

Abstract
Aims
Previous studies have found that excessive sport activities are associated with an increased risk of atrial fibrillation (AF). Whether occupational physical activity (OPA) increases the risk for AF is not well studied. We aimed to examine whether OPA influences the risk of AF.
Methods
80,922 men and women, free from AF, completed in 1997 a questionnaire about their OPA at that time (baseline), and also retrospectively in 1997 their OPA at the age of 30 and 50 years. Participants were categorised into three groups (low, medium and high) based on OPA load. Participants were followed-up in the Swedish National Patient Register for ascertainment of AF. Cox proportional hazards regression models were used to estimate relative risks (RR) with 95% confidence intervals (CI), adjusted for potential confounders.
Results
11,614 cases of AF were diagnosed during follow-up time of up to 17 years. We observed an increased risk of AF in relation to increased load of OPA regardless of age. Compared with men who reported a low load of OPA, the multivariable RR (95% CI) for men with a high load was 1.10 (1.03–1.17) at 30 years, 1.11 (1.04–1.17) at 50 years and 1.19 (1.10–1.29) at baseline. The results for women were similar with multivariable RR of 1.16 (1.06–1.27) at 30 years, 1.14 (1.05–1.24) at 50 years and 1.11 (0.99–1.24) at baseline.
Conclusion
These findings suggest that high load of OPA previous in life may play a role in increasing the risk for AF in both men and women.
Introduction
Atrial fibrillation (AF) is the most prevalent cardiac rhythm disorder of clinical significance and the prevalence of AF is estimated in recent studies to be around 3% among adults age 20 years or older [Citation1–3]. The incidence of AF is expected to rise because of an aging population and increasing occurrence of conditions predisposing AF [Citation4].
There is growing evidence that extensive and long-term endurance exercise may increase the risk for AF, especially in men [Citation5–8]. On the other hand, light-to-moderate intensity physical activity may be protective against AF [Citation7,Citation9]. Most previous studies investigated athletes or physical activity during leisure time. To our knowledge, only two studies have examined whether occupational physical activity (OPA) is associated with risk of AF, and results from those studies were divergent [Citation10,Citation11]. In the Copenhagen City Heart Study, a prospective cohort study of 17,196 men and women, participants who reported very high and high volume of OPA had significantly higher risk of AF compared with those who reported moderate volume of OPA [Citation11]. However, physical strain during working hours was not associated with AF among 19,593 men and 18,807 women in the Danish Diet, Cancer, and Health Study [Citation10]. Here we evaluated the association between occupational physical activity and incidence of AF in cohorts of Swedish adults. We hypothesised that high load of OPA increases the risk for AF.
Methods
Study population
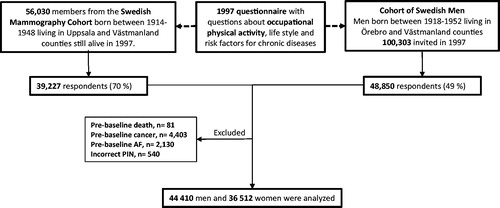
The study population is based on data from two prospective cohort studies of Swedish men (Cohort of Swedish Men) and women (Swedish Mammography Cohort), both of which are part of the national research infrastructure SIMPLER. During 1997, 48,850 out of 100,303 men (born 1918–1952) and 39,227 out of 56,030 women (born 1914–1948) from three Swedish counties completed a questionnaire about lifestyle and other risk factors for chronic diseases. For this analysis we excluded men and women with an erroneous or a missing personal identification number, those with a prior diagnosis of AF or cancer except non-melanoma skin cancer, and those who died between the administration of the questionnaire and start of follow-up. This left 44,410 men, 45–79 years of age, and 36,512 women, 49–83 years of age, for the present analysis (). Furthermore, we excluded men and women with missing data on occupational physical activity for each age category analysed. This left 42,662 men at 30 years of age, 36,628 men at 50 years of age, 37,950 men at baseline (mean age 60), 32,363 women at 30 years of age, 32,015 at 50 years of age, 31,922 at baseline (mean age 62) for the final analysis. The study was approved by the Regional Ethical Review Board in Stockholm, Sweden.
Figure 1. Source population, exclusions and study population.
Assessment of occupational physical activity and other covariates
At baseline (1997), participants completed a questionnaire where they reported OPA during work or occupation in six predefined categories (mostly sitting down; sitting down half the time; mostly standing up; mostly walking, minimum lifting/carrying; mostly walking, significant lifting/carrying; heavy manual labour) throughout their lifetime (at 15, 30 and 50 years of age, and at baseline in 1997). OPA at 15, 30 and 50 years of age were reported retrospectively at baseline in 1997. The validity of the assessment of the occupational physical activity through the questionnaire used in this cohort was tested in 111 men, aged 44–78 years, from the study area, by comparison with two seven-day activity records performed 6 months apart [Citation12]. The Spearman correlation coefficients (adjusted for within-person and between-person variations in the records) between the questionnaire and activity records were 0.4 for occupational physical activity. Information about, alcohol consumption, educational attainment, smoking status and history, weight, height, physical activity, history of hypertension and diabetes, and family history of myocardial infarction was collected in the same questionnaire. Participants were classified as having hypertension or diabetes if they reported that they had these diseases or if they had a diagnosis of these diseases in the Swedish National Patient Register (NPR) or the Swedish National Diabetes Register. Cardiac disease was defined as a diagnosis of ischaemic heart disease, heart failure in the Swedish NPR.
Case ascertainment and follow-up
Cases of AF were ascertained through linkage with the Swedish NPR (using the unique personal identity number assigned to each Swedish resident) and classified according to the International Classification of Diseases (ICD). Cases of AF and atrial flutter were identified using the code I48 from ICD-10. The outcome of AF was defined as either a diagnosis of AF or flutter because of their similarity and close interrelationship. The validity of a diagnosis of AF in the Swedish NPR is high with a positive predictive value of 97% [Citation13].
Dates of death were obtained from the Swedish Death Register. Person-time of follow-up was calculated from 1 January 1998 until the date of diagnosis of AF, death, or 31 December 2014, whichever came first.
Statistical analysis
In the primary analyses, participants were categorised into three groups (low, medium and high) depending on their self-reported occupational physical activity level (Low = mostly sitting down or sitting down about half the time; High = mostly walking with significant lifting/carrying or heavy labour). We analysed women and men separately. Cox proportional hazards regression models with age as the time variable was used to estimate relative risks (RR) with 95% confidence intervals (CI). Multivariable models were adjusted for age (as the time scale), education (less than high school; high school; university), smoking status and history (never, past smoker and <20 pack-years, past smoker and ≥20 pack-years, current smoker and <20 pack-years, or current smoker and ≥20 pack-years), body mass index (kg/m2, continuous), walking or bicycling (almost never, <20 min/day, 20 – 40 min/day, 40 – 60 min/day, or >1 h/day), history of cardiac disease (yes or no), hypertension (yes or no), and diabetes (yes or no), family history of myocardial infarction before age 60 (yes or no), and alcohol consumption (nondrinkers; and <1, 1–6, 7–13, 14–20, and ≥21 drinks/week). Further adjustment for leisure-time exercise at baseline, at age 50, or at age 30 years did not change the results. We therefore did not include leisure-time exercise in the final multivariable model. All statistical analyses were conducted using SAS (version 9.5, SAS Institute, Cary, NC). All statistical tests were two-sided, and p values <.05 were considered statistically significant.
Results
Baseline characteristics for the study population divided by sex and category of OPA level (low, medium, high) are shown in . Compared with high OPA, those with low OPA level had significant higher proportion of post-secondary education, less likely to be current smokers but had a higher proportion of other cardiovascular risk factors such as higher prevalence of diabetes mellitus, hypertension and previous cardiovascular disease.
Table 1. Age-standardized baseline characteristics of participants of the Cohort of Swedish Men and the Swedish Mammography Cohort by categories of work/occupational physical activity at baseline.
Over a median follow-up of 17 years, AF developed in 6917 men and in 4697 women. The associations of OPA with risk of AF in men and women, are presented in . In both men and women, the risk of AF increased with increasing level of OPA in all age groups. Men who reported a high level of OPA at age 30, age 50 and at baseline (mean age 60) had a RR 1.10 (95% CI 1.03 to 1.17), 1.11 (95% CI 1.04 to 1.17) and 1.19 (95% CI 1.10 to 1.29) compared with men who reported a low OPA (). Similar results were observed among women. Women who reported a high level of OPA at age 30, age 50 and at baseline (mean age 62) had a positive association of AF compared with women who reported a low level of OPA, the RR was 1.16 (95% CI 1.06 to 1.27), 1.14 (95% CI 1.05 to 1.24), and 1.11 (95% CI 0.99 to 1.11), across age groups. The association did not reach statistical significance at baseline (mean age 62).
Table 2. Relative risk (95% confidence interval) of atrial fibrillation by categories of work/occupational physical activity at different ages in the Cohort of Swedish Men and the Swedish Mammography Cohort, 1998–2014.
Discussion
In this population-based cohort study we observed an association between OPA and AF. The risk of AF increased with increasing level of OPA in all age groups in both men and women. This finding is consistent with the results by Skielboe and co-workers who also found a positive association between high volume of occupational physical activity and the risk of AF in the Copenhagen City Heart Study [Citation11]. In that study, the HRs were 1.39 (95% CI 1.03 to 1.88) for very high volume OPA and 1.21 (95% CI 1.02 to 1.43) for high volume OPA, compared with moderate volume of OPA [Citation11]. The high level of exposure of OPA in the highest category in the Copenhagen City Heart Study may explain the somewhat stronger association observed in that study compared with our study. The highest category of OPA in the Copenhagen City Heart Study was heavy manual work exemplified as lumberjack, dock worker, stone mason, farm worker and ditch digger [Citation11,Citation14]. Because of the large sample size, especially the large number of AF cases (6917 AF cases in men and in 4697 cases in women), we had high statistical power and could also detect weak associations. The lack of association between OPA and AF in the Danish Diet, Cancer, and Health Study [Citation10] might be related to a short follow up time (mean follow up time 5.7 years) and limited number of cases (n = 418) and therefore limited statistical power.
Other work-related factors such as long working hours and work related psychosocial stress has been found to be associated with increased risk of AF [Citation15,Citation16]. We did not have any information on working hours or psychosocial stress and were not able to adjust for these factors.
Several studies have studied the association between leisure-time exercise and the risk of AF and current evidence is that there is a positive association between high volume of endurance exercise and AF in men, but the effects of exercise in women still remain controversial [Citation5–7,Citation17]. No studies have been able to show that leisure-time exercise increase the risk for AF in women [Citation17–22]. A positive association between high volumes of exercise and AF has been consistently detected in studies of middle-aged men but the association has not been shown when older individuals have been studied. In this study on occupational physical activity and AF risk we observed a positive association in both men and women in all age groups. The exact pathophysiological mechanism by which frequent high-intensity exercise increase the risk for AF is likely multifactorial. Increased hemodynamic load, exercise hypertension, inflammatory and oxidative stress could cause atrial structural remodelling with atrial enlargement and atrial fibrosis. These structural changes in the atria favours re-entry mechanisms and perpetuation of AF [Citation4,Citation23]. Increase in parasympathetic tone is one of the most commonly cited mechanism for exercised induced AF. The autonomous nervous system has a role in both triggering paroxysmal AF and in maintaining persistent AF [Citation24]. It is mainly endurance exercise that has been associated with increased risk of AF and high levels of occupational physical activity involves much more static resistance strain such as lifting/carrying which may suggest somewhat different pathophysiological mechanism in the development of AF. High load of OPA with more lifting and carrying have been associated with higher systolic blood pressure compared to low load of OPA. Leisure-time exercise is more dynamic physical activity and is not correlated with higher systolic blood pressure [Citation25]. This could be one of the pathophysiological mechanisms for development of AF in high load of OPA.
Strengths of this study include the prospective design, the large sample size, the large number of incident cases of AF and the almost complete follow up due to computerised linkage to the nationwide registry with high validity of AF diagnosis. There are several limitations in this study. The exposure of occupational physical activity was collected through a self-administered questionnaire, which could lead to some exposure misclassification, which most likely is random and would attenuate rather than exaggerate any true relationships. A further limitation is the observational design. Despite adjustment for several major risk factors for AF, residual confounding cannot be entirely ruled out as an explanation for the observed findings.
In conclusion, our findings together with those of previous cohort studies indicate that high load of occupational physical activity is associated with an increased risk of AF in both men and women.
Author contributions
ND and SCL designed the study. SCL and AW obtained the data. ND, AW and SCL interpreted the data. ND wrote the report. ND, AW and SCL critically revised the report. SCL did the statistical analysis. All authors approved the final report submission.
Ethics approval
The Regional Ethical Review Board in Stockholm, Sweden, approved this study.
Acknowledgments
The authors acknowledge the national research infrastructure SIMPLER (the Swedish Infrastructure for Medical Population-based Life-course and Environmental Research) for provisioning of facilities and support.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Haim M, Hoshen M, Reges O, et al. Prospective national study of the prevalence, incidence, management and outcome of a large contemporary cohort of patients with incident non-valvular atrial fibrillation. J Am Heart Assoc. 2015;4(1):e001486.
- Friberg L, Bergfeldt L. Atrial fibrillation prevalence revisited. J Intern Med. 2013;274(5):461–468.
- Chugh SS, Havmoeller R, Narayanan K, et al. Worldwide epidemiology of atrial fibrillation: a Global Burden of Disease 2010 Study. Circulation. 2014;129(8):837–847.
- Kirchhof P, ESC Scientific Document Group, Benussi S, Kotecha D, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016;37(38):2893–2962.
- Karjalainen J, Kujala UM, Kaprio J, et al. Lone atrial fibrillation in vigorously exercising middle aged men: case-control study. BMJ. 1998;316(7147):1784–1785.
- Aizer A, Gaziano JM, Cook NR, et al. Relation of vigorous exercise to risk of atrial fibrillation. Am J Cardiol. 2009;103(11):1572–1577.
- Drca N, Wolk A, Jensen-Urstad M, et al. Atrial fibrillation is associated with different levels of physical activity levels at different ages in men. Heart. 2014;100(13):1037–1042.
- Mont L, Sambola A, Brugada J, et al. Long-lasting sport practice and lone atrial fibrillation. Eur Heart J. 2002;23(6):477–482.
- Mozaffarian D, Furberg CD, Psaty BM, et al. Physical activity and incidence of atrial fibrillation in older adults: the cardiovascular health study. Circulation. 2008;118(8):800–807.
- Frost L, Frost P, Vestergaard P. Work related physical activity and risk of a hospital discharge diagnosis of atrial fibrillation or flutter: the Danish Diet, Cancer, and Health Study. Occup Environ Med. 2005;62(1):49–53.
- Skielboe AK, Marott JL, Dixen U, et al. Occupational physical activity, but not leisure-time physical activity increases the risk of atrial fibrillation: The Copenhagen City Heart Study. Eur J Prev Cardiol. 2016;23(17):1883–1893.
- Norman A, Bellocco R, Bergstrom A, et al. Validity and reproducibility of self-reported total physical activity-differences by relative weight. Int J Obes Relat Metab Disord. 2001;25(5):682–688.
- Smith JG, Platonov PG, Hedblad B, et al. Atrial fibrillation in the Malmö Diet and Cancer study: a study of occurrence, risk factors and diagnostic validity. Eur J Epidemiol. 2010;25(2):95–102.
- Saltin B, Grimby G. Physiological analysis of middle-aged and old former athletes. Comparison with still active athletes of the same ages. Circulation. 1968;38(6):1104–1115.
- Toren K, Schioler L, Soderberg M, et al. The association between job strain and atrial fibrillation in Swedish men. Occup Environ Med. 2015;72(3):177–180.
- Kivimaki M, IPD-Work consortium, Nyberg ST, Batty GD, et al. Long working hours as a risk factor for atrial fibrillation: a multi-cohort study. Eur Heart J. 2017;38(34):2621–2628.
- Andersen K, Farahmand B, Ahlbom A, et al. Risk of arrhythmias in 52 755 long-distance cross-country skiers: a cohort study. Eur Heart J. 2013;34(47):3624–3631.
- Drca N, Wolk A, Jensen-Urstad M, et al. Physical activity is associated with a reduced risk of atrial fibrillation in middle-aged and elderly women. Heart. 2015;101(20):1627–1630.
- Myrstad M, Aarønaes M, Graff-Iversen S, et al. Does endurance exercise cause atrial fibrillation in women? Int J Cardiol. 2015;184:431–432.
- Everett BM, Conen D, Buring JE, et al. Physical activity and the risk of incident atrial fibrillation in women. Circ Cardiovasc Qual Outcomes. 2011;4(3):321–327.
- Azarbal F, Stefanick ML, Salmoirago-Blotcher E, et al. Obesity, physical activity, and their interaction in incident atrial fibrillation in postmenopausal women. JAHA. 2014;3(4):e001127. Published 2014 Aug 20. doi:https://doi.org/10.1161/JAHA.114.001127
- Thelle DS, Selmer R, Gjesdal K, et al. Resting heart rate and physical activity as risk factors for lone atrial fibrillation: a prospective study of 309,540 men and women. Heart. 2013;99(23):1755–1760.
- Guasch E, Benito B, Qi X, et al. Atrial fibrillation promotion by endurance exercise: demonstration and mechanistic exploration in an animal model. J Am Coll Cardiol. 2013;62(1):68–77.
- Shen MJ, Choi EK, Tan AY, et al. Neural mechanisms of atrial arrhythmias. Nat Rev Cardiol. 2011;9(1):30–39.
- Clays E, De Bacquer D, Van Herck K, et al. Occupational and leisure time physical activity in contrasting relation to ambulatory blood pressure. BMC Public Health. 2012;12:1002.

