

Abstract
Background: His bundle pacing (HBP) is a physiological alternative to biventricular (BiV) pacing. We compared short-term results of both pacing approaches in symptomatic atrial fibrillation (AF) patients with moderately reduced left ventricular (LV) ejection fraction (EF ≥35% and <50%) and narrow QRS (≤120 ms) who underwent atrioventricular node ablation (AVNA).
Methods: Thirty consecutive AF patients who received BiV pacing or HBP in conjunction with AVNA between May 2015 and January 2020 were retrospectively assessed. Electrocardiographic, echocardiographic, and clinical data at baseline and 6 months after the procedure were assessed.
Results: Twenty-four patients (age 68.8 ± 6.5 years, 50% female, EF 39.6 ± 4%, QRS 95 ± 10 ms) met the inclusion criteria, 12 received BiV pacing and 12 HBP. Both groups had similar acute procedure-related success and complication rates. HBP was superior to BiV pacing in terms of post-implant QRS duration, implantation fluoroscopy times, reduction of indexed LV volumes (EDVi 63.8 (49.6–81) mL/m2 vs. 79.9 (66–100) mL/m2, p = 0.055; ESVi 32.7 (25.6–42.6) mL/m2 vs. 46.4 (42.9–68.1) mL/m2, p = 0.009) and increase in LVEF (46 (41–55) % vs. 38 (35–42) %, p = 0.005). However, the improvement of the NYHA class was similar in both groups.
Conclusions: In symptomatic AF patients with moderately reduced EF and narrow QRS undergoing AVNA, HBP could be a conceivable alternative to BiV pacing. Further prospective studies are warranted to address the outcomes between both ‘ablate and pace’ strategies.
Introduction
Atrioventricular node ablation (AVNA) with right ventricular (RV) pacemaker implantation is a feasible symptomatic treatment option in patients with atrial fibrillation (AF) and rapid ventricular rate, refractory to optimal medical treatment. However, several studies reported neutral findings regarding heart failure (HF) progression and survival [Citation1–3], implying that beneficial effects of rate control and regularisation after AVNA could be hampered by non-physiologic dyssynchronous RV pacing [Citation4,Citation5]. While biventricular (BiV) pacing in conjunction with AVNA derived better results, the benefit was much less distinct in symptomatic AF patients with moderately reduced ejection fraction (EF) and narrow QRS [Citation6–10].
Following AVNA, permanent His bundle pacing (HBP) is an alternative to conventional RV and BiV pacing [Citation11,Citation12]. This physiological mode of pacing was introduced by Deshmukh et al. [Citation13] in 2000, who showed that by capturing the native conduction system, HBP provides normal synchronous activation and preserves left ventricular (LV) function in HF patients with AF and narrow QRS. Recent European Society of Cardiology guidelines for the management of supraventricular tachycardia (SVT) recommend that ‘ablate and pace’ strategy with either BiV pacing or HBP is reasonable when tachycardia-mediated cardiomyopathy cannot be ablated or controlled by pharmacological therapy (Class I, level of evidence C) [Citation14]. However, to the best of our knowledge, both pacing modalities in conjunction with AVNA were not previously compared, especially in the subgroups of patients where the benefit of BiV pacing after AVNA was less distinct.
The present study aimed to compare clinical and echocardiographic outcomes between BiV pacing and HBP in symptomatic AF patients with moderately reduced EF and narrow QRS who underwent AVNA.
Methods
The study complies with the Declaration of Helsinki and was approved by The Republic of Slovenia National Medical Ethics Committee (Komisija za medicinsko etiko Republike Slovenije) and the institutional review board. All patients gave written informed consent before the procedures were performed.
Study population
Thirty consecutive AF patients receiving BiV device (14 patients) or HBP (16 patients) in conjunction with AVNA between May 2015 and January 2020 were analysed in this single-centre observational study. The inclusion criteria were the following: (i) symptomatic permanent AF/atrial flutter refractory to pharmacological rate or rhythm control where ablation procedure failed or was deemed unwarranted [Citation14]; (ii) tachycardiomiopathy with ejection fraction (EF) ≥35% and <50%; (iii) tachycardia with narrow QRS complex (≤120 ms) [Citation14]; (iv) New York Heart Association (NYHA) class II–III; (v) patients were 18 years or older. The exclusion criteria were the following: (i) end-stage HF (NYHA IV); (ii) severe concomitant non-cardiac disease; (iii) need for surgical intervention; (iv) myocardial infarction less than 6 months before the procedure; (v) previous intracardiac device.
Procedures
Device implantation was always performed first, followed by AVNA. The lower rate of the pacing device was initially set to 80 bpm () and programmed to 70 bpm at 1-month follow-up.
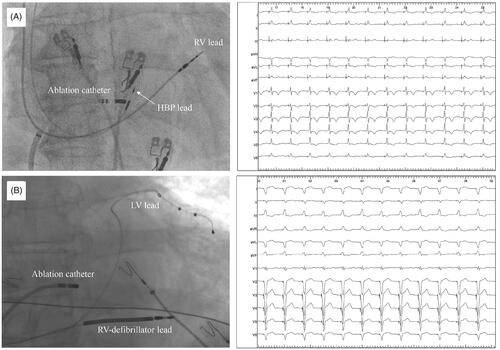
Figure 1. Fluoroscopic view of the ablation catheter in relation to His bundle pacing (Panel A) or biventricular pacing (Panel B) leads and 12-lead ECG after atrioventricular node ablation during both pacing modalities. RV: right ventricular; LV: left ventricular.
His bundle pacing
The procedure was performed as previously described [Citation11,Citation12]. In short, a 4.1 Fr bipolar active fixation lead (SelectSecure 3830, Medtronic, Minneapolis, MN, USA) and dedicated delivery sheath (C315His or C304, Medtronic, Minneapolis, MN, USA) were used for His bundle area mapping. His bundle potential mapping was performed in a unipolar setting with the use of the electrophysiological system (LAB system Pro, BARD/Boston Scientific, Lowell, MA, USA) at a sweep speed of 100 mm/s and under fluoroscopy. Additional visualisation of the tricuspid valve annulus via contrast injection through delivery sheath was usually performed before mapping to delineate the anatomical landmark of His bundle area. Distal HB potential with large ventricular signal and small atrial signal (ventricular to atrial electrogram ratio >3:1) was targeted before pacing lead was screwed into position. Acute HBP threshold ≤2.5 V at 1 ms was considered acceptable. HBP was categorised as selective or non-selective according to the recently proposed definitions [Citation15]. The additional backup lead was implanted in all patients and HBP lead was connected to the atrial port of the dual-chamber device. All HBP procedures were performed by a single experienced operator.
Biventricular pacing
Implantation of the BiV device was performed using standard techniques. The RV lead was positioned in the RV apex or septum. Non-apical, free lateral wall LV lead placement was preferred if permitted by the venous anatomy. Commercially available devices and leads were used. ECG-based VV delay optimisation to ensure left ventricular capture (Q wave in lead I, R wave in lead V1) and optimal QRS duration was performed after AVNA. All procedures were performed by two experienced operators.
Atrioventricular node ablation
AVNA was performed following device implantation which was temporarily set to 40 bpm for the duration of the procedure. After femoral vein access was obtained, a 4- or 3.5-mm irrigated tip ablation catheter (Flexability™, Abbott, Abbott Park, IL, USA or Celsius® Thermocool®, Biosense Webster, Irvine, CA, USA) was advanced through a long sheath (SR0; Fast-Cath™, Abbott, Abbott Park, IL, USA) into the right atrium. Right anterior oblique or anteroposterior view was used for positioning the catheter tip to the presumed area of the AV node in the mid-septum. Additional positioning was done according to the intracardiac electrograms (targeting atrial to the ventricular ratio for proximal AV node site). In the case of HBP, ablation in the close vicinity of the HBP lead tip was avoided by maintaining the ablation catheter tip at or below the level of the ring electrode (). Ablation was performed in a temperature-controlled mode (40 W, up to 60 s). If ablation was performed close to the HBP tip-electrode, as soon as AV block was achieved, pacing started from HBP lead at 0.5–1 V above capture threshold to monitor for any loss of capture. Successful AVNA was recognised with an abrupt drop of heart rate to 40 bpm and was continued for 60 s thereafter. A waiting period of 20 min was typically implemented. Any acute change of device lead position or pacing threshold following AVNA was documented.
Baseline assessment and follow-up
All electrocardiographic measurements were performed with the use of digital callipers at 400% magnification calibrated for paper speed 25 mm/s. Device interrogations, clinical and laboratory evaluations were performed at our device outpatient clinic at 1 month and 6 months post-implantation. Adverse events and device-related complications were closely monitored. Transthoracic two-dimensional echocardiography was performed at baseline and 6 months after device implantation. Body surface area (BSA)-indexed LV volumes and EF were calculated with the biplane Simpson method. Pre-procedural scar burden in patients with coronary artery disease (CAD) with magnetic resonance imaging (MRI) or myocardial perfusion imaging (MPI) was also assessed, if available.
Statistical analysis
For baseline and clinical characteristics, continuous variables were expressed as means and standard deviations or medians with interquartile ranges and compared with either paired or independent t-tests, or Mann–Whitney U tests, as appropriate. Categorical variables were expressed as relative counts and percentages and compared with χ2 tests of association. For all tests, a two-tailed p-value of ≤0.05 was considered statistically significant. All statistical analyses were conducted using IBM SPSS Statistics (Version 25.0., Armonk, NY, USA).
Results
Patient characteristics
A total of 24 patients who received HBP or BiV device after AVNA met the inclusion criteria; 12 patients out of 14 who received BiV device (1 excluded patient had a wide baseline QRS and 1 had EF <35%) and 12 out of 16 HBP recipients (1 excluded patient had wide baseline QRS, 2 had EF <35%, and 1 EF >50%). The mean age of the study population was 68.8 ± 6.5 years, 50% were female, median NYHA class was 3, mean EF was 39.6 ± 4%, and mean QRS width was 95 ± 10 ms. Permanent atrial flutter was present in 21% of the patients. All patients were receiving antiarrhythmic and anticoagulation therapy. No significant differences in baseline characteristics were observed between the groups (). At follow-up, 5 out of 8 patients discontinued loop diuretics in the HBP group (p = 0.034) and 1 out of 6 in the BiV group (p = 0.564). Digoxin and amiodarone were discontinued in all patients, the beta-blocker dosage was lower in all patients, however, the dosage of other HF medications at follow-up was unchanged compared to baseline.
Table 1. Baseline demographic and clinical characteristics of patients by pacing modality.
Pre-procedural MRI or MPI scans were available in 4 CAD patients (4/6) in the BiV cohort and in 2 CAD patients in the HBP group (2/3). Scar burden was very low in both groups and there was no significant scar tissue detected on the lateral LV (site of LV lead location) wall in patients who received BiV pacing.
Procedural outcomes
Device implantation and AVNA were acutely successful and performed simultaneously in all HBP patients. Initially, the C315 sheath was used and switched to C304 in only 2 patients. The ventricular backup lead was implanted in all HBP patients. Selective HBP was achieved in 5 patients (41.7%). Acute increase of HBP lead threshold after AVNA was registered in 1 patient (from 1.8 to 3.2 V at 1 ms). As the capture of the conduction system was still present, the lead revision was not performed. There were no other procedure-related adverse events. No significant change was found in the HBP lead threshold at baseline compared to 6-month follow-up (1.55 V (1.07–2.00) vs. 1.75 V (0.75–2.88), p = 0.230).
All BiV devices were successfully implanted. LV lead was positioned in the LV antero-lateral vein in 3 patients, in the lateral vein in 5 patients, and in the postero-lateral vein in 4 patients. In 3 patients, AVNA was successfully performed within 21 days after BiV device implantation and in 9 during the same hospitalisation. Left ventricular capture during BiV pacing was confirmed with ECG in all patients following AVNA. In one patient slight quadripolar LV lead, dislodgement was documented after AVNA, however, BiV pacing (R wave present in lead V1) with previous ECG morphology was restored after additional pacing vector programming. Thus, LV lead revision was not needed. There were no other procedure-related adverse events. No significant change in LV lead threshold (1.35 V (1.05–1.72) vs. 1.45 V (1.00–1.69); p = 0.475) was noted at follow-up.
Three patients had a defibrillator device for primary prevention in the BiV group and none in the HBP group (p = 0.064). No ventricular tachyarrhythmias were registered during the 6-month follow-up. Device implantation fluoroscopy time was significantly shorter in the HBP group compared to BiV group (p < 0.0001). Baseline QRS duration was similar in both treatment groups. Post-implant QRS duration did not change significantly in the HBP group (91 ± 12 ms vs. 95 ± 15 ms, p = 0.281) and prolonged in the BiV group (from 98 ± 7 ms to 172 ± 13 ms, p < 0.0001). Comparisons of both pacing modalities are presented in .
Table 2. Procedural characteristics and device parameters by pacing modality after atrioventricular node ablation at baseline and follow-up.
Echocardiography and clinical outcomes
Nine (75%) patients in the HBP group and 6 (50%) in the BiV group improved ≥1 NYHA class. Two patients (16.7%) declined by 1 functional class, both in the BiV group (p = 0.162). The median baseline NT-proBNP was 1771 pg/mL (1010–2752) and was similar between groups. In the HBP group, there was a significant reduction of NT-proBNP at follow-up (905 pg/mL (479–1911)) compared to baseline (1616 pg/mL (1010–2792)); p = 0.010. No significant decrease was observed in the BiV group at follow-up (1656 pg/mL (1190–2396)) compared to baseline (1904 pg/mL (1098–2559)); p = 0.625. Glomerular filtration rate (GFR) improved in the HBP group at follow-up (65 mL/min/1.73 m2 (54.4–71.5)) compared to baseline (58 mL/min/1.73 m2 (48–62.5)); p = 0.02. No significant improvement of GFR was observed in the BiV group at follow-up (59 mL/min/1.73 m2 (48.5–65.8)) compared to baseline (57.5 mL/min/1.73 m2 (50.3–61.5)); p = 0.365.
There were no significant baseline differences in indexed LV volumes and LVEF in patient groups based on treatment. At follow-up, LVEF improved significantly in HBP (40% (37–45) to 46% (41–55), p = 0.010). No significant change was observed in the BiV group (39% (35–40) vs. 38% (35–42), p = 0.579). Indexed LV volumes decreased in HBP group (LVEDVi 75 mL/m2 (54.7–94.3) to 63.8 mL/m2 (49.6–81); p = 0.013) and LVESVi (45.5 mL/m2 (33–55.3) to 32.7 mL/m2 (25.6–42.6); p = 0.005). No significant change in LV volumes was observed in BiV group: LVEDVi from 75.9 mL/m2 (65.3–93) to 79.9 mL/m2 (66–100); p = 0.225 and LVESVi from 47.9 mL/m2 (39.5–55.7) to 46.4 mL/m2 (42.9–68.1); p = 0.281. Comparison of mean changes in echocardiographic parameters are shown in and clinical and echocardiographic outcomes between the groups are presented in .
Figure 2. Comparison of mean changes in echocardiographic left ventricular volumes and ejection fraction between biventricular and His bundle pacing after atrioventricular node ablation at baseline and follow-up. LVEDVi: left ventricular end-diastolic volume indexed to body surface area; LVESVi: left ventricular end-systolic volume indexed to body surface area; LVEF: left ventricular ejection fraction; BiV: biventricular pacing; HBP: His bundle pacing.
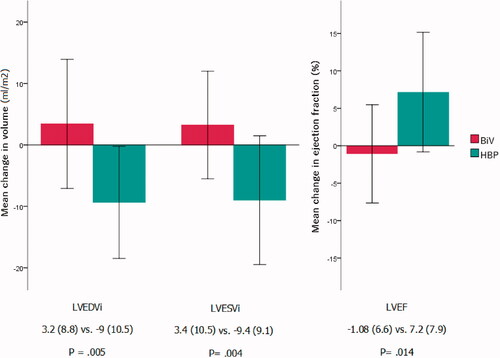
Table 3. Clinical and echocardiographic characteristics of patients by pacing modality after atrioventricular node ablation at baseline and follow-up.
Discussion
The results of our study indicate that in rate control refractory AF patients with moderately reduced EF (EF ≥35% and <50%) and narrow QRS (≤120 ms), HBP after AVNA provides superior ventricular activation and improvement of cardiac function compared to BiV pacing. However, both pacing modalities yielded similar symptomatic benefits.
Electrocardiographic and echocardiographic outcomes
Biventricular pacing could be detrimental in HF patients without significant electrical dyssynchrony as non-physiological ventricular resynchronisation does not return LV activation times to those seen in individuals with intrinsically narrow QRS [Citation16,Citation17]. Patients in our study who received BiV pacing and AVNA for symptomatic AF exhibited significant prolongation of QRS duration and no improvement in echocardiographic parameters. Although post-BiV QRS measurements in AVNA studies [Citation8–10] were not specifically addressed, a similar increase in QRS duration (40.2 ms) after BiV pacing could be observed in The Evaluation of Resynchronisation Therapy for Heart Failure (LESSER-EARTH) trial which enrolled HF patients with narrow QRS [Citation18]. Furthermore, Post AV-Nodal Ablation (PAVE) study showed that BiV pacing superiority was the consequence of functional deterioration in the RV pacing group rather than improvement in the BiV group where LVEF remained unchanged [Citation7]. In the study by Khan et al. [Citation19], which compared pulmonary-vein isolation and ‘ablate and pace’ strategy, a slight deterioration of LVEF (mean absolute change of −1 ± 4%) was noticed in the BiV group after AVNA. In contrast, the Ablate and Pace in Atrial Fibrillation (APAF) trial reported significant improvement of echocardiographic parameters in the BiV group alone and compared to RV pacing [Citation8]. Heterogenous study population could explain the discrepancy, as it is conceivable that the treatment effect of BiV pacing was more pronounced in patients with EF ≤35% (47% of patients) and QRS ≥120 ms (50% of patients) which were not included in our study [Citation8]. The same observation could be made in Ablate and Pace in Atrial Fibrillation plus Cardiac Resynchronisation Therapy (APAF-CRT) trial where, although echocardiographic parameters were not presented, no clear benefit of BiV pacing and AVNA compared to pharmacological treatment was observed in AF patients with narrow QRS and LVEF 36–50% [Citation10]. Focussing on these patients, the results of our study showed that HBP plus AVNA is associated with significant improvement of cardiac function compared to BiV pacing. Structural improvements observed in our HBP group resemble those in previous studies [Citation11,Citation12]. Therefore, it is reasonable to assume that HBP in conjunction with AVNA could be a better alternative to BiV pacing in rate control refractory AF patients with moderately reduced EF and narrow QRS.
Clinical outcomes
Alleviation of symptoms in HF patients with permanent AF is an interplay of adequate rate control and improvement of LV function [Citation20]. Symptomatic benefit after AVNA in our study was equal in both pacing modalities despite greater LV function improvement in HBP compared to BiV patients. This is in line with published data where the symptomatic benefit in a similar cohort of AF patients was mostly related to slowing and regularisation of heart rhythm after AVNA [Citation2,Citation6,Citation7]. Similar conclusions were made in the APAF-CRT trial, where patients with LVEF >35% exhibited significant symptomatic benefit after AVNA and BiV pacing, yet no clear benefit regarding mortality or HF progression [Citation10]. Therefore, our results of similar symptomatic improvement in both groups might imply that rate control after AVNA is the primary driver of symptom improvement in patients with moderately reduced EF while conduction system pacing alleviates the adverse effects of non-physiological BiV pacing in patients with narrow QRS.
Procedural outcomes and clinical implications
The recent development of dedicated tools and encouraging data from the literature made HBP a logical physiologic pacing option for patients undergoing the ‘ablate and pace’ strategy [Citation11–13]. However, there are several aspects that limit the wide applicability of this technique in routine clinical practice. Lower procedural success rates compared to BiV pacing or standard RV pacing, prolonged learning curve, higher initial capture thresholds with early battery depletion, and increased risk of sudden capture threshold fluctuations, including the need for lead revisions are frequently reported in HBP trials [Citation21,Citation22]. On the other hand, the current limitations of HBP might also reflect the early stage of new technology. Therefore, improvement of delivery tools, leads, and battery capacity could overcome these limitations and provide the grounds for wider clinical adoption.
Our study showed similar success and adverse event rates of HBP compared to BiV pacing with significantly lower device implantation fluoroscopy times. Lower HBP fluoroscopy times in our study compared to previous reports [Citation21] may be attributed to the implantation technique which primarily relies on intracardiac signals.
Compared to the BiV device, the AVNA procedure could prove more challenging in HBP due to the vicinity of HBP lead. However, by implanting the HBP lead more distally (no visible atrial electrograms) and by maintaining the ablation catheter tip at or below the level of the ring electrode we were able to avoid ablation-related complications. Of note, only one acute increase in His capture threshold was registered after AVNA. In line with previous reports, no significant increase in the short-term HBP lead threshold was observed [Citation11,Citation12].
Patients with tachycardiomyopathy are often very symptomatic and have greater mortality [Citation20]. The ‘ablate and pace’ strategy is a feasible therapeutic option when rhythm control interventions are no longer pursued [Citation14]. With long-term consequences of irreversible AVNA in mind, appropriate patient and therapy selection should be thoroughly considered. The results of our study indicate that compared to BiV pacing, HBP could provide an additional hemodynamic advantage in symptomatic AF patients with moderate HF and narrow QRS undergoing AVNA. Thus, larger prospective studies are warranted to address clinical and structural outcomes between both ‘ablate and pace’ strategies in different subgroups of rate control refractory AF patients.
Limitations
The retrospective design of the study and a low number of patients limits the strength of our findings. As only short-term procedural, clinical, and echocardiographic outcomes at 6-months were assessed, longer follow-up might have produced different results. Relatively high post-implant QRS duration (172 ± 13 ms) and more patients with coronary artery disease (although not statistically significant) in the BiV group might have impacted on the lack of echocardiographic improvement compared to the HBP group after AVNA. Additional pre-procedural imaging, intra-operative measurements (ventricular activation times, scar identification, etc.), and device optimisation could have yielded shorter BiV paced QRS intervals. However, in patients with narrow QRS undergoing BiV pacing and AVNA, LV lead positioning principally relies on the anatomical approach due to short interventricular delays, thus limiting this pacing method even further in case of unfavourable venous anatomy. Although pre-procedural scar tissue characterisation was not specifically addressed in patients with CAD, additional retrospective analysis of available MRI or MPI revealed low overall scar burden and no significant scar tissue at the site of LV lead location in patients who received BiV pacing. Moreover, low intra-operative LV pacing thresholds [Citation23] recorded in BiV patients might further imply a low probability of significant impact of regional scar (site of LV lead location) on echocardiographic outcomes compared to HBP. In addition, ECG-based VV delay optimisation to ensure left ventricular capture was performed in all patients. Finally, as only rate control refractory AF patients with moderately reduced EF (EF ≥35% and <50%) and narrow QRS (≤120 ms) were specifically assessed, the results cannot be extrapolated to other subgroups of patients undergoing AVNA. While we can assume a similar effect in patients with reduced EF [Citation12], the superiority of HBP in patients with wide QRS may be controversial since only proximal conduction abnormalities are amenable by recruitment of latent Purkinje fibres distal to the site of block [Citation24]. Finally, left bundle branch area pacing was recently introduced as a novel form of physiological pacing that could potentially overcome some limitations of HBP, such as higher capture thresholds, distal location of the conduction block with wide QRS, and technical challenges with a long learning curve [Citation25].
Conclusions
In symptomatic AF patients with moderately reduced EF and narrow QRS, His bundle pacing in conjunction with AVNA showed superior ventricular activation and improvement of cardiac function compared to BiV pacing. The short-term symptomatic benefit in both pacing modalities was similar. Larger prospective studies are warranted to address clinical and structural outcomes between both ‘ablate and pace’ strategies in different subgroups of rate control refractory AF patients.
Disclosure statement
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
References
- Ozcan C, Jahangir A, Friedman PA, et al. Long-term survival after ablation of the atrioventricular node and implantation of a permanent pacemaker in patients with atrial fibrillation. N Engl J Med. 2001;344(14):1043–1051.
- Tan E, Rienstra M, Wiesfeld A, et al. Long-term outcome of the atrioventricular node ablation and pacemaker implantation for symptomatic refractory atrial fibrillation. Europace. 2008;10(4):412–418.
- Chen L, Hodge D, Jahangir A, et al. Preserved left ventricular ejection fraction following atrioventricular junction ablation and pacing for atrial fibrillation. J Cardiovasc Electrophysiol. 2008;19:19–27.
- Tops LF, Schalij MJ, Holman ER, et al. Right ventricular pacing can induce ventricular dyssynchrony in patients with atrial fibrillation after atrioventricular node ablation. J Am Coll Cardiol. 2006;48(8):1642–1648.
- Vernooy K, Dijkman B, Cheriex EC, et al. Ventricular remodeling during long-term right ventricular pacing following His bundle ablation. Am J Cardiol. 2006;97(8):1223–1227.
- Brignole M, Gammage M, Puggioni E, et al. Comparative assessment of right, left, and biventricular pacing in patients with permanent atrial fibrillation. Eur Heart J. 2005;26(7):712–722.
- Doshi RN, Daoud EG, Fellows C, et al. Left ventricular-based cardiac stimulation post AV nodal ablation evaluation (the PAVE study). J Cardiovasc Electrophysiol. 2005;16(11):1160–1165.
- Brignole M, Botto G, Mont L, et al. Cardiac resynchronization therapy in patients undergoing atrioventricular junction ablation for permanent atrial fibrillation: a randomized trial. Eur Heart J. 2011;32(19):2420–2429.
- Chatterjee NA, Upadhyay GA, Ellenbogen KA, et al. Atrioventricular nodal ablation in atrial fibrillation: a meta-analysis of biventricular vs. right ventricular pacing mode. Eur J Heart Fail. 2012;14(6):661–667.
- Brignole M, Pokushalov E, Pentimalli F, et al. A randomized controlled trial of atrioventricular junction ablation and cardiac resynchronization therapy in patients with permanent atrial fibrillation and narrow QRS. Eur Heart J. 2018;39(45):3999–4008.
- Vijayaraman P, Subzposh FA, Naperkowski A. Atrioventricular node ablation and His bundle pacing. Europace. 2017;19(4):iv10–iv16.
- Huang W, Su L, Wu S, et al. Benefits of permanent His bundle pacing combined with atrioventricular node ablation in atrial fibrillation patients with heart failure with both preserved and reduced left ventricular ejection fraction. J Am Heart Assoc. 2017;6:e005309.
- Deshmukh P, Casavant DA, Romanyshyn M, et al. Permanent, direct His-bundle pacing: a novel approach to cardiac pacing in patients with normal His-Purkinje activation. Circulation. 2000;101(8):869–877.
- Brugada J, Katritsis DG, Arbelo E, et al. 2019 ESC Guidelines for the management of patients with supraventricular tachycardiaThe Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur Heart J. 2020;41(5):655–720.
- Vijayaraman P, Dandamudi G, Zanon F, et al. Permanent His bundle pacing: recommendations from a multicenter His bundle pacing collaborative working group for standardization of definitions, implant measurements, and follow-up. Heart Rhythm. 2018;15(3):460–468.
- Shah RM, Patel D, Molnar J, et al. Cardiac-resynchronization therapy in patients with systolic heart failure and QRS interval ≤130 ms: insights from a meta-analysis. Europace. 2015;17(2):267–273.
- Ploux S, Eschalier R, Whinnett ZI, et al. Electrical dyssynchrony induced by biventricular pacing: implications for patient selection and therapy improvement. Heart Rhythm. 2015;12(4):782–791.
- Thibault B, Harel F, Ducharme A, et al. Cardiac resynchronization therapy in patients with heart failure and a QRS complex <120 milliseconds: the Evaluation of Resynchronization Therapy for Heart Failure (LESSER-EARTH) trial. Circulation. 2013;127:873–881.
- Khan MN, Jaïs P, Cummings J, et al. Pulmonary-vein isolation for atrial fibrillation in patients with heart failure. N Engl J Med. 2008;359(17):1778–1785.
- Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129–2200.
- Keene D, Arnold AD, Jastrzębski M, et al. His bundle pacing, learning curve, procedure characteristics, safety, and feasibility: insights from a large international observational study. J Cardiovasc Electrophysiol. 2019;30(10):1984–1993.
- Zanon F, Abdelrahman M, Marcantoni L, et al. Long term performance and safety of His bundle pacing: a multicenter experience. J Cardiovasc Electrophysiol. 2019;30(9):1594–1601.
- Ferri-Certić J, Zavrl-Džananović D, Ležaić L, et al. Impact of left ventricular pacing threshold on ventricular arrhythmia occurrence in cardiac resynchronization therapy. J Cardiol. 2019;74(4):353–359.
- Upadhyay GA, Cherian T, Shatz DY, et al. Intracardiac delineation of septal conduction in left bundle-branch block patterns. Circulation. 2019;139(16):1876–1888.
- Vijayaraman P, Subzposh FA, Naperkowski A, et al. Prospective evaluation of feasibility and electrophysiologic and echocardiographic characteristics of left bundle branch area pacing. Heart Rhythm. 2019;16(12):1774–1782.

