

Abstract
Randomised clinical trials, observational studies, and meta-analyses have shown that sodium–glucose cotransporter 2 inhibitors (SGLT2-i) reduce the risk of hospitalisation for heart failure (HF), chronic kidney disease (CKD) progression, and mortality in patients with HF, irrespective of the presence of type 2 diabetes mellitus. However, real-world epidemiology may differ from clinical trial populations, thereby limiting generalisability and delaying the introduction of novel treatments in clinical practice.
The aim of the present study was to assess the prevalence of DAPA-HF (Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure) inclusion criteria in a population of HF with reduced ejection fraction (HFrEF) patients enrolled in the Italian Network on Heart Failure (IN-HF) registry.
Overall, 3415 IN-HF patients matched the 4744 patients in DAPA-HF, overlapping for most baseline characteristics (e.g. similar average ejection fraction), with a slightly lower prevalence of type 2 diabetes and of HF ischaemic aetiology and a higher percentage of NYHA class II patients. The theoretical eligibility to DAPA-HF in a cardiology setting resulted to be 73%.
The availability of an easily accessible database from a large nationwide prospective registry allows to provide insights to clinicians and policy makers on the applicability of the DAPA HF findings to a contemporary population of HFrEF patients followed by cardiologists. It is reasonable to assume that the results of this analysis can be applicable to the entire SGLT2-ir class of drugs.
Introduction
Large randomised clinical trials (RCTs), real-world observational studies, and meta-analysis overall have shown that sodium–glucose cotransporter 2 inhibitors (SGLT2-i) reduce the risk of hospitalisation for heart failure (HF), cardiovascular mortality and the progression of chronic kidney disease (CKD) in a broad population of patients [Citation1–9] with HF. Their early and glucose-independent benefits suggest that physiopathology pathways of HF and CKD are effectively targeted [Citation10,Citation11], being the two comorbidities often interlinked [Citation12]. However, real-world epidemiology [Citation13,Citation14] can differ from randomised trials (RCTs), often limiting the transferability of novel evidences to clinical practice [Citation15]. This highlights the essential role of large well designed studies to assess cost-effectiveness [Citation16] as well as the replicability of RCTs results [Citation17] in different clinical settings.
This study aimed to assess the prevalence of DAPA-HF (Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure) [Citation4] eligibility criteria in a population of patients with HF and reduced ejection fraction (HFrEF) followed by cardiologists participating in the Italian Network on Heart Failure outcome registry (IN-HF) [Citation18].
Methods
The study cohort derives from the IN-HF registry, a nationwide prospective observational study conducted by 61 hospital cardiology institutions across Italy, enrolling chronic HF patients during routine outpatient visits. The design and main results have been published previously [Citation18,Citation19].
Patients gave written informed consent to anonymous handling of their data for research purposes, and local Institutional Review Boards of all participating centres approved the study according to national rules. Decisions for treatment, diagnostic and therapeutic procedures were left to the participating cardiologists. The investigation followed the principles outlined in the Declaration of Helsinki.
DAPA-HF is a prospective randomised placebo controlled clinical trial designed to evaluate the efficacy and safety of the SGLT2-idapagliflozin in patients with HFrEF, regardless of the presence of diabetes. The main results of this randomised controlled trial have been published elsewhere [Citation4].
To identify the study cohort for this applicability study, the inclusion and exclusion criteria of the DAPA-HF trial ( and Supplemental Table) have been partially applied to the IN-HF registry.
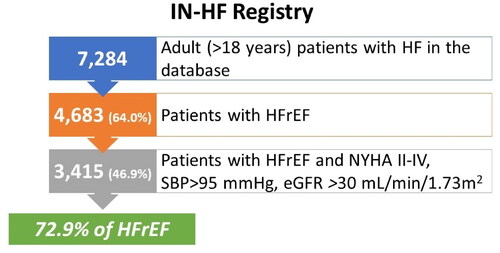
Figure 1. IN-HF outcome registry patient distribution before and after applying DAPA-HF inclusion and exclusion criteria.
The circulating levels of NT-proBNP required as an inclusion criterion in the trial were not considered because the rules of prescription of this drug stated by the regulatory authorities do not include such a measure (https://www.ema.europa.eu/en/documents/product-information/forxiga-epar-product-information_en.pdf).
Categorical variables are presented as percentages, whereas continuous variables are presented as their mean and standard deviation (SD), if normally distributed, or as median and interquartile range (IQR), if not. Categorical variables were compared by the χ2 test and continuous variables by the t-test or the Mann–Whitney U-test. The statistical comparisons have been performed between the DAPA-HF matched population and the non-matched DAPA HF population. Some comparisons of dichotomous variables between the matched population of IN-HF and that actually enrolled in the DAPA-HF trial have been performed. A p-value <0.05 was considered statistically significant. All tests were two sided. Analyses were performed with SAS system software (SAS Institute Inc., Cary, NC, USA).
Results
Of the 7284 adult patients with HF enrolled in the IN-HF outcome registry [Citation19], 4683 patients (64%) had a recorded diagnosis of HFrEF (LVEF ≤ 40%). After applying the inclusion and exclusion criteria of the DAPA-HF clinical trial (Supplemental Table), a total of 3415 out of 4683 (73%) patients resulted eligible for the DAPA-HF trial and have been included in this applicability study ().
Specifically, of the 1268 excluded patients 667 patients were excluded because in NYHA class I, 55 for Type 1 diabetes, 277 for a systolic blood pressure <95 mmHg, and 370 for an eGFR <30 mL/min/1.73 m2. One hundred and one patients had more than one reason for exclusion.
The main baseline demographics, clinical characteristics, and background therapies of the total IN-HF registry population and the two different subgroups of patients either eligible or not to DAPA-HF trial are reported in and summarised side-by-side also with the DAPA-HF population.
Table 1. Main baseline characteristics comparison between the in-HF outcome registry total population and the two subgroups derived from applying the inclusion and exclusion criteria of the DAPA-HF clinical trial, also reported.
Compared to the 1268 non-matching patients, the DAPA-HF matching population included relatively more >75 years old patients, a statistically significant higher proportion of systolic blood pressure >110 mmHg and of preserved renal function expressed by eGFR > 60 mL/min/1.73 m2, with a slightly higher frequency of obese patients. The DAPA-HF matching patients were also treated more frequently with diuretics, ARNI and MRAs as compared to the non-matching subgroup.
When compared with the 4744 patients from the DAPA-HF clinical trial, the matching subgroup of 3415 patients from the IN-HF registry overlapped for most of the baseline characteristics, however the IN-HF population was older, had less history of type 2 diabetes (p value <0.0001) and of heart failure of ischaemic aetiology (p value <0.001), and relatively more patients in NYHA II class (p value = 0.003), in a context in which the average EF was essentially the same. In this study, about 44% of patients had a history of hospitalisation for HF compared to about 47% in the DAPA-HF trial.
Discussion
HF is a major public health problem with a still growing socio-economic impact in Italy and worldwide, advocating for an immediate call-for-action [Citation19]. For decades there have been relatively little improvements in the medical treatment of this condition. However, consistent evidence has emerged for ARNI and, more recently, for SGLT2i, which were able to reduce the risk of HF hospitalisation, renal events, and cardiovascular mortality both in patients with and without type 2 diabetes, possibly driving a paradigm shift from the traditional treatment strategies in HF, unchanged for many years. Undoubtedly, the role of country specific observational research remains of paramount importance for pharmacovigilance, to monitor quality of care, to assess the dimension of the target population for a new drug (object of this specific study), to confirm the RCT’s evidence transferability, and to properly inform changes in guidelines and healthcare policies, including cost sustainability of novel treatments.
As a study limitation, the IN-HF registry network included cardiology centres only, hence the representativeness of our findings might not necessarily represent HF patients managed in other settings, such as primary care or other specialties. A recent article, describing the potential target population eligible for dapagliflozin in the setting of general practitioners and claims data, provided quite different figures [Citation20]. Once again the analysis of data provided by a specialist registry, such as IN-HF, demonstrates how relevant are the differences in patients’ populations followed by different healthcare professionals. However, the two epidemiological points of view provide complementary information, potentially useful for different stakeholders (i.e. general practitioners, cardiologists, regulatory authorities, payers).
Another limitation of this analysis is the lack of natriuretic peptide measures. Differently from another analysis on the same topic [Citation21], we did not consider NT-proBNP measures because this criterion was not considered by the European, and US Regulatory Authorities in their prescription rules.
Being IN-HF registry conducted just in the setting of Italian cardiology centres, the generalisability of the findings should be limited to this setting.
In any case, the availability of an easily accessible database from a nationwide prospective registry allowed us to quickly provide important insights, confirming the applicability and theoretically potential impact of the DAPA HF findings to a contemporary population of HFrEF patients followed by cardiologists in Italy. It is reasonable to assume that results of this analysis can be applicable to the entire SGLT2-inhibitor class of drugs.
High quality large registries, including a different kind of healthcare professionals and representative of the country-specific patients’ population, should be expanded even further to properly inform clinicians and policy makers supporting their evidence-driven initiatives and helping to reduce more effectively the epidemic-size spectrum of risk associated with cardiovascular, renal, and metabolism comorbidities.
Author contributions
All authors contributed equally to the critical evaluation and whole content of the manuscript. All the authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation. The Authors take full responsibility for the integrity and accuracy of the analyses.
Supplemental Material
Download MS Word (48.9 KB)Disclosure statement
MI, MM, MG, FO, LG, MG have no conflict of interest to disclose. PF is an employee of AstraZeneca and own shares from the company. APM, outside the present work, received personal fees for participation in study committees sponsored by AstraZeneca, Bayer, Fresenius, Novartis.
Additional information
Funding
References
- Zannad F, Ferreira JP, Pocock SJ, et al. SGLT2 inhibitors in patients with heart failure with reduced ejection fraction: a meta-analysis of the EMPEROR-Reduced and DAPA-HF trials. Lancet. 2020;396(10254):819–829. doi:10.1016/S0140-6736(20)31824-9.
- Barbarawi M, Al-Abdouh A, Barbarawi O, et al. SGLT2 inhibitors and cardiovascular and renal outcomes: a meta-analysis and trial sequential analysis. Heart Fail Rev. 2022;27(3):951–960. doi:10.1007/s10741-021-10083-z.
- Jhund PS, Solomon SD, Docherty KF, et al. Efficacy of dapagliflozin on renal function and outcomes in patients with heart failure with reduced ejection fraction: results of DAPA-HF. Circulation. 2021;143(4):298–309. doi:10.1161/CIRCULATIONAHA.120.050391.
- McMurray JJV, Solomon SD, Inzucchi SE; DAPA-HF Trial Committees and Investigators, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381(21):1995–2008. doi:10.1056/NEJMoa1911303.
- Packer M, Anker SD, Butler J; the EMPEROR-Reduced Trial Investigators., et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med. 2020;383(15):1413–1424. doi:10.1056/NEJMoa2022190.
- Kosiborod MN, Jhund PS, Docherty KF, et al. Effects of dapagliflozin on symptoms, function, and quality of life in patients with heart failure and reduced ejection fraction: results from the DAPA-HF trial. Circulation. 2020;141(2):90–99. doi:10.1161/CIRCULATIONAHA.119.044138.
- Anker SD, Butler J, Filippatos G; the EMPEROR-Preserved Trial Investigators., et al. Empagliflozin in heart failure with a preserved ejection fraction. N Engl J Med. 2021;385(16):1451–1461. doi:10.1056/NEJMoa2107038.
- Thorvaldsen T, Ferrannini G, Mellbin L, et al. Eligibility for dapagliflozin and empagliflozin in a real-world heart failure population. J Card Fail. 2022;28(7):1050–1062. doi:10.1016/j.cardfail.2022.04.011.
- Lam CSP, Karasik A, Melzer-Cohen C; CVD-REAL Investigators and Study Group., et al. Association of sodium-glucose cotransporter-2 inhibitors with outcomes in type 2 diabetes with reduced and preserved left ventricular ejection fraction: analysis from the CVD-REAL 2 study. Diabetes Obes Metab. 2021;23(6):1431–1435. doi:10.1111/dom.14356.
- Lopaschuk GD, Verma S. Mechanisms of cardiovascular benefits of sodium glucose co-transporter 2 (SGLT2) inhibitors: a state-of-the-Art review. JACC Basic Transl Sci. 2020;5(6):632–644. doi:10.1016/j.jacbts.2020.02.004.
- Joshi SS, Singh T, Newby DE, et al. Sodium-glucose co-transporter 2 inhibitor therapy: mechanisms of action in heart failure. Heart. 2021;107(13):1032–1038. doi:10.1136/heartjnl-2020-318060.
- Cherney DZI, Repetto E, Wheeler DC, et al. Impact of cardio-renal-metabolic comorbidities on cardiovascular outcomes and mortality in type 2 diabetes mellitus. Am J Nephrol. 2020;51(1):74–82. doi:10.1159/000504558.
- Groenewegen A, Rutten FH, Mosterd A, et al. Epidemiology of heart failure. Eur J Heart Fail. 2020;22(8):1342–1356. doi:10.1002/ejhf.1858.
- Maggioni AP, Orso F, Calabria S; ARNO Observatory., et al. The real-world evidence of heart failure: findings from 41 413 patients of the ARNO database. Eur J Heart Fail. 2016;18(4):402–410. doi:10.1002/ejhf.471.
- Averitt AJ, Weng C, Ryan P, et al. Translating evidence into practice: eligibility criteria fail to eliminate clinically significant differences between real-world and study populations. NPJ Digit Med. 2020;3:67. doi:10.1038/s41746-020-0277-8.
- Roberts MH, Ferguson GT. Real-world evidence: bridging gaps in evidence to guide payer decisions. Pharmacoecon Open. 2021;5(1):3–11. doi:10.1007/s41669-020-00221-y.
- Franklin JM, Patorno E, Desai RJ, et al. Emulating randomized clinical trials with nonrandomized real-world evidence studies: first results from the RCT DUPLICATE initiative. Circulation. 2021;143(10):1002–1013. doi:10.1161/CIRCULATIONAHA.120.051718.
- Tavazzi L, Senni M, Metra M; IN-HF (Italian Network on Heart Failure) Outcome Investigators., et al. Multicenter prospective observational study on acute and chronic heart failure: one-year follow-up results of IN-HF (Italian Network on Heart Failure) outcome registry. Circ Heart Fail. 2013;6(3):473–481. doi:10.1161/CIRCHEARTFAILURE.112.000161.
- The Heart Failure Policy Network. The Heart Failure Policy Practice in Europe. Italy. Available at: https://www.hfpolicynetwork.org/wp-content/uploads/Heart-failure-policy-and-practice-in-Europe-Italy.pdf. accessed 8 August 2022.
- Piccinni C, Dondi L, Calabria S, et al. How many and who are patients with heart failure eligible to SGLT2 inhibitors? Responses from the combination of administrative healthcare and primary care databases. Int J Cardiol. 2023;371:236–243. Epub 2022 Sep 27. doi:10.1016/j.ijcard.2022.09.053.
- Håkansson E, Norberg H, Själander S, et al. Eligibility of dapagliflozin and empagliflozin in a real-world heart failure population. Cardiovasc Ther. 2021 Dec 26;2021:1894155. doi:10.1155/2021/1894155.

