

Abstract
Background
Cardiovascular disease (CVD) is one of the leading causes of death in Belgium. Current strategies for the prevention and management of CVD focus on reducing low-density lipoprotein cholesterol (LDL-C) levels. This analysis assessed whether LDL-C goals, recommended by the European Society of Cardiology (ESC)/European Atherosclerosis Society (EAS) guidelines, were being achieved in a Belgian study population.
Methods
The cross-sectional, observational, DA VINCI study enrolled patients prescribed lipid-lowering therapy (LLT) between 21 June 2017 and 20 November 2018. Data for patients from Belgium were extracted for this country-specific analysis. Primary endpoint was the proportion of patients who achieved 2016 ESC/EAS risk-based LDL-C goals; attainment of 2019 risk-based LDL-C goals was evaluated post hoc.
Results
Of 497 enrolled patients, 41% were female and mean age was 68 years. Among subjects with an LDL-C measurement on stabilised LLT, moderate-intensity statin monotherapy was the most prescribed LLT regimen (59%). Overall, 63% of patients achieved their risk-based LDL-C goals according to the 2016 ESC/EAS guidelines. Among patients with established ASCVD, risk-based LDL-C goal attainment was higher in patients with peripheral arterial disease (53%) than patients with coronary (37%) and cerebrovascular disease (42%). According to the updated 2019 ESC/EAS guidelines, less than half (41%) of patients achieved their risk-based LDL-C goal. The proportion of primary and secondary prevention patients who achieved 2019 risk-based LDL-C goals was 59% and 18%, respectively.
Conclusion
These findings reveal a large gap between the LDL-C goals advocated by the ESC/EAS and the levels achieved in routine clinical practice in Belgium.
Introduction
In Belgium, cardiovascular disease (CVD) is the leading cause of death among women and second only to cancer in men [Citation1]; it is responsible for approximately 20% and 25% of premature deaths in women and men, respectively [Citation2]. Current strategies for the prevention and management of CVD focus on reducing risk factors such as low-density lipoprotein cholesterol (LDL-C) levels [Citation3]. Randomised clinical trials and real-world evidence have shown that the reduction of LDL-C levels using lipid-lowering therapies (LLT) reduces the risk of CVD [Citation4–7].
The European Society of Cardiology (ESC)/European Atherosclerosis Society (EAS) guidelines provide recommendations for optimal LLT use and propose LDL-C goals for the management of CVD. These guidelines advise the use of statin regimens (low-, moderate- or high-intensity) as the first-line treatment to lower LDL-C levels [Citation8,Citation9]. In addition, LDL-C goals were set for different groups of patients based on cardiovascular (CV) risk profile (low, moderate, high or very high) [Citation8,Citation9]. The 2016 ESC/EAS guidelines recommended an LDL-C goal of lower than 100 mg/dL (2.6 mmol/L) for patients at high CV risk and lower than 70 mg/dL (1.8 mmol/L) for those at very-high CV risk. In comparison, even lower LDL-C goals have been set in the more recent 2019 ESC/EAS guidelines (<70 mg/dL [1.8 mmol/L] and <55 mg/dL [1.4 mmol/L] for those at high and very high risk, respectively) in comparison with the 2016 LDL-C goals. Furthermore, the 2019 guidelines advised a goal of at least a 50% reduction in LDL-C from pre-treatment levels. A sequential therapeutic strategy to reduce LDL-C was also proposed: use of high-intensity statins prescribed up to a maximally tolerated dose and subsequent use of combination therapy with ezetimibe or with a proprotein convertase subtilisin/kexin type 9 (PCSK9i), if goals are not achieved [Citation8].
Statins are the most commonly prescribed LLT in Belgium, with 1.5 million primary care patients treated with statins in 2016, corresponding to 13% of the total population and 25% of the population older than 40 years of age [Citation3]. However, despite the use of statin therapy, approximately 70% out of 531 patients at very high CV risk did not achieve their risk-based LDL-C goal of 70 mg/dL in a Belgian observational study (published in 2014) [Citation10]. Similarly, the EUROASPIRE V survey, which interviewed 8261 patients with coronary artery disease across 27 European countries, found that most patients did not achieve their LDL-C goals [Citation11]. These data suggest that further optimisation of LLT use in clinical practice is required to achieve the goals set by the current ESC/EAS guidelines.
Although LDL-C levels have been identified as a major risk factor for CVD, hypertension and diabetes are also known to be closely linked with CVD [Citation12,Citation13]. However, the impact of these comorbidities on lipid control is not well established. Studies have demonstrated that blood pressure goal attainment among the Belgian population remains low [Citation14–16]. There is also a growing number of patients with type 2 diabetes mellitus [Citation17]. Given the increasing burden of these risk factors in Belgium, the association among hypertension, diabetes and dyslipidaemia warrants further evaluation.
The DA VINCI study provided contemporary data on rates of LDL-C goal achievement and LLT treatment patterns across Europe [Citation18]. The aim of this country-specific analysis was to assess whether risk-based LDL-C goals were being achieved in Belgian participants from the DA VINCI study.
Methods
Study design
The cross-sectional DA VINCI study enrolled patients from primary and secondary care clinics across 18 European countries. The full study design has been published previously [Citation18]. Briefly, patients were enrolled between 21 June 2017 and 20 November 2018. There were no formal study visits; patients were recruited in chronological order during routine clinic visits, meaning that patients who met the eligibility criteria were invited to participate on the study in the order that they were seen in clinic, until the recruitment target at the study site was fulfilled. Site selection and site caps were put in place to ensure that a target proportion was reached of primary prevention patients (approximately 50% of the overall study population) as well as a target ratio of coronary: cerebral: peripheral disease of 1:2:2 among secondary prevention patients. The following data were obtained from medical records and at single enrolment visit; patient demographics, the most recent LDL-C value up to 14 months before enrolment and all LLT history. LDL-C was calculated using the Friedewald formula as per standard protocols in European pathology laboratories and it is was not specified to be fasting (most recent measurement regardless of fasting status) [Citation18]. The study was designed by the Academic Executive Committee in conjunction with the sponsor, Amgen (full protocol available online [ENCePP; registration no. EU PAS 22075]). The study protocol was approved by the institutional review board or independent ethics committee for each site.
For this country-specific analysis, data for 497 patients from 13 care sites in Belgium were extracted from the DA VINCI study dataset. Patients were categorised into two subgroups at enrolment: primary and secondary prevention. Primary and secondary prevention patients were enrolled in a 1:1 ratio. Participants were considered primary prevention patients if they had no previous history of CV events upon LDL-C measurement. For this subset, the 10-year risk of fatal CVD was calculated using the Systematic Coronary Risk Evaluation (SCORE) [Citation19] and estimated glomerular filtration rate (eGFR) at LDL-C measurement. Patients in the primary prevention subgroup were further categorised according to their CV risk as low, moderate, high or very high risk, according to the ESC/EAS guidelines [Citation8]. Patients who had established atherosclerotic cardiovascular disease (ASCVD) documented prior to LDL-C measurement were considered as secondary prevention. These patients were categorised by the investigator according to predominant underlying disease being managed at enrolment (peripheral artery, cerebrovascular, or coronary disease) and the data were analysed accordingly. For this subset, the 10-year risk of the next CV event was calculated at LDL-C measurement, using the Reduction of Atherosclerosis for Continued Health (REACH) [Citation20] score; all patients were considered very high risk.
Eligibility criteria
Full eligibility criteria are available in the DA VINCI study [Citation18]. Briefly, major inclusion criteria included: being 18 years of age or older; providing informed consent; being prescribed LLT at enrolment or within the previous 12 months; and having an LDL-C measurement recorded up to 14 months before enrolment (most recent measurement; not calculated and regardless of fasting status) was obtained independently of participation in a clinical trial). Major exclusion criteria included: a diagnosis of familial hypercholesterolaemia (FH) with a history of CV events; comorbidities or personal circumstances that could affect clinical decision-making; a positive HIV status; pregnancy or breastfeeding; participation in an interventional clinical trial within 6 months before the enrolment date; and a life expectancy of less than 1 year at enrolment.
Aims and outcomes
The aim of this country-specific analysis was to assess whether risk-based LDL-C goals were being achieved in Belgian participants from the DA VINCI study.
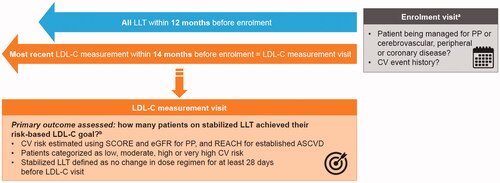
The primary outcome was the proportion of patients on stabilised LLT, who achieved risk-based LDL-C goals recommended by the 2016 ESC/EAS guidelines. Stabilised LLT was defined as no change in dose or regimen for at least 28 days before LDL-C measurement (). For individuals defined as primary prevention at LDL-C measurement, 10-year CV death risk was estimated using systematic coronary risk evaluation (SCORE) and they were categorised as low–moderate, high, or very high risk according to the ESC/EAS guidelines. All patients defined as secondary prevention were categorised as very high risk. Estimated 10-year CV risk at LDL-C measurement in established ASCVD groups was estimated using REACH.
Figure 1. DA VINCI study schema. aPatients were enrolled at a single visit between June 2017 and November 2018. bPatients who were not stabilised on any LLT or had their LDL-C measurement taken before any LLT was initiated were not included in the assessment of the primary outcome. ASCVD: atherosclerotic cardiovascular disease; CV: cardiovascular; eGFR: estimated glomerular filtration rate; LDL-C: low-density lipoprotein cholesterol; LLT: lipid lowering therapy; PP: primary prevention; REACH: REduction of Atherothrombosis for Continued Health; SCORE: Systematic COronary Risk Evaluation.
Given that this study was completed before the publication of the updated 2019 ESC/EAS guidelines, a post hoc analysis was performed to evaluate the proportion of patients achieving the LDL-C goals advocated by the 2019 guidelines. Secondary outcomes included the type of LLT prescribed to patients at the enrolment date.
Statistical analysis
All analyses were descriptive. Continuous variables are reported as mean and standard deviation (SD) or standard error for normally distributed data. For categorical variables, the number and percentage of patients in each category are reported.
Results
Patient characteristics
Patient characteristics are shown in . A total of 497 patients (249 primary prevention and 248 secondary prevention) were enrolled from Belgium. Mean (SD) age was 68 (10) years. Mean (SD) systolic blood pressure was 135 (17) mmHg and diastolic blood pressure was 77 (10) mmHg.
Table 1. Baseline characteristics and demographics of the study population.
The proportion of patients with hypertension was 70.6% (351/497). Among these patients, mean systolic blood pressure (SD) was 136 mmHg (17) and mean diastolic blood pressure (SD) was 77 mmHg (10). In addition, 40.8% (203/497) of patients had type 2 diabetes mellitus. In this subset of patients, the mean (SD) glucose level was 136 mg/dL (43) (7.5 mmol/L [2.4]); 105 were primary prevention and 92 were secondary prevention, and their mean (SD) glucose level was 140 mg/dL (46) (7.7 mmol/L [2.6]) and 131 mg/dL (40) (7.3 mmol/L [2.2]), respectively. Fasting glucose measurement was not mandatory. However, approximately 78% of glucose measurements collected were fasted.
Site characteristics
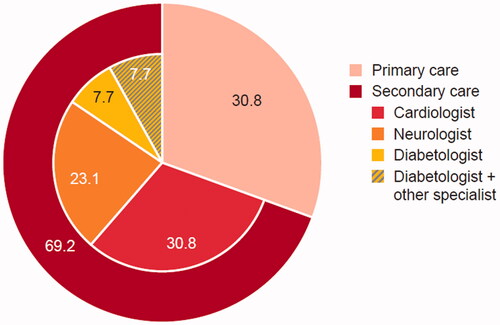
Of the 13 Belgian sites included in this study, there were four primary care centres (30.8%) and nine secondary care clinics (69.2%) (). Patients treated in a secondary care setting were seen by different types of specialists including cardiologists (30.8% [4/13]), neurologists (23.1% [3/13]), diabetologists (15.4% [2/13]) and others (7.7% [1/13]) ().
Figure 2. Site characteristics and specialities within secondary care. aA single site can provide different specialities of secondary care. Patients were enrolled across 13 sites in Belgium.
CV Risk profile
Most primary prevention patients, who had evaluable data for LDL-C measurement, were classified as patients with moderate CV risk (81.2%) (). Moreover, 11.9% (31/261) and 1.9% (5/261) of patients were considered high risk and very high risk, respectively.
Figure 3. CV risk profile in (a) primary prevention patients by SCORE, (b) secondary prevention patients by REACH, (c) ASCVD type in secondary prevention patients. aPrimary prevention patients (n = 261) at LDL-C measurement, with a CV risk calculated using SCORE. bSecondary prevention patients (n = 204) at LDL-C measurement, with data available to calculate the REACH score. cPatients with established ASCVD (n = 239) at enrolment, who were categorised as very-high risk. dPatients with evidence of atherosclerosis or other manifestations of vascular disease at enrolment. ASCVD: atherosclerotic cardiovascular disease; CV: cardiovascular; LDL-C: low-density lipoprotein cholesterol; REACH: Reduction of Artherothrombosis for Continued Health; SCORE: Systemic Coronary Risk Evaluation.
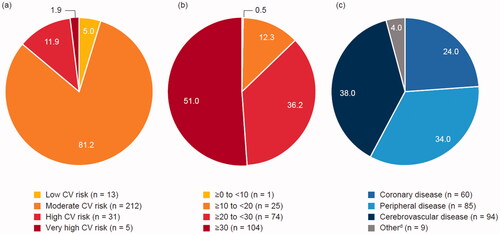
The estimated 10-year risk for the next CV event could be calculated for 204 secondary prevention patients; approximately half had a predicted CV risk greater than 30%. Over one-third of patients had a predicted CV risk greater than 20% (). Of 239 secondary prevention patients, who had established ASCVD, 38.0% had cerebrovascular disease, 34.0% had peripheral disease and 24.0% had coronary artery disease ().
LLT treatment patterns
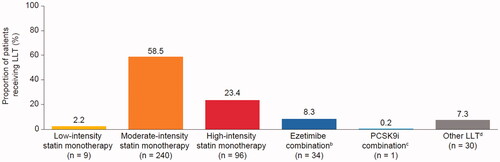
At LDL-C measurement, 93.4% (383/410) of patients received statin therapy, which was the most commonly prescribed LLT. The most frequently prescribed regimen at LDL-C measurement was moderate-intensity statin monotherapy (58.5%) (). Out of 184 secondary prevention patients on stabilised LLT, the majority were receiving moderate- (50.5% [93/184]) or high-intensity statin monotherapy (36.4% [67/184]). Only 8.3% of patients were receiving ezetimibe combination therapy and only one patient (0.2%) received PCSK9i combination therapy ().
Figure 4. LLT treatment patterns at LDL-C measurement. aPatients with stabilised LLT at LDL-C measurement. bEzetimibe combination: patients who were treated with ezetimibe plus a statin of moderate, high or unknown intensity. cPCSK9i combination: patients who were treated with PCSK9i plus a statin of low-, moderate-, high-, or unknown intensity; PCSK9i plus ezetimibe or PCSK9i plus a statin and ezetimibe. dOther LLT: ezetimibe without statin or PCSK9i, PCSK9i without statin or ezetimibe, ezetimibe plus low-intensity statin, unknown intensity statin without ezetimibe or PCSK9i or other LLTs such as fibrates, fish oil etc. LDL-C: low-density lipoprotein cholesterol; LLT: lipid-lowering therapy; PCSK9i: proprotein convertase subtilisin/kexin type 9 inhibitor.
Attainment of 2016 ESC/EAS guideline LDL-C goals
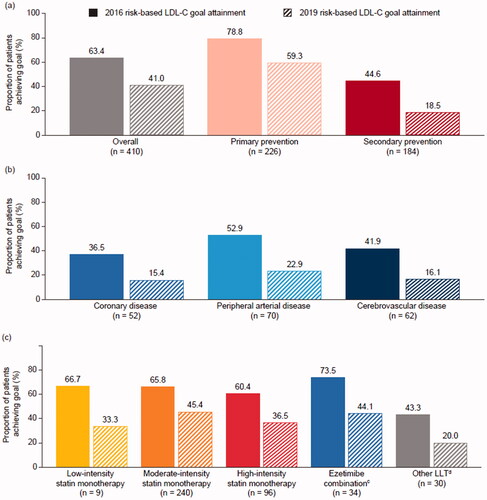
Overall, 63.4% of patients achieved LDL-C goals according to the 2016 ESC/EAS guidelines (). Among primary and secondary prevention patients, 78.8% and 44.6% achieved 2016 LDL-C goals, respectively (). Among these patients with established ASCVD, risk-based LDL-C goal attainment was higher in patients with peripheral arterial disease (52.9%) than patients with cerebrovascular (41.9%) and coronary (36.5%) disease. (). LDL-C goal attainment was highest among patients receiving ezetimibe combination therapy, with approximately three-quarters of patients achieving their risk-based goal (). Goal attainment was similar between males (63.3%) and females (63.5%).
Figure 5. Risk-based LDL-C goal attainment in (a) primary and secondary prevention patients, (b) secondary prevention patients categorised by ASCVD type,a (c) patients categorised by LLT.b. aPatients (n = 410) were receiving stabilised LLT at LDL-C measurement and had data available to assess risk-based goal attainment. bPatients (n = 410) on stabilised LLT therapy and evaluable for goal attainment. cEzetimibe combination: patients who were treated with ezetimibe plus statin of moderate, high or unknown intensity. dOther LLT: Patients treated with ezetimibe without statin or PCSK9i; PCSK9i without statin or ezetimibe; ezetimibe plus statin of low or unknown intensity without ezetimibe or PCSK9i; other LLTs such as fibrates, fish oils, etc. ASCVD: atherosclerotic cardiovascular disease; LDL-C: low-density lipoprotein cholesterol; LLT: lipid-lowering therapy; PCSK9i: proprotein convertase subtilisin/kexin type 9 inhibitor.
Attainment of 2019 ESC/EAS guideline LDL-C goals
Less than half (41.0%) of patients achieved their risk-based LDL-C goals, recommended by the 2019 ESC/EAS guidelines (). The proportion of primary and secondary prevention patients who achieved their 2019 LDL-C goals was 59.3% and 18.5%, respectively. (). Among patients with ASCVD, goal attainment was minimal; only 15.4% of patients with coronary disease were at goal for LDL-C (). Furthermore, less than half of patients met their LDL-C goals, irrespective of the prescribed LLT (). Goal attainment was similar in patients receiving moderate-intensity statin monotherapy (45.4%) and ezetimibe combination therapy (44.1%). Goal attainment for males and females was respectively 39.6% and 42.9%.
Risk-based goal attainment in patients with hypertension and type 2 diabetes mellitus
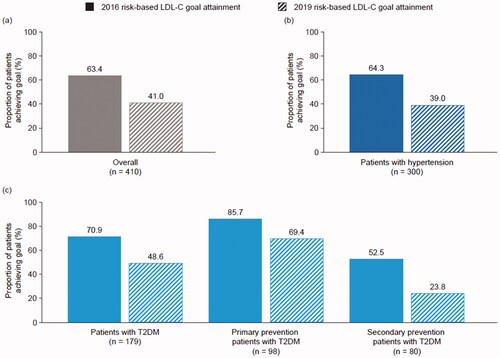
Of 351 patients with hypertension, 300 were evaluable for goal attainment in this subgroup. The proportion of patients who achieved 2016 and 2019 LDL-C goals was 64.3% and 39.0%, respectively (). Among patients with type 2 diabetes mellitus, 179 were evaluable for goal attainment. Attainment of 2016 and 2019 LDL-C goals was 70.9% and 48.6%, respectively (). Of 98 primary prevention patients with type 2 diabetes mellitus who were on stabilised LLT and thus were evaluable for LDL-C goal attainment, 85.7% and 69.4% achieved 2016 and 2019 LDL-C goals, respectively (). Among 80 evaluable secondary prevention patients with type 2 diabetes mellitus, over half (52.5%) of patients achieved 2016 LDL-C goals, but only approximately one-quarter (23.8%) of patients achieved 2019 LDL-C goals ().
Figure 6. Risk-based goal attainment in patients with hypertension and type 2 diabetes mellitus. LDL-C: low-density lipoprotein cholesterol; T2DM: type 2 diabetes mellitus.
LDL-C Levels in patients receiving stabilised LLT and evaluable for goal attainment
Overall, the mean (SD) LDL-C level in the study population was 83.9 mg/dL (31.7) (2.2 mmol/L). Patients with hypertension had a mean (SD) LDL-C of 82.8 mg/dL (30.6) (2.2 mmol/L [0.8]). In the subset of patients with type 2 diabetes mellitus this was 75.4 mg/dL (27.8) (2.0 mmol/L [0.7]) overall. The mean (SD) LDL-C in primary and secondary prevention patients with type 2 diabetes was 78.4 mg/dL (29.2) (2.0 mmol/L [0.8]) and 71.6 mg/dL (25.9) (1.9 mmol/L [0.7]), respectively.
Discussion
More than half of the Belgian participants from the DA VINCI study (63%) achieved 2016 LDL-C goals. However, the proportion of patients who would have achieved LDL-C goals as advocated by the updated 2019 ESC/EAS guidelines were considerably lower (41%). These results are generally in line with those observed in the overall European population. In total, 54% of the overall European population attained the 2016 risk-based LDL-C goals and 33% attained their goal according to the 2019 ESC/EAS guidelines [Citation18].
Among secondary prevention patients, only 19% of patients would have achieved 2019 LDL-C goals. At the time of recruitment of this study (2017), moderate- and high-intensity statin monotherapy was the most commonly prescribed LLT regimens in both primary prevention patients at moderate CV risk and in secondary prevention patients. Notably, the highest proportion of patients who achieved 2016 LDL-C goals was receiving ezetimibe combination therapy.
The findings of this analysis highlight a marked gap between the LDL-C goals recommended by the ESC/EAS and the LDL-C levels achieved in clinical practice in Belgium. The Dyslipidemia International Study (DYSIS), a Belgian study, showed that more than half of all patients (56.2%) did not achieve risk-based LDL-C goals according to 2011 ESC/EAS guidelines. At that time, the DYSIS study indicated that despite statin treatment, lipid abnormalities remained highly prevalent, pointing at the need for more aggressive lipid-lowering treatment [Citation10]. Our findings provide more recent data to support this and suggest that although treatment options have evolved, LDL-C levels are still not well controlled in most patients. A shift in LLT treatment patterns may be required to be able to achieve optimal lipid control, as recommended in the latest ESC/EAS guidelines. Low use of ezetimibe and PCSK9i can be explained by limited access in only a subset of patients in Belgium at the time of the study.
The question can be asked whether the most recent ESC/EAS guidelines have become too strict in relation to the recommended LDL-C goals. The 2019 guidelines recommend a decrease in the LDL-C goal from 70 to 55 mg/dL for very high-risk patients (i.e. those with an ASCVD event or other very high-risk conditions that increase their 10-year risk to a similar level) [Citation8]. For high-risk patients, it remains at 70 mg/dL. The merits of attaining LDL-C levels of around 53 mg/dL compared to 70 mg/dl in very high-risk patients were shown in the IMPROVE-IT study [Citation21]. In this study evaluating the addition of ezetimibe 10 mg to simvastatin 40 mg in post-acute coronary syndrome (ACS) patients, the overall NNT to prevent one event was 50. Subgroup analyses showed that NNT further decreased in patients with risk-enhancing factors such as diabetes, peripheral arterial disease or for instance those with prior coronary artery bypass graft (CABG) [Citation22]. The EAS Task Force recognises that the new LDL-C goals for high and very-high-risk patients with dyslipidaemia are more demanding and cite the data from DA VINCI, where only one-third of the patients attained their LDL-C goal according to the 2019 guidelines [Citation23]. This taskforce suggests a shift from monotherapy to combination therapies and emphasises the need for greater routine use of combination therapies as the standard of care offering evidence-based practical guidance for their implementation [Citation23].
Of note, a higher proportion of patients with peripheral arterial disease achieved their 2016 LDL-C goals compared with patients with coronary and cerebrovascular disease. Patients with peripheral disease have been shown to benefit from the pleiotropic effects of statins, additional to the reduction of LDL-C. For instance, statins can result in improvement of pain-free walking and overall health-related quality of life, enabling patients to increase physical activity which could play a role in further reduction of LDL-C levels [Citation24,Citation25]. Having an active lifestyle and exercise are key factors that are recommended for CVD management and have been shown to improve lipid control [Citation26].
Blood pressure control has been reported to be low among the Belgian population [Citation14–16]. While there is no established causal relationship between hypertension and elevated LDL-C levels, some anecdotal analyses have shown that patients with hypertension are more likely to have elevated LDL-C levels than patients with normotensive blood pressure [Citation27,Citation28]. Nevertheless, hypertension was well controlled among the patients enrolled from Belgium in the DA VINCI study. Additionally, LDL-C goal attainment was similar in patients with hypertension compared with the overall population. Despite blood pressure parameters being well controlled, lipid levels remained above-recommended levels. A possible explanation is that adequate blood pressure control was achieved with use of multiple anti-hypertensive medications such as diuretics and beta-blockers, which can have deleterious effects on the lipid profile [Citation29].
Patients with type 2 diabetes were overrepresented in this study (40%). Diabetes is an important risk factor for ASCVD. Patients with type 2 diabetes have an at-least moderate risk and a minimum LDL-C target <100mg/dL (2019 ESC/EAS guidelines [Citation8] and for those with risk-enhancing factors even lower targets, and are thus more likely to be offered lipid-modifying therapy and eligible for enrolment. In addition, a number of study sites specialised in diabetology (20/128 site overall, and 2/9 sites within Belgium). Patients with type 2 diabetes mellitus showed better goal attainment, with a lower mean LDL-C, than the overall population. It should be noted that in Belgium, patients with type 2 diabetes are followed in a care program integrating primary care and annual visit with specialists. In a recent evaluation of the effectiveness of this care program, it was found that the quality of care for type 2 diabetes patients evaluated using the intermediate health outcome parameters increased. A higher percentage of patients had controlled blood pressure, lower LDL cholesterol and HbA1c after inclusion in this care program for type 2 diabetes [Citation30].
This analysis has some limitations that should be discussed. The primary DA VINCI study, from which these data were extracted, is a cross-sectional study in which a longitudinal follow-up of the enrolled patients was not carried out. Some patient groups such as those receiving ezetimibe combination therapy had a low sample size, which should be considered when interpreting results. Baseline LDL-C levels were not recorded and thus, it was not possible to quantify whether patients achieved a 50% reduction in LDL-C levels from the untreated state, as recommended by the 2019 ESC/EAS guidelines. Baseline LDL-C levels, clinician bias in prescribing LLTs and local prescribing restrictions at the time the study was carried out could have had an impact on the levels of goal attainment observed. Finally, sites that participate in registries do not necessarily reflect the practices of those who don’t. These sites tend to be more interested in research and in LLT, so perhaps manage patients better. As such the findings may not reflect the ‘worse cases scenario’.
Conclusions
The findings of this real-world cross-sectional study highlight the need for change in clinical practices for the management of dyslipidaemia in Belgium. This study raises awareness of the burden of dyslipidaemia and stresses the importance of optimising LLT regimens used in Belgium to achieve recommended LDL-C goals.
Author contributions
KKR contributed substantially to the study design and concept; KKR, PvdB were involved in data acquisition; SB conducted the data analyses; and PvdB, KKR, SB assisted with interpretation of the data. All authors were involved in drafting of the manuscript, provided critical revisions for important intellectual content, approved the final version submitted for publication, and agreed to be accountable for all aspects of the work.
Acknowledgements
The authors thank Natasha Rangwani, PhD, of PharmaGenesis London, London, UK, for medical writing support. The authors also acknowledge Dr. Gaia Kiru, Dr. Jennifer Murphy and Mrs. Amanda Bravery from Imperial College London for the additional support and K.K.R. acknowledges his support by the NIHR Imperial Biomedical Research Centre
Disclosure statement
KKR reports: grants from Amgen, during the conduct of the study; personal fees from AbbVie, Aegerion, Akcea, Algorithm, AstraZeneca, Bayer, Boehringer Ingelheim, Cerenis, Cipla, Dr Reddy’s, Esperion, Kowa, Lilly, The Medicines Company, Novartis, Silence Therapeutics, Takeda and Zuellig Pharma; and grants and personal fees from Amgen, Daiichi Sankyo, MSD, Pfizer and Sanofi/Regeneron, outside the submitted work. PvdB employer received honoraria for lecturing/advisory boards from Amgen, Bayer, Boehringer-Ingelheim, Idorsia, Menarini, Novartis, Novo Nordisk, Sanofi, and Servier. SB is an employee of Amgen Ltd.
Additional information
Funding
References
- OECD. Belgium: Country health profile 2017. 2017 [Accessed 9 Feb 2021]. Available from: https://www.oecd.org/belgium/belgium-country-health-profile-2017-9789264283299-en.htm
- Renard F, Tafforeau J, Deboosere P. Premature mortality in Belgium in 1993-2009: leading causes, regional disparities and 15 years change. Arch Public Health. 2014;72(1):34.
- Cordon A, De Meester C, Gerkens S, et al. Statins for the primary prevention of cardiovascular events. Health Technology Assessment (HTA) Brussels. KCE Reports 306. Belgian Health Care Knowledge Centre (KCE); 2019.
- Di Angelantonio E, Sarwar N, Perry P, et al.; Emerging Risk Factors Collaboration. Major lipids, apolipoproteins, and risk of vascular disease. Jama. 2009;302(18):1993–2000.
- Lewington S, Whitlock G, Clarck R, et al. Blood cholesterol and vascular mortality by age, sex, and blood pressure: a Meta-analysis of individual data from 61 prospective studies with 55 000 vascular deaths. The Lancet. 2007;370:1829–1839.
- Baigent C, Blackwell L, Emberson J, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a Meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376:1670–1681.
- Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376(18):1713–1722.
- Mach F, Baigent C, Catapano AL, et al.; ESC Scientific Document Group. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41(1):111–188.
- Catapano AL, Graham I, De Backer G, et al.; ESC Scientific Document Group. 2016 ESC/EAS guidelines for the management of dyslipidaemias. Eur Heart J. 2016;37(39):2999–3058.
- Devroey D, Radermecker RP, Van der Schueren BJ, et al. Prevalence of persistent lipid abnormalities in statin-treated patients: Belgian results of the dyslipidaemia international study (DYSIS). Int J Clin Pract. 2014;68(2):180–187.
- Kotseva K, De Backer G, De Bacquer D, et al.; on behalf of the EUROASPIRE Investigators*. Lifestyle and impact on cardiovascular risk factor control in coronary patients across 27 countries: Results from the european society of cardiology ESC-EORP EUROASPIRE V registry. Eur J Prev Cardiolog. 2019;26(8):824–835.
- Kjeldsen SE. Hypertension and cardiovascular risk: General aspects. Pharmacol Res. 2018;129:95–99.
- Leon BM, Maddox TM. Diabetes and cardiovascular disease: epidemiology, biological mechanisms, treatment recommendations and future research. World J Diabetes. 2015;6(13):1246–1258.
- Van der Niepen P, Thijs V, Devroey D, et al. Belgian global implementation of cardiovascular and stroke risk assessment study: methods and baseline data of the BELGICA-STROKE STUDY. Eur J Cardiovasc Prev Rehabil. 2011;18(4):635–641.
- Leeman M, Dramaix M, Van Nieuwenhuyse B, et al. Cross-sectional survey evaluating blood pressure control ACHIEVEment in hypertensive patients treated with multiple anti-hypertensive agents in Belgium and Luxembourg. PLoS One. 2018;13(11):e0206510.
- Borne PVD, Missault L, Persu A, et al. The COMmon control of hypErtenSion and therapeutic attitudes in BelgIum and luxemburg study (COME STAI). Acta Cardiol. 2016;71(1):35–40.
- Van Casteren VF, Bossuyt NH, Moreels SJ, et al. Does the belgian diabetes type 2 care trajectory improve quality of care for diabetes patients? Arch Public Health. 2015;73(1):31.
- Ray K, Molemans B, Schoonen W, et al.; the DA VINCI study. EU-Wide Cross-Sectional observational study of Lipid-Modifying therapy use in secondary and primary care: the DA VINCI study. Eur J Prevent Cardiol. 2021;28(11):1279–1289.
- Conroy R, Pyörälä K, Fitzgerald A, et al. Estimation of ten-year risk of fatal cardiovascular disease in Europe: the SCORE project. Eur Heart J. 2003;24(11):987–1003.
- Wilson PW, D'Agostino R, Sr., Bhatt DL, et al. An international model to predict recurrent cardiovascular disease. Am J Med. 2012;125(7):695–703.e1.
- Cannon CP, Blazing MA, Giugliano RP, et al. Ezetimibe added to statin therapy after acute coronary syndromes. N Engl J Med. 2015;372(25):2387–2397.
- Pradhan A, Bhandari M, Sethi R. Ezetimibe and improving cardiovascular outcomes: current evidence and perspectives. Cardiol Res Pract. 2020;2020:9815016.
- Averna M, Banach M, Bruckert E, et al. Practical guidance for combination lipid-modifying therapy in high- and very-high-risk patients: a statement from a european atherosclerosis society task force. Atherosclerosis. 2021;325:99–109.
- Poredos P, Jezovnik MK. Do the effects of secondary prevention of cardiovascular events in PAD patients differ from other atherosclerotic disease? Int J Mol Sci. 2015;16(7):14477–14489.
- Mohler ER, 3rd, Hiatt WR, Creager MA. Cholesterol reduction with atorvastatin improves walking distance in patients with peripheral arterial disease. Circulation. 2003;108(12):1481–1486.
- Wang Y, Xu D. Effects of aerobic exercise on lipids and lipoproteins. Lipids Health Dis. 2017;16(1):132.
- Choudhury KN, Mainuddin AKM, Wahiduzzaman M, et al. Serum lipid profile and its association with hypertension in Bangladesh. Vas Health Risk Manage. 2014;10:327–332.
- Osuji CU, Omejua EG, Onwubuya EI, et al. Serum lipid profile of newly diagnosed hypertensive patients in nnewi, South-East Nigeria. Int J Hypertens. 2012;2012:710486.
- Herink M, Ito MK. Medication induced changes in lipid and lipoproteins [updated 2018 May 10]. In: Feingold KR, Anawalt B, Boyce A, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000. Available from: https://www.ncbi.nlm.nih.gov/books/NBK326739/
- Goossens M, Kalyvas C, Kennel T, et al. De zorgtrajecten diabetes mellitus type 2 en chronische nierinsufficiëntie en kwaliteit van zorg. Brussel: Sciensano. Depotnummer; 2017–2019.

