

Abstract
Background and purpose
Hypertension is common in patients with atrial fibrillation (AF) and carries an additional risk for complications, most notably stroke and bleeding. We assessed the history of hypertension, level of blood pressure control, and an interaction with the choice of oral anticoagulants on clinical outcomes
Methods
We performed a systematic review and meta-analysis of studies that randomised patients to novel oral anticoagulants (NOACs) or vitamin K antagonists (VKAs) and reported outcomes stratified by presence of hypertension. Collected outcomes were: ischaemic stroke or systemic embolism (SE), haemorrhagic stroke, intracranial haemorrhage and major bleeding. Log adjusted hazard ratios (HR) and corresponding standard error were calculated, and HRs were compared using Mantel-Haenszel random effects. Quality of the evidence was assessed with Cochrane risk of bias tool.
Results
Five high-quality studies were eligible, including 71.527 participants who received NOACs (apixaban, dabigatran, edoxaban, rivaroxaban) or VKAs, with median follow-up of 1.8–2.8 years. Compared with patients without hypertension, those with hypertension had higher adjusted risk for ischaemic stroke/SE (HR: 1.25, 95%-CI:1.09, 1.43) and haemorrhagic stroke (HR:1.98, 1.24–3.16). On a continuous scale, the risk of ischaemic stroke/SE increased 6–7% per 10 mmHg increase in systolic blood pressure. No interactions were found between the efficacy or safety of NOACs versus VKAs in the presence or absence of hypertension. In both groups, the use of NOACs led to a lower risk of ischaemic stroke/SE, haemorrhagic stroke and intracranial haemorrhage compared with patients that used VKAs.
Conclusions
Adequate blood pressure management is vital to optimally reduce the risk of stroke in patients with atrial fibrillation. The benefits of NOACs over VKAs, also apply to patients with elevated blood pressure.
Introduction
Atrial fibrillation is the most common sustained cardiac arrhythmia, with a lifetime prevalence of about one in four [Citation1]. Elevated blood pressure is an important risk factor for developing AF, with most studies showing a direct and linear relation between blood pressure levels and the risk of AF [Citation2]. Prior studies show that hypertension is the most frequent comorbidity in patients with AF, with prevalence values ranging from 49–90% [Citation2,Citation3]. Moreover, in patients with AF, hypertension exerts a multiplicative effect on the risk of experiencing stroke and bleeding events [Citation2,Citation3]. As such, achieving blood pressure targets as well as adequate antithrombotic treatment are critical to reduce the risk of stroke. Because of the growing use of novel oral anticoagulants (NOAC) in patients with AF, it is important to understand whether the presence of hypertension interferes with the effects of these drugs versus conventional vitamin K antagonists (VKA). We therefore conducted a study in which we assessed patients with AF, the presence of hypertension and level of blood pressure control, and an interaction with the choice of oral anticoagulants on clinical outcomes.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used to undertake this review.
Data sources and searches
Electronic databases (MedLine/PubMed) were searched from database inception until the search date August 8 2019. We used key words for atrial fibrillation in combination with key words for hypertension or blood pressure and anticoagulants (VKA, NOACs) (Supplemental Table S1).
Study selection and population
Two investigators (REH, RDL) identified potentially eligible studies. We used an online systematic review platform (Rayyan, Qatar Computing Research Institute, Doha, Qatar). We applied the following inclusion criteria: 1) original data studies presenting follow-up data on stroke and major bleeding; 2) involving comparisons by presence of hypertension and/or blood pressure control; 3) involving a randomised comparison between a NOAC (apixaban, dabigatran, rivaroxaban, or edoxaban) versus a vitamin K antagonist (warfarin, coumadin, etc). Using these selection criteria, our population consisted of populations with AF randomised to NOAC/VKA, in which the comparative safety and efficacy was stratified by hypertension status and/or blood pressure control.
Outcomes of interest
The outcomes of interest were stroke or systemic embolism, haemorrhagic stroke, intracranial bleeding, and major bleeding.
Data extraction and quality assessment
One investigator (REH) extracted data elements from each study, with a second investigator (WAML) independently reviewing these data for accuracy. The quality of the studies were assessed using the Cochrane Risk of Bias tool for assessing risk of bias in randomised studies.
Data synthesis and analysis
Data were extracted and displayed in tables. Log adjusted hazard ratios (HR) and corresponding standard error were calculated, and HRs were compared using Mantel-Haenszel random effects to account for heterogeneity. Analyses were performed with Review Manager (RevMan version 5.3, The Cochrane Nordic Collaboration, Copenhagen, Denmark).
Results
Search results
Our search included 590 studies of which we assessed 19 in full-text. Of those, 5 studies met the inclusion criteria of our study. These studies were post-hoc analyses from the ARISTOTLE (apixaban versus warfarin) [Citation4], RE-LY (dabigatran versus warfarin) [Citation5], ENGAGE AF (edoxaban versus warfarin) [Citation6], and ROCKET-AF (rivaroxaban versus warfarin) [Citation7] and J-ROCKET (rivaroxaban versus warfarin in Japan) [Citation8] trials. The flowchart of our search strategy and reasons for exclusions can be found as Supplemental Figure S1.
Quality assessment
As shown in Supplemental Table S2, the five studies were well designed and conducted, which renders the risk of bias overall low. Given that both studies involved post-hoc analyses of randomised trials, we assessed for additional biases. We found no skewedness, with a balanced randomisation to NOAC versus VKA among patients with and without hypertension in all studies. A potential source of bias lies in the assumption that patients with elevated blood pressure levels or (poorly) controlled hypertension at baseline maintained this status throughout the study duration and vice versa.
Study and patient characteristics
The five included studies comprised 71,527 participants, who were enrolled at sites in the Americas, Europe and Asia between 2005 and 2010, with a median follow-up duration of 1.9–2.8 years. Average patient age at baseline was about 70, and hypertension was present in the vast majority of patients (n = 64,796; 90.5%; range of 79–100%). Compared to those without hypertension, patients with hypertension were more often female and had higher stroke risk (CHA2DS2-VASc score) and comparable bleeding risk (HAS-BLED). Of reported antihypertensive medications, ACE/ARBs were most commonly used, followed by beta-blockers (Supplemental Table S3).
Impact of hypertension and stroke or systemic embolism
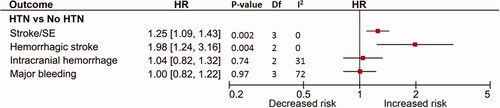
Patients with hypertension had higher risk for ischaemic stroke/SE (HR: 1.25, 95% CI: 1.09, 1.43) and haemorrhagic stroke (HR: 1.98, 1.24–3.16) compared with patients without hypertension at baseline (). Two studies provided data on incremental risks of systolic blood pressure, and showed that the risk of ischaemic stroke/SE increased by 6–7% per 10 mmHg rise [Citation5,Citation7]. The impact of poor blood pressure control on the risk of stroke/SE was further illustrated in ENGAGE-AF [Citation6]. Among hypertensive patients the hazard ratio for stroke/SE increased from 1.51 (1.23–1.85) (systolic blood pressure of 140–150 mmHg) to 2.01 (1.50–2.70) in those with ≥150 mmHg, using 130–140 mmHg as a reference.
Figure 1. Impact of hypertension on stroke and other adverse outcomes in patients with atrial fibrillation.
Impact of hypertension and bleeding outcomes
As shown in , no increased risk for bleeding complications was found in those with or without a history of hypertension. In a secondary analysis from ENGAGE-AF, however, the authors found an increased risk for major bleeding in those with uncontrolled versus controlled hypertension, with hazard ratios of 1.36 (1.13–1.62) and 1.64 (1.26–2.12) for systolic blood pressure of 140–150 and ≥150 mmHg, respectively [Citation6].
Impact of hypertension on the comparative efficacy and safety of NOACs versus VKA
The presence of hypertension did not interact with the comparative efficacy and safety of NOACs, as illustrated in the risk of stroke and major bleeding in , as well as for the remaining safety and efficacy outcomes. Both in patients with and without hypertension the use of NOACs had a more favourable efficacy and safety profile compared with VKA. Moreover, there was no difference in the efficacy or safety profile of NOACs among patients with controlled versus uncontrolled hypertension as shown in .
Figure 2. Impact of hypertension on comparative safety and efficacy of NOAC versus VKA.
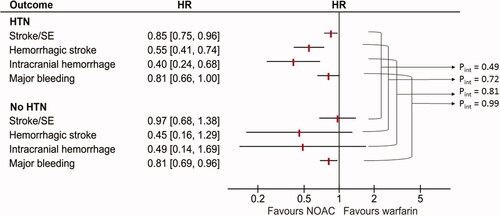
Table 1. Impact of hypertension control (> =140mmHg versus <140 mmHg) on the comparative efficacy and safety of NOAC versus VKA.
Discussion
Hypertension is a highly prevalent comorbidity in patients with AF who are treated with anticoagulants. In this study we found that the risks of ischaemic stroke/SE and haemorrhagic stroke were substantially increased in hypertensive patients, particularly in those with poor blood pressure control. The risk of stroke appears to follow a linear curve with 6–7% increased risk per 10 mmHg increase in systolic blood pressure. Furthermore, we evaluated the impact of hypertension status on the comparative safety and efficacy of NOACs. We found no such interaction for stroke or bleeding in controlled and uncontrolled hypertension, indicating that NOACs present an equal if not preferable option for prophylaxis stroke and systemic embolism in patients with AF irrespective of hypertension status or blood pressure control.
Strengths and limitations
The current study was performed using high-quality data from five randomised clinical trials comparing NOACs with VKA, with rigorous baseline assessment and clinical follow-up. The foremost limitation of our study was that we relied on study-level data from post hoc analyses, which did not allow us to adjust for possible confounding. Also, our analysis was limited by its dependence on baseline hypertension status and blood pressure assessment, with events recorded over follow-up, which may be years since the initial patient was recruited. There were no data on the impact of increased blood pressure variability or data on ambulatory blood pressure reading and the impact on outcomes. Furthermore, a number of trials excluded patients with very high blood pressure levels (≥170 to 180 mm Hg systolic), as such our findings may not cover the entire blood pressure spectrum. Finally, we lumped the NOACs together as a group/class, assuming that there would be no difference between individual NOACs in the interaction with hypertension.
Hypertension and atrial fibrillation: double trouble
Prevention of stroke is central to the management of AF, which involves the use of oral anticoagulation in the presence of risk factors [Citation9]. Hypertension is the commonest modifiable risk factor for stroke and thromboembolism risk (40–90%), both in clinical trial populations (as shown in our study) as well as in population-based cohorts [Citation2,Citation3]. Patients with AF also have a higher risk bleeding events, most notably intracranial haemorrhage, which is related to oral anticoagulation therapy as well as a higher intrinsic risk of bleeding [Citation10]. Similarly, the presence of (uncontrolled) hypertension is an important risk factor for bleeding, both in anticoagulated and non-anticoagulated patients [Citation10]. Moreover, adequate management of hypertension is important for rhythm control and heart failure [Citation11]. Therefore given these risks, adequate blood pressure control should form an integral part of the management of atrial fibrillation in order to reduce residual stroke risk among anticoagulated patients.
Optimal blood pressure target in atrial fibrillation
European guidelines on blood pressure control in general populations recommend that the first objective should be to lower blood pressure to <140/90 mmHg, and provided that treatment is well tolerated, treated blood pressure values should be targeted to 120–130/80 mmHg or 130–140 mmHg in older patients [Citation12]. These recommendations with respect to optimal targets for blood pressure may perhaps also be applicable in populations with AF. In an analysis from the Stroke Prevention using an Oral Thrombin Inhibitor in atrial Fibrillation (SPORTIF) III and V trials the authors found an increasing rate of ischaemic stroke/SE with increasing quartiles of systolic blood pressure, in which the event rate increased markedly at mean systolic blood pressure of >140 mmHg [Citation13]. These findings are in line with those from ROCKET-AF and ARISTOTLE which found that stroke event rates were lower in patients with controlled (<140mmHg systolic) versus uncontrolled hypertension (≥140 mmHg systolic) [Citation4,Citation7]. A secondary analysis from ENGAGE-AF suggests that systolic blood pressure levels of 110–130 mmHg may present the most optimal target for minimising stroke risk in anticoagulated patients with AF and hypertension [Citation6]. Similarly, a large Korean study (n = 298,374) among patients with AF undergoing hypertension treatment found that patients with blood pressure of 120–129/<80 mmHg had the lowest risk for major cardiovascular events compared with patients with higher and lower blood pressure levels (adjusted hazard ratios of 1.05 [1.01, 1.09], 1.05 [1.01–1.08] and 1.13 [1.09–1.16] for blood pressures of <120/80, 130–139/80–89 and ≥140/90 mmHg, respectively) [Citation14].
Blood pressure control intervention studies in atrial fibrillation
Randomised intervention studies have thus far been inconclusive, or were limited to select sub-populations [Citation15–18]. The most relevant study is ACTIVE-I (n = 9016), which showed that the intervention (irbesartan) led to a 2.9 mmHg greater reduction in systolic blood pressure and while the primary outcome of cardiovascular events was not significantly different, there was a reduction in cerebrovascular and embolic events (hazard ratio 0.87, 0.77–0.98) [Citation18]. Given the paucity of data and the increasing prevalence of hypertension and AF in our populations, future randomised intervention studies are warranted to investigate whether more stringent blood pressure targets will a) improve cardiovascular outcomes, and b) outweigh the risks (i.e. hypotension, syncope, electrolyte abnormalities and acute kidney injury).
Conclusion
The presence of hypertension is common and modifiable risk factor for stroke in patients with atrial fibrillation who receive anticoagulant therapy. Novel oral anticoagulants present an equal if not preferable option over warfarin both in terms of stroke and bleeding complications irrespective of hypertension status or blood pressure control.
Disclosure statement
Dr Harskamp reported receiving grants from the Dutch Research Council outside the submitted work. Prof. Lopes reported receiving consulting fees from Bayer, Boehringer Ingelheim, Daiichi Sankyo, Merck, and Portola Pharmaceuticals; and grants and consulting fees from Bristol-Myers Squibb, GlaxoSmithKline, Medtronic, Pfizer, and Sanofi outside the submitted work.
Additional information
Funding
References
- Staerk L, Wang B, Preis SR, et al. Lifetime risk of atrial fibrillation according to optimal, borderline, or elevated levels of risk factors: cohort study based on longitudinal data from the Framingham Heart Study. BMJ. 2018;361:k1453
- Liatakis I, Manta E, Tsioufis C. Hypertension and atrial fibrillation: epidemiological data, pathogenesis, and therapeutic implications. Am J Hypertens. 2019;32(8):725–726.
- Verdecchia P, Angeli F, Reboldi G. Hypertension and atrial fibrillation: doubts and certainties from basic and clinical studies. Circ Res. 2018;122(2):352–368.
- Rao MP, Halvorsen S, Wojdyla D, et al. Blood pressure control and risk of stroke or systemic embolism in patients with atrial fibrillation: results from the apixaban for reduction in stroke and other thromboembolic events in atrial fibrillation (ARISTOTLE) trial. J Am Heart Assoc. 2015;4(12):e002015.DOI:https://doi.org/10.1161/JAHA.115.002015
- Nagarakanti R, Wallentin L, Noack H, et al. Comparison of characteristics and outcomes of dabigatran versus warfarin in hypertensive patients with atrial fibrillation (from the RE-LY Trial). Am J Cardiol. 2015;116(8):1204–1209.
- Park S, Bergmark BA, Shi M, et al. Edoxaban versus warfarin stratified by average blood pressure in 19 679 patients with atrial fibrillation and a history of hypertension in the ENGAGE AF-TIMI 48 trial. Hypertension. 2019;74(3):597–605.
- Vemulapalli S, Hellkamp AS, Jones WS, et al. Blood pressure control and stroke or bleeding risk in anticoagulated patients with atrial fibrillation: results from the ROCKET AF Trial. Am Heart J. 2016;178:74–84.
- Matsumoto M, Hori M, Tanahashi N, J-ROCKET AF Study Investigators, et al. Rivaroxaban versus warfarin in Japanese patients with non-valvular atrial fibrillation in relation to hypertension: a subgroup analysis of the J-ROCKET AF trial. Hypertens Res. 2014;37(5):457–462.
- Lip GY, Nieuwlaat R, Pisters R, et al. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. 2010;137(2):263–272.
- Esteve-Pastor MA, Rivera-Caravaca JM, Lip GYH. Hypertension and atrial fibrillation: balancing stroke and bleeding risks. Am J Hypertens. 2017;30(11):1063–1065.
- Dzeshka MS, Shantsila A, Shantsila E, et al. Atrial fibrillation and hypertension. Hypertension. 2017;70(5):854–861.
- Williams B, Mancia G, Spiering W, List of authors/Task Force members, et al. 2018 Practice Guidelines for the management of arterial hypertension of the European Society of Hypertension and the European Society of Cardiology: ESH/ESC Task Force for the Management of Arterial Hypertension. J Hypertens. 2018;36(12):2284–2309.
- Lip GY, Frison L, Grind M, on behalf of the SPORTIF Investigators, et al. Effect of hypertension on anticoagulated patients with atrial fibrillation. Eur Heart J. 2007;28(6):752–759.
- Kim D, Yang PS, Kim TH, et al. Ideal blood pressure in patients with atrial fibrillation. J Am Coll Cardiol. 2018;72(11):1233–1245.
- Parkash R, Wells GA, Sapp JL, et al. Effect of aggressive blood pressure control on the recurrence of atrial fibrillation after catheter ablation: a randomized, open-label clinical trial (SMAC-AF [Substrate Modification With Aggressive Blood Pressure Control]). Circulation. 2017;135(19):1788–1798.
- Rienstra M, Hobbelt AH, Alings M, for the RACE 3 Investigators, et al. Targeted therapy of underlying conditions improves sinus rhythm maintenance in patients with persistent atrial fibrillation: results of the RACE 3 trial. Eur Heart J. 2018;39(32):2987–2996.
- Arima H, Hart RG, Colman S, PROGRESS Collaborative Group, et al. Perindopril-based blood pressure-lowering reduces major vascular events in patients with atrial fibrillation and prior stroke or transient ischemic attack. Stroke. 2005;36(10):2164–2169.
- Investigators AI, Yusuf S, Healey JS, et al. Irbesartan in patients with atrial fibrillation. N Engl J Med. 2011;364(10):928–938.

