of the connective action on collective action.
4.2.12 Collective action
Collective action is defined as activities that individuals contribute together with the aim of seeking the public good (CitationBennett & Segerberg, 2012). Participation in voluntary associations, groups or clubs is a universal action and members are attracted to join for the same purpose. People are motivated to provide collective good, simply because of the attractiveness of the collective good and common interests to the group members (CitationOlson, 1971). Collective action does not mean involvement of everybody in the community or benefit to everybody, rather of highly motivated and interested individuals who provide collective benefits for the community (CitationOliver & Marwell, 1985). A study conducted in a rural area of Kenya (CitationDiiro et al. (2016) revealed that participation in community activities increases public health awareness and experience in performing related interventions. This may happen through public meetings and community work (CitationRickard et al., 2011). In Rwanda, there is also a community work every last Saturday of the month, and from there, citizens discuss some topics including disease prevention and receive some other important communication from the government. In turn, citizens may improve their awareness on those discussed issues. Consequently, the model proposes that participation in collective action influences people to gain experience.
Experience gained from participation in a citizen science platform, involvement in collective action, and use of malaria preventive measures may lead to a change of perceptions which may turn into the rapid acceptance and consistent use of malaria preventive measures (CitationMozumder & Marathe, 2007; CitationRickard et al., 2011). This experience may also improve trust and social network. Thus, the model proposes that having experience positively influences both individual perceptions and social capital.
The model’s proposed relationships are to be tested through an implementation of the project by using a citizen science approach, in two separate phases. Phase one will test the malaria risk perceptions and perceived efficacy of malaria preventive measures. This includes a baseline survey to determine malaria perceptions and malaria preventive measures in the local community. Phase two encompasses testing the entire model through a second household survey with the aim to evaluate the contribution of a citizen science approach to the consistent use and acceptance of malaria preventive measures. Both phases use a mixed methods approach (quantitative and qualitative) with the aim to achieve triangulation of data.
5 Key features of a future citizen science platform in Rwanda
An integrated project called Environmental Virtual Observatories for Connective Action (EVOCA) is currently underway to design, implement and evaluate a citizen science approach that involves and evaluates the above-described research model. This interdisciplinary project with both social and ecological aspects presents added advantages as it considers all potential social and ecological data, hence prevent missing data in case these aspects are used independently (CitationCrain et al., 2014). This citizen science platform is proposed to complement malaria prevention and control interventions that are currently implemented in Rwanda by the National Malaria Control Program (NMCP). The NMCP has various activities related to malaria prevention especially social and behavioural change communication strategies through the use of interpersonal communication, community radio with a focus on community mobilization and engagement in the use of LLINS and early diagnosis and treatment. The project may also play an important role in sustaining the gains from a community engagement project conducted in Ruhuha, Eastern region, Rwanda (CitationIngabire, Hakizimana et al., 2016; CitationIngabire, Kateera et al., 2016). The EVOCA project planned in Ruhuha sector to involve the existing local infrastructure (CMATs) as useful and knowledgeable resources in the study area may improve their efficiency.
Similar to the other citizen science initiatives on mosquito ecology in Europe (CitationKampen et al., 2015), we envision the citizens to report information via either paper-based forms or via a web-based form. Via paper-based form, citizens are supposed to collect information about mosquito habitats, mosquito nuisance, and history of possible malaria episodes and this information will be digitalized. The paper-based form will be developed and distributed among those who are willing to participate in the project via monthly community work, evening parent meetings (so-called akagoroba k’ ababyeyi), and other meetings that may be planned in the community. Those with smartphones may report through a web-based form.
To empower citizens to become active participants in the project and in the decision-making process regarding malaria, and its prevention, lay information needs to be provided.This may include information about malaria causes, malaria symptoms, malaria preventive and control measures, as well as early diagnosis and treatment.
Participation in citizen science requires community mobilization and motivation. Motivation to participate in a citizen science project includes personal interest in the topic, social interaction, and feedback as an external reward (CitationNov et al., 2011; CitationRotman et al., 2012). Olson also has argued that what motivates people to participate are not economic motives (money related), but rather other forms of motives, including friendship and respect, as well as other social and psychological motives (CitationOlson, 1971). A survey conducted in the Ruhuha sector, after the establishment of CMATs in a community-based project, indicated an increase in personal acceptance and use of malaria preventive measures (CitationIngabire, Hakizimana et al., 2016). This showed that the citizens gained more knowledge related to the burden of malaria, were interested in malaria prevention and were able to make personal decisions making on how to prevent it. Citizens are more likely to continue participation when their contributions are valued throughout the project, when involved in further data analysis and when they get the opportunity to have further training (CitationRotman et al., 2014a). Though participation in citizen science is voluntary, it may also be driven by external parties or social norms (CitationNov et al., 2011). CitationRotman et al. (2014a) also argued that the motivation of volunteers to participate in citizen science projects is affected by both personal and societal interests.
CitationNov et al. (2011) suggested that the design and implementation of a citizen science project should attempt to raise the volunteers’ commitment to the project and related goals. To achieve this, communicating the project’s goals and the intended outcome to the involved volunteers is key. CitationRotman et al. (2014b) added that provision of feedback helps the volunteers to understand what they have contributed. This, in turn, encourages them to do more and continue their participation for the long term. While preparing and discussing the implementation of a citizen science platform and motivation for participation, CitationBennett and Segerberg (2012) emphasized that the scientists should know the great importance of community appreciation, respect and work/production recognition. Appreciation of volunteers is crucial as they are investing their time and even resources without expectation of a monetary reward. The form of feedback provision for our proposed citizen science platform will be discussed beforehand to ensure that it is integrated in the research process.
The inclusion of all stakeholders and their views on this new proposed platform is the first step before the actual design of the platform. Targeting all stakeholders does not automatically mean that they all participate or are willing to participate, as this involve a process of explaining the overall target and how everybody may benefit from that process. Discussing and agreeing on the processes and rules of engagement beforehand may help to create links and working lines among all stakeholders involved. Intensive and continuing interactions and discussion with various parties improves relationships among different stakeholders groups and build up their confidence to become partners in the research process (CitationGiller et al., 2008). This is planned to be done through stakeholder mapping and ensure that key stakeholders are aware of all processes that are expected to be conducted. A study conducted by CitationIngabire, Kateera et al. (2016) in Ruhuha, Rwanda did a stakeholder analysis and indicated three main categories of stakeholders including a primary category (lay community), a secondary category (administrative and health institutions), and a tertiary category who are key stakeholders (policymakers and funders). Thus, this may help to know whom to target, and which message to give to whom mainly at the initial stage.
Similar to other research projects, citizen science projects also encounter challenges and barriers. These include lack of resources for implementation and running the project, lack of or poorly designed technology, and lack of interest among decision makers who are the potential stakeholders, especially when it comes to the sustainability of the project. CitationRotman et al. (2014a) argued that lack of time for participation, technological related problems, and local infrastructural barriers are the key factors to take into account when mobilizing communities. Considering the local context in which the implementation of the citizen science platform will occur, especially taking into account that the citizens are farmers, first of all, many of them may lack time for participation as most of the time they are working at their farms. The level of literacy may also be an issue that may limit them to participate. However, considering that at least one household member knows how to read and write, then this may be less of an issue as long as one can help others to answer any given question or provide any necessary information. Low socioeconomic status may prevent some of those interested in using mobile phones to send SMS as they may not have the credits. However, this may be less of an issue as an alternative paper-based form is planned.
CitationCrain et al. (2014) revealed that mobilizing, attracting and retaining participants in citizen science projects is a complex process as it relies on numerous cognitive, behavioural and social characteristics. Therefore, there is a need to consider these barriers and characteristics from the start of the design and implementation of every citizen science project. Addressing these barriers and having decision makers included and interested from the start of the design of the project may enable both short and long term participation of all stakeholders including volunteers. Therefore, these barriers and characteristics are considered in this integrated project in order to focus on the connection between heterogeneous human and vector behaviour. This paper is focusing on human behaviour while a companion paper focuses on malaria vector surveillance and environmental conditions (CitationMurindahabi et al., 2018).
6 Conclusion
By taking an integrative approach, our model of determinants of malaria prevention behaviour aims to enhance our understanding of the interrelationships between factors that influence individuals to participate in a citizen science platform and use malaria preventive measures. Our model of determinants of malaria prevention behaviour is the first to integrate the HBM, TPB, and UTAUT models into a synthesized research model for explaining behavioural intention to adopt a new innovation, in this case, malaria prevention measures and a citizen science platform. This model could be useful as a foundation for future interventions and research activities and will be tested in an application to support malaria prevention in Rwanda. The proposed conceptual framework describes linkages in malaria prevention models and this has implications in both academic and societal settings in relation to malaria prevention and control. Most of the proposed linkages between the concepts (social capital and individual perceptions, social capital and collective action, connective action and collective action, experiences and social capital, as well as experience and individual perceptions to mention few) are new to malaria prevention context. Consequently, this proposed model could be valid for behaviour research and other issues related to vector-borne or other infectious diseases. This model may serve as an important step in this field of research, be empirically tested and provide useful information for further research and academic debates from different countries. As shown it is initially important to consider antecedents including social capital and individual perceptions when designing a citizen science platform. Community mobilization is a key to get people interested in a citizen science project. Features of a citizen science platform to be conducted as an interdisciplinary project involving the collection of socio-ecological data also present a promising tool to complement the existing malaria prevention and control interventions implemented by NMCP in Rwanda.
Competing interests
The authors declare that they have no conflicting interests.
Acknowledgements
This publication is part of the project “Environmental Virtual Observatories for Connective Action (EVOCA)”, project duration 2016-2020, which is funded by Wageningen University, The Netherlands through its Interdisciplinary Research and Education Fund (INREF).
Related Research Data
References
- E. Aceves-Bueno A.S. Adeleye D. Bradley W. Tyler Brandt P. Callery M. Feraud Citizen science as an approach for overcoming insufficient monitoring and inadequate stakeholder buy-in in adaptive management: criteria and evidence Ecosystems 18 3 2015 493 506 https://doi.org/10.1007/s10021-015-9842-4
- Á.F. Agudo-Peregrina Á. Hernández-García F.J. Pascual-Miguel Behavioral intention, use behavior and the acceptance of electronic learning systems: differences between higher education and lifelong learning Comput. Hum. Behav. 34 2014 301 314 https://doi.org/10.1016/j.chb.2013.10.035
- A.S. Ahadzadeh S. Pahlevan Sharif F.S. Ong K.W. Khong Integrating health belief model and technology acceptance model: an investigation of health-related internet use J. Med. Internet Res. 17 2 2015 e45 https://doi.org/10.2196/jmir.3564
- S.M. Ahmed M.S. Hossain M. Kabir Conventional or interpersonal communication: which works best in disseminating malaria information in an endemic rural Bangladeshi community? PLoS One 9 6 2014e90711https://doi.org/10.1371/journal.pone.0090711
- I. Ajzen The theory of planned behavior Organ. Behav. Hum. Decis. Processes 50 1991 179 211
- A. Ankomah S.B. Adebayo E.D. Arogundade J. Anyanti E. Nwokolo O. Ladipo M.M. Meremikwu Determinants of insecticide-treated net ownership and utilization among pregnant women in Nigeria BMC Public Health 12 105 2012 https://doi.org/10.1186/1471-2458-12-105
- B. Asiimwe-Kateera J. Condo A. Ndagijimana S. Kumar M. Mukeshimana E. Gaju Analysis: Mobile health approaches to non-communicable diseases in Rwanda Rwanda J. Ser. F Med. Health Sci. 2 1 2015 89 92 https://doi.org/10.4314/rj.v2i1.13F
- H.E. Atieli G. Zhou Y. Afrane M.C. Lee I. Mwanzo A.K. Githeko G. Yan Insecticide-treated net (ITN) ownership, usage, and malaria transmission in the highlands of western Kenya Parasites Vectors 4 113 2011 https://doi.org/10.1186/1756-3305-4-113
- J.A. Atkinson A. Bobogare L. Fitzgerald L. Boaz B. Appleyard H. Toaliu A. Vallely A qualitative study on the acceptability and preference of three types of long-lasting insecticide-treated bed nets in Solomon Islands: implications for malaria elimination Malar. J. 8 119 2009 https://doi.org/10.1186/1475-2875-8-119
- J.A. Atkinson L. Fitzgerald H. Toaliu G. Taleo A. Tynan M. Whittaker Community participation for malaria elimination in Tafea Province, Vanuatu: Part I. Maintaining motivation for prevention practices in the context of disappearing disease Malar. J. 9 93 2010 https://doi.org/10.1186/1475-2875-9-93
- J.O. Bamidele M.I. Ntaji E.A. Oladele O.K. Bamimore Community participation in malaria control in olorunda local government Area, Osun State, Southwestern Nigeria Afr. J. Infect. Dis. 6 2 2012 24 28 https://doi.org/10.4314/ajid.v6i2.1
- N. Beer A.S. Ali H. Eskilsson A. Jansson F.M. Abdul-Kadir G. Rotllant-Estelrich A qualitative study on caretakers’ perceived need of bed-nets after reduced malaria transmission in Zanzibar, Tanzania BMC Public Health 12 606 2012 https://doi.org/10.1186/1471-2458-12-606
- W.L. Bennett A. Segerberg The logic of connective action Inf. Commun. Soc. 15 5 2012 739 768 https://doi.org/10.1080/1369118x.2012.670661
- A. Bennett S.J. Smith S. Yambasu A. Jambai W. Alemu A. Kabano T.P. Eisele Household Possession and use of insecticide-treated mosquito nets in Sierra Leone 6 months after a national mass-distribution campaign PLoS One 7 5 2012 e37927
- S. Berthe D. Loll S.L. Faye I. Wone H. Koenker B. Arnold R. Weber When I sleep under the net, nothing bothers me; I sleep well and I’m happy": Senegal’s culture of net use and how inconveniences to net use do not translate to net abandonment Malar. J. 13 357 2014 https://doi.org/10.1186/1475-2875-13-357
- Z. Birhanu L. Abebe M. Sudhakar G. Dissanayake Y. Yihdego G. Alemayehu D. Yewhalaw Access to and use gaps of insecticide-treated nets among communities in Jimma Zone, southwestern Ethiopia: baseline results from malaria education interventions BMC Public Health 15 1304 2015 https://doi.org/10.1186/s12889-015-2677-2
- G.S. Bloomfield R. Vedanthan L. Vasudevan A. Kithei M. Were E.J. Velazquez Mobile health for non-communicable diseases in Sub-Saharan Africa: a systematic review of the literature and strategic framework for research Global Health 10 49 2014 https://doi.org/10.1186/1744-8603-10-49
- R. Bonney T.B. Phillips H.L. Ballard J.W. Enck Can citizen science enhance public understanding of sciencA Public Underst. Sci. 25 1 2016 2 16 https://doi.org/10.1177/0963662515607406
- J.I. Campbell I. Aturinda E. Mwesigwa B. Burns D. Santorino J.E. Haberer The technology acceptance model for resource-limited settings (TAM-RLS): a novel framework for mobile health interventions targeted to low-literacy end-users in resource-limited settings AIDS Behav. 2017 https://doi.org/10.1007/s10461-017-1765-y
- V.L. Champion C.S. Skinner 4th ed. The Health Belief Model: Health Behaviour and Health Education: Theory, Research and Pracitce vol. 4 (2008) 45–65.
- J.M. Cohen D.L. Smith C. Cotter A. Ward G. Yamey O.J. Sabot B. Moonen Malaria resurgence: a systematic review and assessment of its causes Malar. J. 11 122 2012 https://doi.org/10.1186/1475-2875-11-122
- J.P. Cohn Citizen science: can volunteers Do Real research? BioScience 58 3 2008 192 197 https://doi.org/10.1641/b580303
- H. Cole-Lewis T. Kershaw Text messaging as a tool for behavior change in disease prevention and management Epidemiol. Rev. 32 1 2010 56 69 https://doi.org/10.1093/epirev/mxq004
- S.J. Coleman Social Capital in the creation of human Capital Am. J. Sociol. 94 1988 S95 S120
- R. Crain C. Cooper J.L. Dickinson Citizen science: a tool for integrating studies of human and natural systems Annu. Rev. Environ. Resour. 39 2014 641 665 https://doi.org/10.1146/annurev-environ-030713-154609
- A.W. Crall R. Jordan K. Holfelder G.J. Newman J. Graham D.M. Waller The impacts of an invasive species citizen science training program on participant attitudes, behavior, and science literacy Public Underst. Sci. 22 6 2012 745 764 https://doi.org/10.1177/0963662511434894
- M.-A. Créach G. Velut F. de Laval S. Briolant L. Aigle C. Marimoutou Factors associated with malaria chemoprophylaxis compliance among French service members deployed in Central African Republic Malar. J. 15 174 2016 https://doi.org/10.1186/s12936-016-1219-4
- F.D. Davis Perceived usefulness, perceived ease of use, and user acceptance of information technology MIS Q. Manag. Inf. Syst. Res. Center Univ. Minnesota 13 3 1989 319 340
- L.A. de Weger P.S. Hiemstra E. Op den Buysch A.J. van Vliet Spatiotemporal monitoring of allergic rhinitis symptoms in the Netherlands using citizen science Allergy 69 8 2014 1085 1091 https://doi.org/10.1111/all.12433
- L. Den Broeder J. Devilee H. Van Oers A.J. Schuit A. Wagemakers Citizen science for public health Health Promot. Int. 2016 https://doi.org/10.1093/heapro/daw086
- L. Den Broeder L. Lemmens S. Uysal K. Kauw J. Weekenborg M. Schönenberger Public health citizen science; perceived impacts on citizen scientists: a case study in a low-income neighbourhood in the Netherlands Citizen Sci. Theory Pract. 2 1 2017 1 17 https://doi.org/10.5334/cstp.89
- T. Dessewffy Z. Nagy Born in facebook: the refugee crisis and grassroots connective action in Hungary Int. J. Commun. 10 2016 2872 2894
- G.M. Diiro H.D. Affognon B.W. Muriithi S.K. Wanja C. Mbogo C. Mutero The role of gender on malaria preventive behaviour among rural households in Kenya Malar. J. 15 14 2016 https://doi.org/10.1186/s12936-015-1039-y
- P. DiMaggio E. Hargittai W.R. Neuman J.P. Robinson Social implications of the internet Annu. Rev. Sociol. 27 2001 307 336
- S.V. Dlamini C.-W. Liao Z.H. Dlamini J.S. Siphepho P.-C. Cheng T.-W. Chuang C.-K. Fan Knowledge of human social and behavioral factors essential for the success of community malaria control intervention programs: the case of Lomahasha in Swaziland J. Microbiol. Immunol. Infect. 50 2 2017 245 253 https://doi.org/10.1016/j.jmii.2015.05.003
- C.E. Dunn A. Le Mare C. Makungu Malaria risk behaviours, socio-cultural practices and rural livelihoods in southern Tanzania: implications for bednet usage Soc. Sci. Med. 72 3 2011 408 417 https://doi.org/10.1016/j.socscimed.2010.11.009
- T.P. Eisele D. Larsen R.W. Steketee Protective efficacy of interventions for preventing malaria mortality in children in Plasmodium falciparum endemic areas Int. J. Epidemiol. 39 Suppl. 1 2010 i88 i101 https://doi.org/10.1093/ije/dyq026
- K.C. Ernst M.H. Hayden H. Olsen J.L. Cavanaugh I. Ruberto M. Agawo S. Munga Comparing ownership and use of bed nets at two sites with differential malaria transmission in western Kenya Malar. J. 15 217 2016 https://doi.org/10.1186/s12936-016-1262-1
- K.C. Ernst S. Erly C. Adusei M.L. Bell D.K. Kessie A. Biritwum-Nyarko J. Ehiri Reported bed net ownership and use in social contacts is associated with uptake of bed nets for malaria prevention in pregnant women in Ghana Malar. J. 16 13 2017 https://doi.org/10.1186/s12936-016-1660-4
- B. Eskenazi L. Quiros-Alcala J.M. Lipsitt L.D. Wu P. Kruger T. Ntimbane mSpray: a mobile phone technology to improve malaria control efforts and monitor human exposure to malaria control pesticides in Limpopo, South Africa Environ. Int. 68 2014 219 226 https://doi.org/10.1016/j.envint.2014.03.003
- B.S. Fjeldsoe A.L. Marshall Y.D. Miller Behavior change interventions delivered by mobile telephone short-message service Am. J. Prev. Med. 36 2 2009 165 173 https://doi.org/10.1016/j.amepre.2008.09.040
- J.I. Forrest M. Wiens S. Kanters S. Nsanzimana R.T. Lester E.J. Mills Mobile health applications for HIV prevention and care in Africa Curr. Opin. HIV AIDS 10 6 2015 464 471 https://doi.org/10.1097/coh.0000000000000198
- M. Fujiie Y. Hayami M. Kikuchi The conditions of collective action for local commons management: the case of irrigation in the Philippines Agric. Econ. 33 2 2005 179 189 https://doi.org/10.1111/j.1574-0862.2005.00351.x
- K.T. Galvin N. Petford F. Ajose D. Davies An exploratory qualitative study on perceptions about mosquito bed nets in the Niger Delta: what are the barriers to sustained use? J. Multidiscip. Healthc. 4 2011 73 83 https://doi.org/10.2147/jmdh.s15917
- I. Garcia-Martí R. Zurita-Milla A. Swart K.C. van den Wijngaard A.J.H. van Vliet S. Bennema M. Harms Identifying environmental and human factors associated with tick bites using volunteered reports and frequent pattern mining Trans.GIS 21 2 2017 277 299 https://doi.org/10.1111/tgis.12211
- K.E. Giller C. Leeuwis J.A. Andersson W. Andriesse A. Brouwer P. Frost Competing claims on natural resources: what role for science? Ecol. Soc. 13 2 2008 34
- J.E. Gimnig P. Otieno V. Were D. Marwanga D. Abong’o R. Wiegand The effect of indoor residual spraying on the prevalence of malaria parasite infection, clinical malaria and anemia in an area of perennial transmission and moderate coverage of insecticide treated nets in Western Kenya PLoS One 11 1 2016e0145282https://doi.org/10.1371/journal.pone.0145282
- M.P. Graves M.J. Ngondi J. Hwang A. Getachew T. Gebre W.A. Mosher Factors associated with mosquito net use by individuals in households owning nets in Ethiopia Malar. J. 354 2011 10
- C. Gryseels S. Uk V. Sluydts L. Durnez P. Phoeuk S. Suon Factors influencing the use of topical repellents: implications for the effectiveness of malaria elimination strategies Sci. Rep. 5 16847 2015 https://doi.org/10.1038/srep16847
- S.I. Hay D.J. Rogers S.E. Randolph D.I. Stern J. Cox G.D. Shanks R.W. Snow Hot topic or hot air? Climate change and malaria resurgence in East African highlands Trends Parasitol. 18 12 2002 530 534
- B.K. Haywood A “Sense of Place” in public participation in scientific research Sci. Educ. 98 1 2013 64 83 https://doi.org/10.1002/sce.21087
- K. Honjo A. Satake N-player mosquito net game: individual and social rationality in the misuse of insecticide-treated nets J. Theor. Biol. 342 2014 39 46 https://doi.org/10.1016/j.jtbi.2013.11.001
- M.R. Hoque An empirical study of mHealth adoption in a developing country: the moderating effect of gender concern BMC Med. Inf. Decis. Mak. 16 51 2016 https://doi.org/10.1186/s12911-016-0289-0
- Y.M.G. Hounmanou M.S.S. Agonsanou V. Dougnon M.H.B. Vodougnon E.M. Achoh J. Mohammed E.D. Karimuribo The necessity of mobile phone technologies for public health surveillance in Benin Adv. Public Health 2016 https://doi.org/10.1155/2016/5692480
- M.C. Ingabire A. Rulisa L. Van Kempen C. Muvunyi C.J. Koenraadt M. Van Vugt Factors impeding the acceptability and use of malaria preventive measures: implications for malaria elimination in eastern Rwanda Malar. J. 14 136 2015 https://doi.org/10.1186/s12936-015-0659-6
- M.C. Ingabire E. Hakizimana F. Kateera A. Rulisa B. Van Den Borne I. Nieuwold Using an intervention mapping approach for planning, implementing and assessing a community-led project towards malaria elimination in the Eastern Province of Rwanda Malar. J. 15 594 2016 https://doi.org/10.1186/s12936-016-1645-3
- M.C. Ingabire F. Kateera E. Hakizimana A. Rulisa D.V.B. Borne C. Muvunyi Stakeholder engagement in community-based malaria studies in a defined setting in the Eastern Province, Rwanda Mediterr. J. Soc. Sci. 7 2 2016 188 196
- H. Iwashita G. Dida K. Futami G. Sonye S. Kaneko M. Horio Sleeping arrangement and house structure affect bed net use in villages along Lake Victoria Malar. J. 9 176 2010 https://doi.org/10.1186/1475-2875-9-176
- N.S. Joo B.T. Kim Mobile phone short message service messaging for behaviour modification in a community-based weight control programme in Korea J. Telemed. Telecare 13 8 2007 416 420 https://doi.org/10.1258/135763307783064331
- H. Kampen J.M. Medlock A.G. Vaux C.J. Koenraadt A.J. van Vliet F. Bartumeus Approaches to passive mosquito surveillance in the EU Parasites Vectors 8 9 2015 https://doi.org/10.1186/s13071-014-0604-5
- F. Kateera C.M. Ingabire E. Hakizimana A. Rulisa P. Karinda M.P. Grobusch Long-lasting insecticidal net source, ownership and use in the context of universal coverage: a household survey in eastern Rwanda Malar. J. 14 390 2015 https://doi.org/10.1186/s12936-015-0915-9
- M.R. Kaufman D. Rweyemamu H. Koenker J. Macha My children and I will no longer suffer from malaria”: a qualitative study of the acceptance and rejection of indoor residual spraying to prevent malaria in Tanzania Malar. J. 11 220 2012 https://doi.org/10.1186/1475-2875-11-220
- J. Kim H.-A. Park Development of a health information technology acceptance model using consumers’ health behavior intention J. Med. Internet Res. 14 5 2012 e133 https://doi.org/10.2196/jmir.2143
- I. Kleinschmidt C. Schwabe M. Shiva J.L. Segura V. Sima S.J. Mabunda M. Coleman Combining indoor residual spraying and insecticide-treated net interventions Am. J. Trop. Med. Hyg. 81 3 2009 519 524
- C. Kullenberg D. Kasperowski What is citizen science? – a scientometric meta-analysis PLoS One 11 1 2016e0147152https://doi.org/10.1371/journal.pone.0147152
- J.-W. Lee S. Mendlinger Perceived self-efficacy and its effect on online learning acceptance and student satisfaction J. Serv. Sci. Manag. 4 3 2011 243 252 https://doi.org/10.4236/jssm.2011.43029
- K.A. Lindblade D. Mwandama T. Mzilahowa L. Steinhardt J. Gimnig M. Shah A cohort study of the effectiveness of insecticide-treated bed nets to prevent malaria in an area of moderate pyrethroid resistance, Malawi Malar. J. 14 31 2015 https://doi.org/10.1186/s12936-015-0554-1
- K. Macintyre M. Littrell J. Keating B. Hamainza J. Miller T.P. Eisele Determinants of hanging and use of ITNs in the context of near universal coverage in Zambia Health Policy Plan. 27 4 2012 316 325 https://doi.org/10.1093/heapol/czr042
- P. Meankaew J. Kaewkungwal A. Khamsiriwatchara P. Khunthong P. Singhasivanon W. Satimai Application of mobile-technology for disease and treatment monitoring of malaria in the " Border Healthcare Programme" Malar. J. 9 237 2010 https://doi.org/10.1186/1475-2875-9-237
- C.M. Montgomery K. Munguambe R. Pool Group-based citizenship in the acceptance of indoor residual spraying (IRS) for malaria control in Mozambique Soc. Sci. Med. 70 10 2010 1648 1655 https://doi.org/10.1016/j.socscimed.2010.01.020
- T.D. Moon C.B. Hayes M. Blevins M.L. Lopez A.F. Green L. Gonzalez-Calvo Factors associated with the use of mosquito bed nets: results from two cross-sectional household surveys in Zambezia Province, Mozambique Malar. J. 15 196 2016 https://doi.org/10.1186/s12936-016-1250-5
- P. Mozumder A. Marathe Role of information and communication networks in malaria survival Malar. J. 6 136 2007 https://doi.org/10.1186/1475-2875-6-136
- D.K. Mukhopadhyay S.S. Basu D. Roy N. Das F. Akbar G.N. Sarkar Netting the malaria menace: distribution and utilization of long-lasting insecticidal net in a malaria endemic area in Bankura, West Bengal J. Vector Borne Dis. 53 1 2016 23 29
- K. Munguambe R. Pool C. Montgomery C. Bavo A. Nhacolo L. Fiosse What drives community adherence to indoor residual spraying (IRS) against malaria in Manhica district, rural Mozambique: a qualitative study Malar. J. 10 344 2011 https://doi.org/10.1186/1475-2875-10-344
- S. Munro S. Lewin T. Swart J. Volmink A review of health behaviour theories: how useful are these for developing interventions to promote long-term medication adherence for TB and HIV/AIDS? BioMed Central 7 104 2007 https://doi.org/10.1186/1471-2458-7-104
- E.E.H. Murhandarwati A. Fuad M.D.F. Nugraheni Sulistyawati M.A. Wijayanti B.S. Widartono T.-W. Chuang Early malaria resurgence in pre-elimination areas in Kokap Subdistrict, Kulon Progo, Indonesia Malar. J. 13 130 2014 https://doi.org/10.1186/1475-2875-13-130
- M.M. Murindahabi D. Asingizwe P.M. Poortvliet A.J.H. Van Vliet E. Hakizimana L. Mutesa A digital citizen science platform for malaria surveillance and control in Ruhuha: Community-based malaria mosquito surveillance approach NJAS-Wageningen J. Life Sci. 2018(this issue)
- H.A. Mwenesi Social science research in malaria prevention, management and control in the last two decades: an overview Acta Trop. 95 3 2005 292 297 https://doi.org/10.1016/j.actatropica.2005.06.004
- P.N. Ng’ang’a G. Jayasinghe V. Kimani J. Shililu C. Kabutha L. Kabuage Bed net use and associated factors in a rice farming community in Central Kenya Malar. J. 8 64 2009 https://doi.org/10.1186/1475-2875-8-64
- F. Ngabo J. Nguimfack F. Nwaigwe C. Mugeni D. Muhoza R.D. Wilson Designing and implementing an innovative SMS-based alert system (RapidSMS-MCH) to monitor pregnancy and reduce maternal and child deaths in Rwanda Pan Afr. Med. J. 31 2012 13
- O. Nov O. Arazy D. Anderson Dusting for science: motivation and participation of digital citizen science volunteers Paper Presented at the Iconference 2011
- A.A. Obala J.N. Mangeni A. Platt D. Aswa L. Abel J. Namae W. Prudhomme O’Meara What is threatening the effectiveness of insecticide-treated bednets? A case-control study of environmental, behavioral, and physical factors associated with prevention failure PLoS One 10 7 2015 e0132778
- J.L. Obermayer W.T. Riley O. Asif J. Jean-Mary College smoking cessation using cell phone text messaging J. Am. Coll. Health 53 2 2004 71 78
- O.F. Okumu E. Mbeyela G. Lingamba J. Moore J.A. Ntamatungiro R.D. Kavishe Comparative field evaluation of combinations of long-lasting insecticide treated nets and indoor residual spraying, relative to either method alone, for malaria prevention in an area where the main vector is Anopheles arabiensis Parasites Vectors 6 46 2013
- P. Oliver G. Marwell A theory of the critical mass. I. Interdependence, group heterogeneity, and the production of collective action AJS 91 3 1985 522 556
- S. Olsen S. Smith T. Oei J. Douglas Health belief model predicts adherence to CPAP before experience with CPAP Eur. Respir. J. 32 3 2008 710 717 https://doi.org/10.1183/09031936.00127507
- M. Olson The Logic of Collective Action: Public Goods and the Theory of Groups Book Review 1971 107 114
- C. Panter-Brick S.E. Clarke H. Lomas M. Pinder S.W. Lindsay Culturally compelling strategies for behaviour change: a social ecology model and case study in malaria prevention Soc. Sci. Med. 62 11 2006 2810 2825 https://doi.org/10.1016/j.socscimed.2005.10.009
- B. Pluess F.C. Tanser C. Lengeler B.L. Sharp Indoor residual spraying for preventing malaria Cochrane Database Syst. Rev. 4 2010CD006657https://doi.org/10.1002/14651858.CD006657.pub2
- President’s Malaria Initiative Rwanda Malaria Operational Plan FY 2015 2015
- President’s Malaria Initiative Rwanda Malaria Operational Plan FY 2016 2016
- President’s Malaria Initiative Rwanda Malaria Operational Plan FY 2017 2017
- R.D. Putnam Tuning in, tuning Out: the strange disappearance of social Capital in America Polical Sci. Politics 28 4 1995 664 683
- P. Ramos-Pinto Social Capital as a Capacity for Collective Action. Assessing Social Capital: Concept, Policy, Practice 2006
- G.D. Rickard N.R. Dudovitz D.M. Wong C.H. Jen D.R. Osborn E.H. Fernandez I.C. Donkor Closing the gap between insecticide treated net ownership and use for the prevention of malaria Prog. Commun. Health Partnersh. 5 2 2011 123 131 https://doi.org/10.1353/cpr.2011.0018
- E.E. Ricotta M. Boulay R. Ainslie S. Babalola M. Fotheringham H. Koenker M. Lynch The use of mediation analysis to assess the effects of a behaviour change communication strategy on bed net ideation and household universal coverage in Tanzania Malar. J. 14 15 2015 https://doi.org/10.1186/s12936-014-0531-0
- W.J.H. Rittel M.M. Webber Dilemmas in a general theory of planning Policy Sci. 4 2 1973 155 169 https://doi.org/10.1007/BF01405730
- J. Rose G. Fogarty Determinants of perceived usefulness and perceived ease of use in the technology acceptance model: senior consumers’ adoption of self-service banking technologies Acad. World Bus. Mark. Manag. Dev. 2 10 2006 122 129
- D. Rotman J. Preece J. Hammock K. Procita D. Hansen C. Parr Dynamic changes in motivation in collaborative citizen-science projects Paper Presented at the Conference on Computer Supported Cooperative Work 2012
- D. Rotman J. Hammock J. Preece D. Hansen C. Boston A. Bowser Y. He Motivations affecting initial and long-term participation in citizen science projects in Three countries Paper Presented at the in iconference 2014
- D. Rotman J. Hammock J.J. Preece C.L. Boston D.L. Hansen A. Bowser Y. He Does Motivation in Citizen Science Change With Time and Culture? 2014 229 232 https://doi.org/10.1145/2556420.2556492
- C.L. Russell A. Sallau E. Emukah P.M. Graves G.S. Noland J.M. Ngondi Determinants of bed net use in Southeast Nigeria following mass distribution of LLINs: implications for social behavior change interventions PLoS One 10 10 2015e0139447
- M. Setbon J. Raude Population response to the risk of vector-borne diseases: lessons learned from socio-behavioural research during large-scale outbreaks Emerg. Health Threats J. 2 2009 e6 https://doi.org/10.3134/ehtj.09.006
- L.C. Steinhardt A. Yeka S. Nasr R.E. Wiegand D. Rubahika A. Sserwanga The effect of indoor residual spraying on malaria and anemia in a high-transmission area of Northern Uganda Am. J. Trop. Med. Hyg. 88 5 2013 855 861 https://doi.org/10.4269/ajtmh.12-0747
- C.E. Strachan A. Nuwa D. Muhangi A.P. Okui M.E. Helinski J.K. Tibenderana What drives the consistent use of long-lasting insecticidal nets over time? A multi-method qualitative study in mid-western Uganda Malar. J. 15 1 2016 44 https://doi.org/10.1186/s12936-016-1101-4
- T. Teo Examining the influence of subjective norm and facilitating conditions on the intention to use technology among pre-service teachers: a structural equation modeling of an extended technology acceptance model Asia Pac. Educ. Rev. 11 2 2010 253 262 https://doi.org/10.1007/s12564-009-9066-4
- C.I. Tobin-West E.O. Asuquo Utilization of intermittent preventive treatment of malaria by pregnant women in Rivers State, Nigeria Int. J. Prevent. Med. 4 1 2013 63 71
- L.P. Toé O. Skovmand K.R. Dabiré A. Diabaté Y. Diallo T.R. Guiguemdé Decreased motivation in the use of insecticide-treated nets in a malaria endemic area in Burkina Faso Malar. J. 8 175 2009 https://doi.org/10.1186/1475-2875-8-175
- M.X. Tong A. Hansen S. Hanson-Easey S. Cameron J. Xiang Q. Liu Perceptions of malaria control and prevention in an era of climate change: a cross-sectional survey among CDC staff in China Malar. J. 16 136 2017 https://doi.org/10.1186/s12936-017-1790-3
- A.F. van Woezik L.M. Braakman-Jansen O. Kulyk L. Siemons J.E. van Gemert-Pijnen Tackling wicked problems in infection prevention and control: a guideline for co-creation with stakeholders Antimicrob. Resist. Infect. Control 5 20 2016 https://doi.org/10.1186/s13756-016-0119-2
- V. Venkatesh H. Bala Technology acceptance model 3 and a research agenda on interventions Decis. Sci. 39 2 2008 273 315
- V. Venkatesh F.D. Davis A theoretical extension of the technology acceptance model: four longitudinal field studies Manag. Sci. 46 2 2000 186 204 https://doi.org/10.1287/mnsc.46.2.186.11926
- V. Venkatesh M.G. Morris G.B. Davis F.D. Davis User acceptance of information technology: toward a unified View Manag. Inf. Syst. Q. 27 3 2003 425 478
- Y.-S. Wang H.-H. Lin P. Luarn Predicting consumer intention to use mobile service Inf. Syst. J. 16 2 2006 157 179 https://doi.org/10.1111/j.1365-2575.2006.00213.x
- N. Watanabe A. Kaneko S. Yamar G. Taleo T. Tanihata J.K. Lum A prescription for sustaining community engagement in malaria elimination on Aneityum Island, Vanuatu: an application of health empowerment theory Malar. J. 14 291 2015 https://doi.org/10.1186/s12936-015-0779-z
- J. Weidman D.E. Dickerson C.T. Koebel Prevention through design adoption readiness model (PtD ARM): an integrated conceptual model Work 52 2015 865 876
- WHO World Malaria Report 2016 World Health Organization Geneva, Switzerland
- M. Widmar C.J. Nagel D.Y. Ho P.W. Benziger N. Hennig Determining and addressing obstacles to the effective use of long-lasting insecticide-impregnated nets in rural Tanzania Malar. J. 8 315 2009 https://doi.org/10.1186/1475-2875-8-315
- K. Witte Putting the fear back into fear appeals: the extended parallel process model Commun. Monogr. 59 1992 329 349
- A.N. Wotodjo V. Richard S. Boyer S. Doucoure N. Diagne A. Touré-Baldé The implication of long-lasting insecticide-treated net use in the resurgence of malaria morbidity in a Senegal malaria endemic village in 2010–2011 Parasites Vectors 8 267 2015 https://doi.org/10.1186/s13071-015-0871-9
- J. Yasuoka M. Jimba R. Levins Application of loop analysis for evaluation of malaria control interventions Malar. J. 13 140 2014 https://doi.org/10.1186/1475-2875-13-140
- X. Zhang X. Han Y. Dang F. Meng X. Guo J. Lin User acceptance of mobile health services from users' perspectives: the role of self-efficacy and response-efficacy in technology acceptance Inf. Health Soc. Care 42 2 2016 194 206 https://doi.org/10.1080/17538157.2016.1200053
- G. Zhou Y.A. Afrane A.M. Vardo-Zalik H. Atieli D. Zhong P. Wamae Changing patterns of malaria epidemiology between 2002 and 2010 in Western Kenya: the fall and rise of malaria PLoS One 6 5 2011 e20318 https://doi.org/10.1371/journal.pone.0020318
- D. Zurovac A.O. Talisuna R.W. Snow Mobile phone text messaging: tool for malaria control in Africa PLOS Med. 9 2 2012e1001176