

Abstract
Objectives
Neutrophil-to-lymphocyte ratio (NLR), one of the composite biomarker of systemic inflammatory status, was proved promising in predicting clinical outcomes of acute coronary syndrome (ACS). However, there were no evidences that NLR was directly relative to the clinical outcomes of unstable angina pectoris (UAP). Therefore, this study was aimed to detect whether NLR could predict the coronary artery lesion severity (indicated as SYNTAX score) and clinical outcomes (especially long-term cardiovascular mortality) in patients with.
Methods
In the single-centre retrospective study, 4110 patients with UAP were enrolled and divided into two groups according to their primary NLR values and followed up at a median time duration of 36 months. The differences of SYNTAX score and cardiovascular mortality between groups were analysed, and the predictive value of NLR was determined.
Results
NLR was positively and linearly correlated with SYNTAX score (r = 0.270). Diabetes (p = 0.049), lymphocyte (p = 0.004), NLR (p = 0.002) and SYNTAX score (p < 0.001) were independent predictors of long-term cardiovascular mortality in patients with UAP. Kaplan–Meier analysis revealed higher occurrence of cardiovascular mortality when NLR > 2.38 (p = 0.015). Receiver operating characteristic (ROC) analysis showed that NLR = 2.76 is an effective cut point for predicting cardiovascular mortality (69.2% sensitivity, 64.8% specificity).
Conclusions
NLR value was positively related to the severity of coronary artery lesion and proved to be an independent predictor of cardiovascular mortality in patients with UAP. This study would contribute to therapy and prognosis optimisation of UAP.
1. Introduction
Despite the technological development of diagnosis and treatment of acute coronary syndrome (ACS), new strategies for assisting therapy choice and predicting prognosis are still in demand, especially for non-ST elevation acute coronary syndrome (NSTE-ACS), which was prone to relate with multi-vessels lesion and poor prognosis [Citation1–3]. Predictive models, such as SYNTAX score, have been recommended by current guidelines as a reliable parameter which shows significant relation with severity of coronary artery lesion, helps to decide whether to perform percutaneous coronary intervention (PCI) and predicts long-term adverse outcomes for NSTE-ACS [Citation4,Citation5].
Recently, several studies demonstrated that inflammatory state which was indicated by blood cells counts and biochemical parameters would significantly impact on the clinical outcomes of patients with ACS [Citation6–8]. Since single parameter provided less information, composite parameters were preferred to describe comprehensive state of inflammatory and oxidative stresses, among which neutrophil-to-lymphocyte ratio (NLR) was proved to be promising with predictive value for ACS [Citation9,Citation10]. Meanwhile, NLR showed inflammatory state (indicated by neutrophil count and lymphocyte count) simultaneously with easier accessibility than SYNTAX score and other biomarkers.
However, few studies focussed on the predictive value of NLR on outcomes of unstable angina pectoris (UAP), which comprised a large proportion of NSTE-ACS and was prone to suffer poor outcomes similarly with non-ST elevation myocardial infraction (NSTEMI) [Citation11,Citation12]. Reliable parameters for therapy choice assistance and prognostic prediction would significantly standardise the treatment and improve the prognosis of UAP. Therefore, in this study, retrospective analysis of a large cohort of UAP patients in single centre was presented. The predictive value of coronary artery lesion severity and cardiovascular mortality of patients with UAP was studied statistically, which might contribute to the clinical application of NLR for therapy and prognosis optimisation of UAP in the future.
2. Materials and methods
This study was performed in accordance with the principles of the Declaration of Helsinki and was approved by the local institutional ethics committee with a waiver for informed consent (No. 2017-P2-123-01), and permission was granted to use data for analysis.
2.1. Study population
In this single-centre study, a total of 4573 patients were admitted to the Cardiovascular Centre in Beijing Friendship Hospital from December 2012 to December 2018 and underwent coronary angiography because UAP were retrospectively enrolled. UAP was defined as recurrent or worsen angina without rising myocardial enzymes (CK-MB, troponin I or T). All data of patients were collected at the endpoint by experienced investigators and checked by their coordinators.
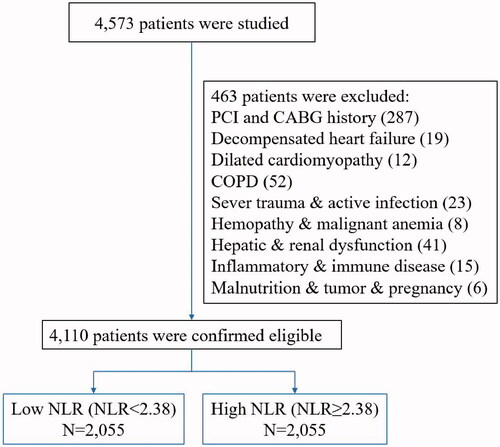
In order to decrease the influence of accompanying disease, 463 patients with a history of previous percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) surgery (287 cases), decompensated heart failure (19 cases), dilated cardiomyopathy (12 cases), chronic obstructive pulmonary disease (COPD) (52 cases), severe trauma and active infection (23 cases), haemopathy and malignant anaemia (8), hepatic and renal dysfunction (41 cases), inflammatory and immunologic disease (15 cases), malnutrition, malignant tumour and pregnancy (6 cases) were excluded. Finally, remaining 4110 patients were confirmed eligible and included in this study ().
Figure 1. Flow diagram of this study. NLR: neutrophil-to-lymphocyte ratio.
2.2. Clinical data and laboratory assay
Basic clinical information were collected by resident doctors on admission and extracted from medical history by investigators, which included (1) basic information: age, sex, systolic blood pressure (SBP) and diastolic blood pressure (DBP) and heart rate; (2) medical history of hypertension, diabetes, dyslipidaemia and stroke. Body mass index (BMI) was calculated as body weight (kg)/height square (m2).
Blood samples were collected for laboratory tests before any medical therapy and primary coronary angiography. Laboratory data of haemoglobin, platelet, lymphocyte, neutrophil, glucose, triglyceride (TG), total cholesterol (TC), high density lipoprotein-cholesterol (HDL-C) and low density lipoprotein-cholesterol (LDL-C) were extracted from medical history by investigators. NLR was calculated as the ratio of the neutrophil and lymphocyte, originated from the same blood sample on admission.
The study population was divided into two groups based on the NLR values. The low NLR group (n = 2055) was defined as patients with NLR values <2.38, while the high NLR was defined as patients with NLR values ≥ 2.38.
2.3. Coronary angiography and SYNTAX score
Coronary angiography was performed using standard techniques. Angiographic images of coronaries were extracted from medical history of patients. The number (single vessel or multi-vessels) and severity (percentage of coronary artery blockage) of coronary arteries involved were recorded by investigators.
The severity of coronary atherosclerotic lesions was assessed and recorded as SYNTAX score. The SYNTAX score was calculated with online tool (http://www.syntaxscore.com) [Citation13] by two experienced cardiologists, respectively, who were blinded to the laboratory and clinical data of patients. Coronary artery lesions ≥50% stenosis in vessels ≥ 1.5 mm was scored. A third cardiologist would evaluate the coronary angiograms with disagreement between above two assessments.
2.4. Follow-up and cardiovascular mortality
All patients were informed and scheduled for clinical follow-up at 1st, 3rd and 6th month as well as 1st, 2nd, 3rd and 5th year after being discharged or earlier if any relative symptoms emerged. The follow-up data were collected by investigators with hospital records, outpatient services and telephone calls. Medical treatment, relative symptoms and their frequency, adverse event, rehospitalisation, death and cause were recorded when patients were followed up. All-cause mortality was regarded as endpoint in this study.
The occurrence of cardiovascular mortality, which was defined as death caused by congestive heart failure, cardiac arrest and villainous arrhythmias during follow-up period was recorded in detail.
2.5. Statistical analysis
Continuous variables were presented as median values and standard deviations, which were compared between groups by T-test. Categorical variables were presented as numbers and percentages and compared between groups using Chi-square test. Statistical analyses were performed by using SPSS 19.0 (Chicago, Illinois, The USA) software. Statistical significance was set as p < 0.05.
Pearson correlation analysis was performed to assess the correlation of NLR with SYNTAX score. Univariate and multiple Cox proportional hazards models were used to determine independent factors of cardiovascular mortality. Hazard ratios (HRs) were presented with 95% confidence intervals (CIs) to show the risk of a factor when apparent. The receiver operating characteristic (ROC) curves was used to evaluate the predictive accuracy of NLR for cardiovascular mortality and determine a cut-off value of NLR. Kaplan–Meier survival curves were constructed to evaluate the prognostic value of NLR.
3. Results
From December 2012 to December 2018, a total of 4110 patients (2507 male, 56.85%; mean age 64.60 ± 9.65) with the diagnosis of UAP were enrolled and followed up during median 36.00 months (range 1–72 months).
3.1. Characteristics of the low NLR and high NLR groups
According to NLR of patients, the population was evenly divided into two groups: low NLR group (NLR < 2.38, n = 2055) and high NLR group (NLR ≥ 2.38, n = 2055). Baseline characteristics, laboratory tests and coronary angiographic findings are presented in . There were no significant differences between groups in gender (p = 0.774), BMI (p = 0.557), SBP (p = 0.596), DBP (p = 0.962), history of dyslipidaemia (p = 0.617), haemoglobin (p = 0.432), platelet (p = 0.275), glucose (p = 0.116), TC (p = 0.067), HDL-C (p = 0.506), LDL-C (p = 0.136), or multi-vessels ratio (p = 0.411). High NLR group owned higher age (64.72 versus 64.48, p = 0.027), HR (71.12 versus 69.52 bpm, p = 0.032), hypertension (75.03% versus 69.52%, p < 0.001), diabetes (39.08% versus 33.92%, p = 0.001), history of stroke (17.76% versus 13.72%, p < 0.001), neutrophil (4.76 versus 3.54 k/μL, p < 0.001), NLR (3.512 versus 1.80, p < 0.001), SYNTAX score (17.59 versus 16.89, p = 0.022) and lower lymphocyte (1.43 versus 2.01 k/μL, p < 0.001), TG (1.52 versus 1.74 mmol/L, p < 0.001). Meanwhile, NLR showed significant linear correlation with SYNTAX score (r = 0.270, p < 0.001) ().
Figure 2. Correlation of neutrophil-to-lymphocyte ratio with SYNTAX score (Each dot represents one patient; the straight line represents the best fit line obtained by linear regression analysis).
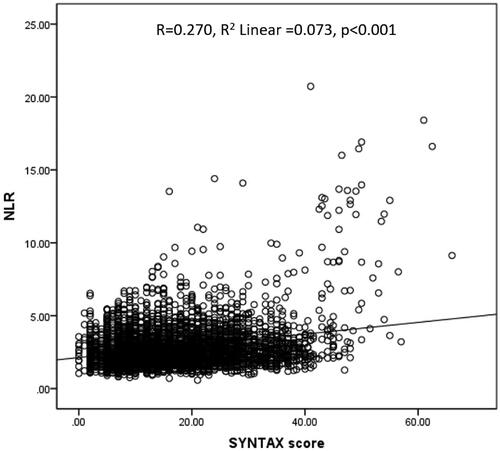
Table 1. Baseline characteristics of groups stratified by NLR.
3.2. NLR as an independent predictor of UAP prognosis
There were no significant differences of the follow-up time between low NLR group (31.84 ± 15.99 months) and high NLR group (31.49 ± 15.79 months) (p = 0.404). During follow-up period, the rehospitalisation was mainly caused by increased and frequently occurred symptoms, non-fatal myocardial infarction or acute heart failure. There were no significant difference of rehospitalisation rate between low NLR group (21.31%) and high NLR group (20.78%) (p = 0.674). However, high NLR group owned significantly higher cardiovascular mortality (0.58% versus 1.31%, p = 0.016) and all-cause mortality (1.95% versus 3.07%, p = 0.028) than low NLR group ().
Table 2. Clinical outcome of groups stratified by NLR.
Cox regression analysis was used to detect the independent predictor of clinical outcomes of patients with UAP (). In univariate Cox regression analysis, diabetes (p = 0.011), haemoglobin (p = 0.012), lymphocyte (0.001), NLR (p = 0.002) and SYNTAX score (p < 0.001) were significant predictors of cardiovascular mortality. In multiple Cox regression analysis, diabetes (p = 0.049), lymphocyte (p = 0.004), NLR (p = 0.002) and SYNTAX score (p < 0.001) were significant predictors of cardiovascular mortality. Therefore, diabetes, lymphocyte, NLR and SYNTAX score were independent predictors of cardiovascular mortality in patients with UAP.
Table 3. Univariate and multiple Cox regression analysis of the factors predicting cardiac mortality in patients with UAP.
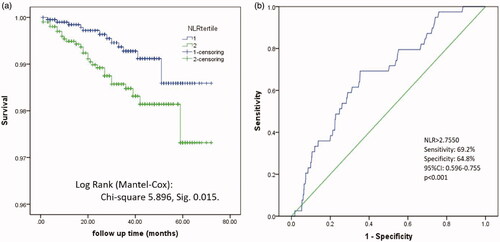
Kaplan–Meier analysis according to the event-free survival revealed higher occurrence of cardiovascular mortality in the high NLR group (p = 0.015) (). Receiver operating characteristic (ROC) analysis showed that NLR > 2.7550 had 69.2% sensitivity and 64.8% specificity for cardiovascular mortality (area under the curve: 0.676) ().
Figure 3. Kaplan–Meier survival curve showed the (a) cardiovascular mortality and (b) all-cause mortality of groups stratified by NLR. NLR: neutrophil-to-lymphocyte ratio.
4. Discussions
In this study, a total of 4110 patients diagnosed with UAP were retrospectively studied and followed up within six years. It showed that NLR value increased with an increase of SYNTAX score and was positively correlated with SYNTAX score, which indicated that NLR could predict the severity of coronary artery lesion of patients with UAP. Meanwhile, NLR was resulted as one of the independent factors which could predict the long-term cardiovascular mortality of UAP. Patients with higher NLR value suffered from higher cardiovascular mortality during follow-up period. The present study was the first to demonstrate an association of NLR with coronary artery lesion and clinical outcomes in patients with UAP.
NLR, a composite parameter indicated systemic inflammatory, was discovered to be significantly correlated with cardiovascular disease [Citation14]. A higher NLR value was discovered to predict cardiac arrhythmias [Citation15] and correlated with higher mortality of ACS, frequent congestive heart failure [Citation16,Citation17] and valvular heart disease [Citation18]. Since the coronary artery lesion of ACS was closely relative to the systemic inflammatory, the relationship of NLR and ACS was more attractive and well-studied recently. Neutrophil was regarded as a major actor in inflammatory and the waterfall effects of inflammatory reactions were finally contributed to the formation of atherosclerotic plaques and thromboses [Citation19,Citation20]. On the contrary, lymphocyte was discovered to stimulate the anti-inflammatory factor secretion of mononuclear cells [Citation21]. Meanwhile, it was indicated by Karackattu et al. [Citation22] that lymphocyte count was drastically low in patients with cardiac events. Therefore, the combination of high neutrophil count and low lymphocyte count might provide more information of the current state of coronary artery lesion and help to predict the progression. Notably, in this study, lymphocyte count was discovered to be an independent predictor of the cardiovascular mortality, which indicated that lower lymphocyte might correlate to the unstable plaque in coronary artery of patients with UAP and result in adverse prognosis.
NLR was reported to own significantly predicting value of ACS prognosis. Higher NLR value was correlated with worse clinical outcomes of ACS. Soylu et al. [Citation23] demonstrated that NLR predicted coronary artery lesion severity and mortality after NSTE-ACS. Kaya H et al. [Citation24] showed that NLR was independently associated with the severity of coronary artery lesion in patient with NSTEMI. Meanwhile, NLR was discovered to correlate with the risk prediction model such as higher GENSINI, GRACE and SYNTAX score. Kurtul et al. [Citation25] indicated that NLR was linearly correlated with SYNTAX score (coefficient β = 0.380, 95% CI 1.165–1.917, p < 0.001) in an NSTEMI cohort. Zhou et al. [Citation26] proved an enhanced predictive value of NLR combined with the GRACE risk score on the PCI outcomes of patients with acute coronary syndrome (ACS). In a large coronary artery disease (CAD) cohort prospective study, NLR was found to be a good predictor of GENSINI score and the presence of CAD (OR = 1.18, 95%CI: 1.09–1.27, p = 0.009) [Citation27]. In our results, admission NLR of patients with UAP was positively and linearly correlated to the SYNTAX score and was one of the predictors of cardiovascular mortality. NLR >2.755 might better predict cardiovascular mortality according to ROC curve, which included nearly 31.34% (1382/4410) patients with UAP.
Close relationship was discovered between NLR and cardiovascular mortality of UAP in a long-term follow-up period in this study, which was indicated that NLR might largely mirror the actual state of coronary artery lesion and could help choose a more suitable therapy plan. However, in consideration of the NLR performed as a non-specific parameter for coronary artery lesion and UAP, low NLR with prediction for low risk of cardiovascular mortality was more believable than high NLR for high risk of cardiovascular mortality [Citation23,Citation28]. A more specific biomarker beyond NLR was still to be discovered.
5. Limitations
Several limitations of this study were presented here. First, this was a retrospective single-centre study. The conclusion might be selectively applicable to other clinical centre. Second, the treatment of patients in this UAP cohort was not mentioned and studied as a factor for the survival analysis. The drug and intervention therapies could hardly be standardised and were adjusted according to the admission cardiac examination and systemic condition of patients. Third, not all information was involved for the predictor discovery in cardiovascular mortality analysis. Notably, myocardial enzyme and BNP of patients were not mentioned for their negativity in patients with UAP. Fourth, the lack of comprehensive adverse events, like during a long-term follow-up period was due to insufficient retrospective data. A more detailed follow-up might provide a different point-of-view.
6. Conclusions
NLR, a composite biomarker, was retrospectively tested in this study based on a large cohort of UAP. It was indicated that NLR value was positively related to the severity of coronary artery lesion and proved to be an independent predictor of cardiovascular mortality in patients with UAP. This study would contribute to therapy and prognosis optimisation of UAP.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Hamm CW, Bassand JP, Agewall S, et al. ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: the task force for the management of acute coronary syndromes (ACS) inpatients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2011; 32:2999–3054.
- Fox KA, Dabbous OH, Goldberg RJ, et al. Prediction of risk of death and myocardial infarction in the six months after presentation with acute coronary syndrome: prospective multinational observational study (GRACE). BMJ. 2006;333(7578):1091.
- Terkelsen CJ, Lassen JF, Norgaard BL, et al. Mortality rates in patients with ST-elevation vs. non-ST elevation acute myocardial infarction: observations from an unselected cohort. Eur Heart J. 2005;26(1):18–26.
- Kaya MG, Sahin O, Akpek M, et al. Relation between serum total bilirubin levels and severity of coronary artery disease in patients with non-ST-segment elevation myocardial infarction. Angiology. 2014; 65(3):245–249.
- van Gaal WJ, Ponnuthurai FA, Selvanayagam J, et al. The syntax score predicts peri-procedural myocardial necrosis during percutaneous coronary intervention. Int J Cardiol. 2009; 135(1):60–65.
- Sarli B, Baktir AO, Saglam H, et al. Neutrophil-to-lymphocyte ratio is associated with severity of coronary artery ectasia. Angiology. 2014; 65(2):147–151.
- Libby P, Ridker PM, Hansson GK. Inflammation in atherosclerosis: from pathophysiology to practice. J Am Coll Cardiol. 2009;54(23):2129–2138.
- Libby P. Inflammation in atherosclerosis. Arterioscler Thromb Vasc Biol. 2012; 32(9):2045–2051.
- Kaya MG, Akpek M, Lam YY, et al. Prognostic value of neutrophil/lymphocyte ratio in patients with ST-elevated myocardial infarction undergoing primary coronary intervention: a prospective, multicenter study. Int J Cardiol. 2013; 168(2):1154–1159.
- Akpek M, Kaya MG, Lam YY, et al. Relation of neutrophil/lymphocyte ratio to coronary flow to in-hospital major adverse cardiac events in patients with ST-elevated myocardial infarction undergoing primary coronary intervention. Am J Cardiol. 2012; 110(5):621–627.
- Chesebro JH, Fuster V. Thrombosis in unstable angina. N Engl J Med. 1992; 327(3):192–194.
- Vogrin S, Harper R, Paratz E, et al. Comparative effectiveness of routine invasive coronary angiography for managing unstable angina. Ann Intern Med. 2017; 166(11):783–791.
- SYNTAX Working Group. SYNTAX score calculator. Available from: http://www.SYNTAXscore.com.
- Afari ME, Bhat T. Neutrophil to lymphocyte ratio (NLR) and cardiovascular diseases: an update. Expert Rev Cardiovasc Ther. 2016; 14(5):573–577.
- Bruins P, Te Velthuis H, Yazdanbakhsh AP, et al. Activation of the complement system during and after cardiopulmonary bypass surgery: postsurgery activation involves C-reactive protein and is associated with postoperative arrhythmia. Circulation. 1997; 96(10):3542–3548.
- Prabhu SD. Cytokine-induced modulation of cardiac function. Circ Res. 2004; 95(12):1140–1153.
- Benites-Zapata VA, Hernandez AV, Nagarajan V, et al. Usefulness of neutrophil-to-lymphocyte ratio in risk stratification of patients with advanced heart failure. Am J Cardiol. 2015; 115(1):57–61.
- Baysal E, Burak C, Cay S, et al. The neutrophil to lymphocyte ratio is associated with severity of rheumatic mitral valve stenosis. J Blood Med. 2015; 6:151–156.
- Ortega E, Gilabert R, Nunez I, et al. White blood cell count is associated with carotid and femoral atherosclerosis. Atherosclerosis. 2012; 221(1):275–281.
- Borissoff JI, Otten JJ, Heeneman S, et al. Genetic and pharmacological modifications of thrombin formation in apolipoprotein e-deficient mice determine atherosclerosis severity and atherothrombosis onset in a neutrophil-dependent manner. PLoS One. 2013; 8(2):e55784.
- Frangogiannis NG, Smith CW, Entman ML. The inflammatory response in myocardial infarction. Cardiovasc Res. 2002; 53(1):31–47.
- Karackattu SL, Picard MH, Krieger M. Lymphocytes are not required for the rapid onset of coronary heart disease in scavenger receptor class B type I/apolipoprotein E double knockout mice. Arterioscler Thromb Vasc Biol. 2005; 25(4):803–808.
- Soylu K, Gedikli O, Dagasan G, et al. Neutrophil-to-lymphocyte ratio predicts coronary artery lesion complexity and mortality after non-ST-segment elevation acute coronary syndrome. Rev Port Cardiol. 2015; 34(7–8):465–471.
- Kaya H, Ertaş F, İslamoğlu Y, et al. Association between neutrophil to lymphocyte ratio and severity of coronary artery disease. Clin Appl Thromb Hemost. 2014;20(1):50–54.
- Kurtul S, Sarli B, Baktir AO, et al. Neutrophil to lymphocyte ratio predicts syntax score in patients with non-st segment elevation myocardial infarction. Int Heart J. 2015; 56(1):18–21.
- Zhou D, Wan Z, Fan Y, et al. A combination of the neutrophil-to-lymphocyte ratio and the GRACE risk score better predicts PCI outcomes in Chinese Han patients with acute coronary syndrome. Anatol J Cardiol. 2015; 15(12):995–1001.
- Chen J, Chen MH, Li S, et al. Usefulness of the neutrophil-to-lymphocyte ratio in predicting the severity of coronary artery disease: a gensini score assessment. JAT. 2014; 21(12):1271–1282.
- Sawant AC, Adhikari P, Narra SR, et al. Neutrophil to lymphocyte ratio predicts short- and long-term mortality following revascularization therapy for ST elevation myocardial infarction. Cardiol J. 2014;21(5):500–508.

