Abstract
Here we present a case series from a primate research facility. The index case, a 4-year-old pig-tailed macaque (Macaca nemestrina) experimentally infected with chimeric simian-human immunodeficiency virus (SHIV SF162 P4 ), developed weight loss and was euthanized. Based on necropsy results the animal was diagnosed with opportunistic atypical mycobacteriosis associated with simian AIDS (SAIDS). Subsequently, tissues from the index animal, as well as tissues and oral mucosal swabs from six SHIV-infected contacts, were analyzed using molecular methods and found to contain nucleic acid sequences characteristic of Mycobacterium tuberculosis complex (MTBC). These data suggest that existing protocols fail to reliably detect MTBC infection in laboratory primates used as experimental models.
Emerging Microbes & Infections (2012) 1, e30; doi:10.1038/emi.2012.31
Case series
In June 2010, a 4-year-old male pig-tailed macaque (Macaca nemestrina) that had been experimentally infected with chimeric simian-human immunodeficiency virus (SHIVSF162 P4) and had developed chronic diarrhea and weight loss of 14% of its body weight over a 5-month period was euthanized with a presumptive diagnosis of stage 3 simian AIDS (SAIDS). Over the previous months diagnostic work up revealed depletion of CD4 cells and hypoalbuminemia with consistently negative stool cultures and negative stool examinations for gastro-intestinal parasites. Thoraco-abdominal radiography and abdominal ultrasound 2 weeks prior to euthanasia were normal, with the exception of mild splenomegaly and a circular hyperechoic area visualized in the liver. All routine tuberculin skin testing (TST) performed via intradermal eyelid injection of 1500 units of mammalian old tuberculin (Synbiotics, USA) prior to SHIVSF162 P4 inoculation in March 2009 was negative. No other laboratory abnormalities were noted. On necropsy, numerous multifocal fibrous-encapsulated mesenteric lymph node granulomas ranging in size from millimeters to 2.0 cm in diameter were found. Other organ systems were grossly unremarkable. Histologic analysis revealed mild to extensive multifocal histiocytic infiltration of the jejunum, ileum, colon and cecum. Mesenteric granulomas consisted of fibrous walls surrounding necrotic debris. The liver contained microgranulomas with some giant cells. Although no acid-fast bacteria (AFB) were seen in the mesenteric node granulomas, large numbers of AFB were found in foamy macrophages in the small and large intestine, as well as in the liver, mesenteric, inguinal and axillary lymph nodes. Tissues were not sent for AFB culture. The pathologist’s final diagnosis was opportunistic atypical mycobacteriosis associated with SAIDS immunosuppression.
As atypical mycobacteriosis is not regarded as readily transmissible between primates, no quarantine measures were implemented among animals housed with the index case (animal A). However, recognizing that a primary hepatic case of Mycobacterium tuberculosis complex (MTBC) had been recently detected in a pig-tailed macaque in this same colony,Citation1 we requested oral swab samples from contact animals on the same study (animals B, C, D and E) that had been housed adjacent to animal A and who had intermittent grooming contact with animal A subsequent to their experimental infection with SHIV in March 2009. We have previously shown that MTBC DNA can be recovered from the mouths of free-ranging primates in areas where MTBC prevalence in humans is high.Citation2
In November and December 2010, animals B–E were euthanized at study’s end per experimental protocol. One of the animals, (animal B), was noted to have 10% weight loss over the preceding 6 months and had, as a result, been given nutritional supplementation. Other than weight loss, no signs or symptoms of disease were noted. Animals C, D and E did not exhibit significant weight loss or other clinical signs or symptoms of disease ().
On necropsy, gross pathology of animals B, C, D and E was essentially normal, but histological analysis revealed lymphohistiocytic, plasmacytic and eosinophilic gastro-entero-colitis with enteric villar blunting and fusion in all four animals. In addition, extensive colonic spirochetosis was found in colonic specimens of animals D and E (). At necropsy, swabs of the mouth, liver and lung tissue from animals A–E were provided for nucleic acid analysis.
Also, oral, liver and lung swabs obtained at necropsy from two additional M. nemestrina (animals F and G) that had been experimentally infected with SHIV, housed in the same room as the index animal and that were euthanized after developing diarrhea and weight loss were included in the polymerase chain reaction (PCR) analysis. Histological analysis of animal F’s tissues found plasmacytic and eosinophilic gastro-entero-colitis, lymphoid depletion and hemosiderin deposition in lamina propria of the small intestine. Histologic analysis of animal G’s tissues showed lymphohistiocytic, plasmacytic and eosinophilic gastro-entero-colitis and enterocolonic amyloidosis (). Staining and culture of tissue for AFB were not performed on animals B–G.
Table 1 History and pathology characteristics of seven pig-tailed macaques on a SHIV study where MTBC went undetected
IS6110, a nucleic acid sequence diagnostic for mycobacteria of the MTBC and not present in atypical mycobacteria, was amplified from tissue samples from all seven animals ().Citation3 For all seven IS6110 amplifications, nucleic acid sequences were identical to the target IS6110 sequence of NCBI reference sequence NC_000962.2 (Figure 1). Importantly, IS6110 was detected in oral swabs acquired from animals B, C, D and E while they were alive.
Comment
IS6110 is known to occur only in mycobacteria of the MTBC, a group of closely related bacteria that includes Mycobacterium tuberculosis, which infects a third of the world’s human population.Citation4 Atypical mycobacteria do not contain the IS6110 sequence.Citation3 Thus, the mycobacteria detected in this study are not atypical mycobacteria. It should be emphasized that, in order to prevent false positive results stemming from contamination, stringent anti-contamination protocols were followed and appropriate negative controls were performed (see footnote to ).
The MTBC has been implicated in epizootic infection of laboratory primates over the past decades.Citation2,Citation5 Primate research facilities have gone to significant lengths to create populations (known as specific pathogen-free, or SPF) that are free of mycobacteria and a select group of enzootic simian viruses.Citation6 SPF colonies are designed to protect laboratory workers from enzootic primate-borne pathogens and to ensure that results obtained using primate biomedical models are not confounded by the presence of known pathogenic agents. The results described here suggest that present protocols in place at primate facilities sometimes fail to detect MTBC infection. Our results do not establish the timing of these animals’ infections; both reactivation of latent infection and newly acquired MTBC infection could have occurred. Notwithstanding, all animals in this study were born in the United States; thus, infection occurred at a domestic primate facility.
These data raise several questions. First, what role, if any, did MTBC play in the wasting disease observed in four of the animals, three of which had diarrhea? Are the histologic findings of intestinal leukocytic infiltration present in all animals related to MTBC and/or SHIV? Does MTBC act as a cofactor in causing disease in SHIV-infected pig-tailed macaques in an analogous manner to the synergistic action of HIV and MTBC in humans? Are there other infectious agents (such as the colonic spirochetes detected in two animals) or noninfectious factors involved? Further research, employing prospective and/or experimental designs, is needed to shed light on these issues.
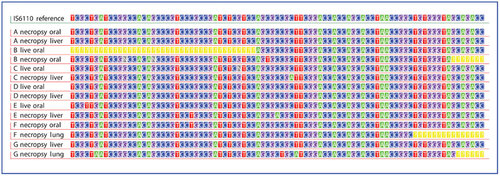
Table 1 IS6110 amplification of swabsFootnotea collected at live and/or necropsy time points from SHIV-infected pigtailed macaques
Second, how prevalent is MTBC infection in laboratory primate populations?Citation7 Are particular primate species or those that are on immunosuppressive studies at greater risk than others? Evidence shows that both within and among primate species variation in host response to infection with MTBC is much greater than previously understood.Citation8,Citation9,Citation10,Citation11 Additionally, functional differences in response to SIV or SHIV infection are also broad,Citation12,Citation13 and the host response to SIV influences the course of MTBC coinfection.Citation14 Currently, TST is used to screen for and diagnose infection with MTBC in laboratory primates.Citation5 TST relies on an animal's ability to mount an immune response. Because SHIV suppresses immune function by depleting the host's T lymphocytes, TST is not used to screen for mycobacterial infection in SHIV-infected laboratory animals. This is ironic and problematic, as infection with immunodeficiency viruses may increase macaques’ susceptibility to mycobacteria, as occurs in humans.Citation15 SHIV-infected macaques being used to model HIV are precisely those in whom detection of mycobacterial infection is most critical. Our findings reemphasize the importance of more rigorous protocols for the detection of MTBC in primate research laboratories.
Failure to reliably detect MTBC in laboratory primates raises a fundamental question about scientific experiments that use nonhuman primates as models of human pathophysiology. Could undetected infection with MTBC confound the results of research? Can we assume that the outcomes we observe in animals used to model host responses to a broad range of disease processes are governed by known independent variables, or is there another unknown, the presence of MTBC, which could interfere with the processes we are attempting to understand? After all, the nonhuman primate model is the raison d’etre of primate research facilities. It is this question that argues most strongly for the development of new protocols for the screening and diagnosis of MTBC in primate colonies. We agree with Sizemore and colleaguesCitation16 that ‘quickly and accurately identifying the presence of Mtb in… both latent and active TB is a critical first step to prevention of additional cases.’ The oral swab PCR used in this case series relies upon direct detection of the infectious agent rather than on a host immune response, and was able to identify the presence of MTBC DNA in four animals while they were still alive. Adoption of direct pathogen identification methods such as oral swab PCR could allow researchers the opportunity to monitor the presence of MTBC infections in their biomedical models. Further testing of this method in controlled trials is warranted in order to determine whether oral swab PCR can play a role in widespread screening and diagnosis for MTBC infection in the primate biomedical model.
The authors are grateful to Nicholas Lerche, DVM, MPVM who strongly believed that an interdisciplinary approach to infectious disease research was critical for a complete and nuanced understanding of our biomedical models and research outcomes. Shiu-Lok Hu, PhD provided useful discussions and critical reading of the manuscript. This research was supported by funding from NIH-NCRR grant P51 RR000166 and RR 02S014, NIH-NIAID grant R01 AI078229 and N66001-02-C-8072 DARPA.
- Stockinger DE, Roellich KM, Vogel KW et al. Primary hepatic Mycobacterium tuberculosis complex infection with terminal dissemination in a pig-tailed macaque (Macaca nemestrina). J Amer Assoc Lab Anim Sci2011; 50: 258–262.
- Wilbur A, Engel G, Rompis A et al. From the mouths of monkeys: Detection of Mycobacterium tuberculosis complex DNA from buccal swabs of synanthropic macaques. Am J Primatol2012; 74: 676–686.
- Eisenach KD. Use of an insertion sequence for laboratory diagnosis and epidemiologic studies of tuberculosis. Ann Emerg Med1994; 24: 450–453.
- WHO. Global tuberculosis control—epidemiology, strategy, financing.Geneva, World Health Organization.2009.
- Lerche NW, Yee JL, Capuano SV, Flynn JL. New approaches to tuberculosis surveillance in nonhuman primates. Inst Lab Anim Res J2008; 49: 170–178.
- Morton WR, Agy MB, Capuano SV, Grant RF. Specific pathogen-free macaques: definition, history, and current production. Inst Lab Anim Res J2008; 49: 137–144.
- Wilbur A, Engel GA, Jones-Engel L. TB infection in the nonhuman primate biomedical model: tip of the iceberg? Med Hypotheses2012; 79: 365–367.
- Lin P, Rodgers M, Smith L et al. Quantitative comparison of active and latent tuberculosis in the cynomolgus macaque model. Infect Immunol2009; 77: 4631–4642.
- Flynn JL, Capuano SV, Croix D et al. Non-human primates: a model for tuberculosis research. Tuberculosis2003; 83: 116–118.
- Mehra S, Golden NA, Dutta NK et al. Reactivation of latent tuberculosis in rhesus macaques by coinfection with simian immunodeficiency virus. J Med Primatol2011; 40: 233–243.
- Gormus B, Blanchard J, Alvarez X, Didier P. Evidence for a rhesus monkey model of asymptomatic tuberculosis. J Med Primatol2004; 33: 134–145.
- Smith M, Dale C, DeRose R et al. Analysis of pigtail macaque major histocompatibility complex class I molecules presenting immunodominant simian immunodeficiency virus epitopes. J Virol2005; 79: 684–695.
- Pratt BF, O’Connor DH, Lafont BA et al. MHC class I allele frequencies in pigtail macaques of diverse origin. Immunogenetics2006; 58: 995–1001.
- Shen Y, Zhou D, Chalifoux L et al. Induction of an AIDS virus-related tuberculosis-like disease in macaques: a model of simian immunodeficiency virus- mycobacterium coinfection. Infect Immunol2002; 70: 869–877.
- Pawlowski A, Jansson M, Sköld M, Rottenberg M, Källenius G. Tuberculosis and HIV Co-Infection. PLoS Pathogens2012; 8: e1002464.
- Sizemore CF, Schleif AC, Bernstein JB, Heilman CA. The role of biomedical research in global tuberculosis control: gaps and challenges. Emerg Microbes Infect2012; 1: e9.
- Inoue R, Tang WY, Wee SY, Barkham T. Evaluation of a real-time probe-based PCR assay with internal control for the direct detection of Mycobacterium tuberculosis complex. Eur J Clin Microbiol Infect Dis2011; 30: 131–135.
- Poinar H, Kuch M, Pääbo S. Molecular analyses of oral polio vaccine samples. Science2001; 292: 743–744.