

Abstract
Objectives: To explore age at death (AD) for major cardiovascular diseases (CVD) and their risk factors in originally middle-aged men followed nearly to extinction in the Seven Countries Study.
Materials and methods: Thirteen cohorts of men aged 40–59 years (N = 10,628) in seven countries (USA, Finland, the Netherlands, Italy, Serbia, Greece, Japan) were enrolled in late 1950s and early 1960s and were followed 45 years for mortality. AD was computed for coronary heart disease (CHD), stroke (STR), heart disease of uncertain aetiology (HDUE) and for all-causes. AD was compared across CHD-HDUE-STR. Cox models were computed for each end-point using baseline age, cigarettes smoking, systolic blood pressure and serum cholesterol.
Results: After 45 years 92.9% of men had died. The most common CVD death was CHD in most cohorts except some Mediterranean and Japanese cohorts where STR or HDUE were most prevalent. In 13 cohorts mean AD was 74.5, 73.5, 75.7 and 79.1 years, respectively, for all-cause, CHD, STR and HDUE mortality (all possible differences were significant). The difference, across cohorts, between the highest and the lowest mean AD was 12.9, 9.0 and 4.7 years for CHD, HDUE and STR mortality, respectively. Risk factors explored were significant predictors of all three CVD end-points, except serum cholesterol, specific to CHD mortality.
Conclusions: AD is a useful indicator of previous health and aging populations. STR and HDUE are diseases appearing later in life, thus being associated with a higher AD compared with CHD mortality.
Introduction
Age at death (AD) is a metric frequently used to describe fatal events related to rare diseases occurring in infants and children and for its estimation in forensic medicine. A larger and more comprehensive use of this metric is in demography and can be estimated in populations that (nearly) reached extinction. In this case, AD has advantages over death rates and life expectancy because it is unrelated to the entry age of the study population. AD is widely used in demography to describe mortality trends across populations [Citation1–4] but almost never used in classical field epidemiology. Population studies with a follow-up reaching the stage of extinction are rare. Classical examples are the British Doctors Study with participants enrolled in the 1950s and followed-up for 50 years in relation to smoking habits and fatal events [Citation5] and the Minnesota Business and Professional Men Study of Cardiovascular Diseases [Citation6].
In 13 cohorts of the Seven Countries Study (SCS) of Cardiovascular Diseases (CVD) baseline risk factor data and information on vital status and causes of death during 45 years of follow-up were collected. We explored AD for three major CVD endpoints as well as the strength of the association of four major risk factors with the same fatal conditions.
Materials and methods
Populations
Out of the original 16 cohorts of the Seven Countries Study, three: Dalmatia (former Yugoslavia), Slavonia (former Yugoslavia) and Rome railroad (Italy) discontinued the follow-up after 25 years while the other 13 reached at least 45 years of follow-up. Nine of the 13 cohorts were rural communities: East Finland and West Finland (Finland), Crevalcore and Montegiorgio (Italy), Velika Krsna (Serbia), Crete and Corfu (Greece), and Tanushimaru and Ushibuka (Japan). The other four cohorts were the US railroad, men from the town of Zutphen (The Netherlands), a cohort of workers in a large cooperative in Zrenjanin (Serbia) and a cohort of university professors in Belgrade (Serbia). A total of 10,628 men aged 40–59 years at baseline between 1958 and 1964 were examined and had high entry participation rates (94.8% on average). More details can be found elsewhere [Citation7–9].
Mortality
The 13 cohorts completed the follow-up for vital status and causes of death during the 45 years of follow-up. During that period of time, 53 men were lost to follow-up (5 per 1000) and were censored at defined dates.
Information on date of death and causes of death were systematically collected at regular intervals. Causes of death were coded following the 8th Revision of the WHO-ICD [Citation10] and were adjudicated by a single reviewer (AM) following pre-defined criteria. Additional descriptive information about each death was available to the reviewer in more than half of cases and was used in assigning final causes of death. In the presence of multiple causes of death and in case of serious doubts about the underlying cause of death, a hierarchical rank was adopted with violence, cancer, coronary heart disease (CHD), stroke and other causes in sequence.
Total CVD deaths were classified in five categories: coronary heart disease (CHD), stroke (STR), heart disease of uncertain aetiology (HDUE), peripheral arterial disease and other cardiovascular diseases. We focussed on CHD, STR and HDUE, disregarding the last two conditions because of small numbers.
CHD included only typical events characterised by myocardial infarction or sudden coronary deaths (when other causes could be reasonably excluded). Cases of heart disease presented only as heart failure, blocks or arrhythmias or defined as chronic CHD, were not coded as CHD but called HDUE for reasons explained elsewhere [Citation11,Citation12]. Fatal strokes (STR) were defined in a rough way since for the majority of cases it was impossible to segregate thrombotic from haemorrhagic events.
Risk factors
Four classical risk factors, common at baseline in all cohorts, were considered for multivariable analysis. They were (a) age in years at the closest birthday; (b) cigarette smoking classified as smokers and non-smokers; the latter contained both never and ex-smokers since preliminary tests showed that these two groups have similar predictive power during long-term follow-up; (c) systolic blood pressure in mmHg, measured in supine position using a mercury sphygmomanometer according to the method reported in the WHO Cardiovascular Survey Methods [Citation13]; the average of two consecutive measurements was used for analysis; (d) serum cholesterol in casual blood samples were determined with the Abell-Kendall method modified by Anderson and Keys [Citation14].
Baseline data were collected before the era of the Helsinki Declaration, with consent implied by participation in the examinations, while subsequently verbal or written consent was obtained to collect follow-up data.
Statistical analysis
For the purpose of this analysis, the 13 cohorts were individually considered as well as pooled. Prevalent CVD cases at baseline were not excluded because inclusion did not change the outcome of the analyses. Death rates per 1000 during 45 years for all-causes, CHD, STR and HDUE were computed for the 13 cohorts and their pool. Mean AD was computed for each end-point in each cohorts and their pool. Men still alive were censored at the end of the 45-year follow-up.
Mean AD for single end-points were compared across cohorts with ANOVA. Comparisons of the mean AD and the difference of AD among the three CVD end-points were performed by T test. Multivariable Cox proportional hazard models were computed for each CVD end-point including four covariates plus dummy variables identifying cohorts (the cohorts with highest death rate for each end-point were taken as reference: East Finland for CHD; Zrenjanin for STR and Velika Krsna for HDUE. This analysis was limited to 10,368 men due to missing data on risk factors for 260 men (2.4%). Proportionality of hazards was checked using the Schoenfeld residual plots that did not show any important trend. Coefficients of each risk factor were compared by T test for pairs of end-points (CHD versus STR, CHD versus HDUE; STR versus HDUE). This was done to identify possible differences in the predictive power of major risk factors of the three CVD end-points, taking into account their different mean AD.
Results
A total of 10,628 middle-aged men were examined at entry between 1958 and 1964 in 13 cohorts of the SCS. Total death rates over the 45-year follow-up period differed across cohorts, with highest levels (96.3%) in Zrenjanin (Serbia) and (96.1%) in Velika Krsna (Serbia) and the lowest (87.2%) in Crete (Greece) and (84.8%) Belgrade (Serbia) (). The total death rate was 92.9%, while CVD deaths comprised, on average, 50.7% of total deaths with large variations across cohorts. Overall, CHD, STR, and HDUE mortality represented 92.7% of total CVD deaths.
Table 1. All-causes and cardiovascular disease (CVD) mortality after 45-years of follow-up in 13 cohorts of the seven countries study.
AD: differences in individual CVD end-points across cohorts
The highest age for total death was 78.6 years in Crete (Greece) and the lowest 70.9 years in East Finland ().
Table 2. Mean age at death of all-causes, coronary heart disease (CHD), heart disease of uncertain aetiology (HDUE) and stroke (STR) after 45-years of follow-up in 13 cohorts of the seven countries study.
Even in individual CVD end-point there were large variations in different cohorts, as confirmed by the test of ANOVA. For example, for CHD there was a difference of more than 12 years between the highest (Crete in Greece) and the lowest AD (East Finland); in the case of HDUE the highest AD was found in Belgrade (Serbia), the lowest in Tanushimaru (Japan) with a difference of 9 years; and finally for STR, Corfu (Greece) had highest AD while Zrenjanin (Serbia) and Ushibuka (Japan) had the lowest with a 4.3-year difference. In general the rank of AD across cohorts was different for each of the three CVD end-points. The rank correlation coefficients of AD were of 0.42 between CHD and HDUE, 0.42 between CHD and STR and 0.63 between HDUE and STR.
AD between couples of end-points
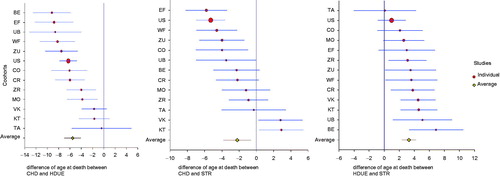
The mean age at total death for the 13 cohorts was 74.5 years for CHD, 79.1 for HDUE and 75.7 for STR. The difference between CHD and HDUE was −5.5 years, that for CHD versus STR was −2.2 years and that of HDUE versus STR was 3.3 years. All these differences were statistically significant ( and ). However, considering each cohorts, this picture was not always uniform since AD for CHD was significantly lower than that of HDUE in 8 cases out of 13; that of CHD was lower than that of STR in 6 cases; while AD for HDUE was significantly higher than that of STR in 8 cases. These results are illustrated in using forest plots.
Figure 1. Difference in age at death of CHD versus HDUE (−5.53 on average), CHD versus STR (−2.22 on average) and HDUE versus STR (3.28 on average).
AD of CVD events versus AD of all other causes of death
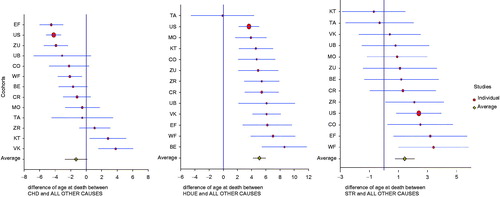
AD of individual CVD end-points versus AD of all causes (minus the one considered in each comparison) are reported in suggesting, overall, small but significant differences in all cases, with HDUE and STR having higher and CHD lower AD compared to that of all other causes of death. Again, not all comparisons, when considering individual cohorts, were statistically significant.
Figure 2. Difference in age at death of CHD versus OTHER CAUSES (−1.32 on average), HDUE versus OTHER CAUSES (5.08 on average) and STR versus OTHER CAUSES (1.43 on average).
Multivariable models
Cox proportional hazard models showed that age at baseline examination, cigarette smoking and systolic blood pressure were significantly associated with the three CVD end-points, while serum cholesterol was significantly related only to CHD mortality (). The strongest risk factor for all three CVD end-points was age at baseline examination. The strength of the association of smoking with CHD and HDUE mortality did not differ but was stronger for CHD than for STR mortality. The strength of the association of systolic blood pressure with CHD and HDUE mortality did not differ but was stronger for stroke compared to CHD and HDUE mortality. Serum cholesterol was only associated to CHD mortality.
Table 3. Cox proportional hazards models for three fatal cardiovascular end-points in 45 years, with four covariates in the seven countries study.
All the analyses described above were replicated for the 10 cohorts with 50 years of follow-up and showed similar results (not reported).
Discussion
The 45-year follow-up of 13 cohorts of the SCS showed that half of total deaths were due to total CVD deaths and the three major CVD end-points CHD, STR and HDUE represented up to 92.7% of all CVD deaths. The lowest mean AD was 73.5 years for CHD and was 2.2 years greater for STR and 5.5 years greater for HDUE mortality. The mean age of death between the extremes among the 13 cohorts differed by 12.9 years for CHD, 4.7 years for stroke and 9 years for HDUE mortality. The largest difference in AD in the pool of the cohorts was −5.5 years for CHD compared to HDUE mortality. The risk factors age at baseline examination, systolic blood pressure and smoking were strongly related to the three major CVD end-points and serum cholesterol was only associated with CHD mortality. These data also suggest some ‘ecological’ interpretations of AD although this would need an entirely different analysis and approach. We can only say that for CHD – the most common and best defined condition – AD was inversely related with overall mean baseline level of serum cholesterol, blood pressure and smoking habits.
The three CVD end-points studied here differ from a demographic perspective since age at CHD death is lower than age at total death, while STR and HDUE had a higher AD with the largest difference for CHD compared to HDUE mortality. Although the role of age at CHD death was particularly strong in areas with high death rates, the high AD of HDUE was the most relevant finding. This suggests that CHD, STR and HDUE are different diseases with specific pathologies and characterised by two common major risk factors: systolic blood pressure and smoking [Citation13]. Serum cholesterol is a major risk factor only for CHD but not for STR and HDUE. A competing risk analysis in the two Italian rural cohorts of the SCS confirmed that serum cholesterol was an important risk factor of CHD only, whereas a negative coefficient of this risk factor was found for competing diseases and in particular for HDUE [Citation15,Citation16]. We can hypothesise that if typical CHD will be partly prevented, it could be partly substituted by what we call HDUE. AD for STR was also smaller than that of HDUE while blood pressure had a greater coefficient for STR than for HDUE.
AD starting from middle-age is a valuable indicator of population health. The mean AD of the 13 SCS cohorts was 74.5 years and varied from 70.9 years in rural East Finland to 78.6 years in rural Crete (Greece). The mean age at CHD death was 73.5 years and ranged from 68.0 in East Finland and 80.9 in Crete. In the late 1950s and early 1960s when the SCS started, mean high serum cholesterol levels and a typical Northern European diet were associated with the lowest age at CHD and total deaths in East Finland compared to the highest in Crete, characterised by a lower mean serum cholesterol level and a traditional Mediterranean diet. [Citation7,Citation17,Citation18]. Although large changes in population serum cholesterol levels and partly dietary patterns occurred during the long-term follow-up, the characteristic differences in CHD and total mortality remained between Northern and Mediterranean Southern Europe.
During the decades of follow-up risk factor levels, although not systematically measured in all cohorts, showed changes usually characterised – at cohort level – by small declines in high-risk areas and increase in low-risk areas, latter particularly large in the Serbian areas. These changes allowed to explain part of the CHD mortality acceleration in some areas, and deceleration in others [Citation19–22]. These changes might impact on AD too, a hypothesis that needs an independent, complex and dedicated analysis.
HDUE is a mix of different conditions whose aetiology is not well-defined. In our material 21% was defined as ‘chronic CHD’ without clear evidence of typical CHD; 66% had heart failure (acute in about 1/5th of them); 10% had heart failure definitely linked to hypertension and 3% had chronic atrial arrhythmias or blocks. Our findings might be wrongly interpreted if a fatal heart failure following a typical CHD manifestation is considered the cause of death. This derives from the strict rules used in our epidemiological protocols in defining diagnoses and causes of death. If the clinical history of a subject includes typical CHD manifestations (myocardial infarction, acute ischaemic attacks and coronary death) CHD remains the cause of death and heart failure and other clinical manifestations appearing later are simply classified as consequences of CHD. On the other hand, cases of heart disease manifested only as heart failure (in the absence of the typical CHD syndromes) are never classified as CHD. Therefore, still allowing for some errors, cases classified as HDUE are most likely not due to gross coronary lesions and in any case they appear later in life.
Still, the most convincing evidence that CHD and HDUE are likely different diseases relies on old pathology contributions of the 1960s [Citation23,Citation24]. It was shown that large myocardial scars were accompanied by more or less advanced atherosclerotic lesions of large coronary vessels, while diffuse small fibro-sclerotic lesions of myocardium were unrelated to evident coronary atherosclerosis, suggesting the existence of a condition of undefined aetiology called ‘myocardial fibrosis’ [Citation25].
Findings on STR might be of uncertain interpretation since thrombotic cases could not be segregated from haemorrhagic cases, but altogether AD for STR showed intermediate levels between those of CHD and HDUE.
A limitation of this analysis was that findings were confined to a single gender – men – starting from their middle-age, a fact that surely could have neglected events occurred before that age range. Moreover, it was not possible to segregate thrombotic from haemorrhagic STR, the majority being classified in a generic way, due to the diagnostic limitations during the first decades after the start of the study. On the other hand, the strength of this analysis stays in the very long follow-up leaving the proportion of survivors to about 7% of the entry cohorts.
Outside demographic research, attention to AD is rare because it has probably little or no meaning if the study population did not reach extinction. Only a few cohort studies followed the participants until (nearly) extinction [Citation5,Citation6]. Analyses of epidemiologists, interested in cohorts followed until extinction, differ from those of demographers using official mortality statistics. In one of these studies, the mode of AD was used to investigate changes of mortality in low mortality countries and allowed new descriptions and interpretations of human longevity [Citation1]. In another contribution, variance in age at adult death was an important dimension of change in mortality. Risk factors, such as educational level and socio-economic status, were good indicators of the speed of the age pattern of mortality change [Citation2]. Frequently, the aging evolution studied in the past using aging rates led to wrong estimates that could be avoided using the shape of aging, a new metric for comparing aging trends [Citation3]. In general, the mode of AD was the best indicator of age increase in populations [Citation4].
In conclusion, AD computed in nearly extinct population samples allowed us to add another characteristic able to distinguish CHD from HDUE and STR and suggesting, once more, that these three conditions are different diseases, and that analyses based on their pool may distort the truth on some aspects of their characteristics.
Acknowledgements
The authors are grateful to Prof. David R Jacobs, University of Minnesota, Minneapolis, MN, USA, for reviewing the text and providing valuable advice.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Canudas-Romo V. The modal age at death and the shifting mortality hypothesis. Demog Res 2008;19:1179–1204.
- Tuljapurkar S. The final inequality variance in age at death. In: Shoven JB, editor. Demography and the economy, from the Natinal Bureau of Economic Research. Chicago: University of Chicago Press; 2010. p. 209–221.
- Wrycza TF, Missov TI, Baudisch A. Quantifying the shape of aging. PLoS One. 2015; 10:e0119163.
- Horiuchi S, Ouellette N, Cheung SLK, et al. Modal age at death: lifespan indicator in the era of longevity extension. Vienna Yearbook of Population Res. 2013; 2:37–69.
- Doll R, Peto R, Boreham J, et al. Mortality in relation to smoking: 50 years’ observations on male British doctors. Br Med J. 2004; 328:1519–1531.
- Tielemans SM, Geleijnse JM, Menotti A, et al. Ten-year blood pressure trajectories, cardiovascular mortalty and life years lost in two extinction cohorts: the Minnesota Business and Professional Men and the Zutphen Study. J Am Heart Assoc. 2015;4:001378.
- Keys A, Blackburn H, Menotti A. Coronary heart disease in seven countries. Circulation. 1970;41(Suppl 1):1–211.
- Keys A, Aravanis C, Blackburn H, et al. Seven countries study. A multivariate analysis of death and coronary heart disease. Cambridge (MA): Harvard Univ Press; 1980. p. 1–381.
- Kromhout D, Menotti A, Blackburn H. Prevention of Coronary Heart Disease. Diet, Lifestyle and Risk Factors in the Seven Countries Study. Norwell (MA): Kluwer Publ; 2002. p. 1–267.
- World Health Organization. International Classification of Diseases. 8th Rev ed. Geneva: World Health Organization; 1975.
- Menotti A, Puddu PE, Lanti M, et al. Epidemiology of typical coronary heart disease versus heart disease of uncertain etiology (atypical) fatalities and their relationships with classic coronary risk factors. Int J Cardiol. 2013;168:3963–3967.
- Puddu PE, Terradura Vagnarelli O, Mancini M, et al. Typical and atypical coronary heart disease deaths and their different relationships with risk factors. The Gubbio residential cohort Study. Int J Cardiol. 2014;173:300–304.
- Rose G, Blackburn H. Cardiovascular Survey Methods. Geneva: World Health Organization; 1968.
- Anderson JT, Keys A. Cholesterol in serum and lipoprotein fractions; its measurement and stability. Clin Chem. 1956; 2:145–159.
- Puddu PE, Piras P, Menotti A. Competing risks and lifetime coronary heart disease incidence during 50 years of follow-up. Int J Cardiol. 2016; 219:79–83.
- Puddu PE, Piras P, Menotti A. Lifetime competing risks between coronary heart disease mortality and other causes of death during 50 years of follow-up. Int J Cardiol. 2017;228:359–363.
- Menotti A, Puddu PE, Adachi H, et al. The strength of the multivariable associations of major risk factors predicting coronary heart disease mortality is homogeneous across different areas of the Seven Countries Study during 50-year follow-up. Acta Cardiol. 2017; [Aug 8]; [7 p.]. DOI:10.1080/00015385.2017.1351249
- Menotti A, Kromhout D, Puddu PE, et al. Baseline fatty acids, food groups, a diet score and 50-year all-cause mortality rates. An ecological analysis of the Seven Countries Study. Ann Med. 2017;49:718–727.
- Menotti A, Blackburn H, Kromhout D, et al. Changes in population cholesterol levels and coronary heart disease deaths in seven countries. Eur Heart J. 1997; 18:566–571.
- Menotti A, Lanti M, Kafatos A, et al. The role of a baseline casual blood pressure measurement and of blood pressure changes in middle age in prediction of cardiovascular and all-cause mortality occurring late in life: a cross-cultural comparison among the European cohorts of the Seven Countries Sudy. J Hypertens. 2004;22:1683–1690.
- Lanti M, Menotti A, Nedeljkovic S, et al. Long-term trends in major cardiovascular risk factors in cohorts of aging men in the European cohorts of the Seven Countries Study. Aging Clin Exp Res. 2005; 17:306–315.
- Menotti A, Lanti M, Kromhout D, et al. Forty-year coronary mortality trends and changes in major risk factors in the first 10 years of follow-up in the seven countries study. Eur J Epidemiol. 2007;22:747–754.
- Schwartz CJ, Mitchell JR. The relation between myocardial lesions and coronary artery disease. i. An unselected necropsy study. Br Heart J. 1962;24:761–786.
- Mitchell JR, Schwartz CJ. The relation between myocardial lesions and coronary artery disease ii. A selected group of patients with massive cardiac necrosis or scarring. Br Heart J. 1963;25:1–24.
- Anonimous. Myocardial fibrosis. Br Med J. 1963; 1:1304.

