

Abstract
Background
Transcatheter aortic valve implantation (TAVI) with the SAPIEN 3 device has recently shown significant clinical benefits, compared to surgical aortic valve replacement (SAVR), in patients at low risk for surgical mortality (PARTNER 3 trial, NCT02675114). Currently in Belgium, TAVI use is restricted to high-risk or inoperable patients with severe symptomatic aortic stenosis (sSAS). This cost-utility analysis aimed to assess whether TAVI with SAPIEN 3 could lead to potential cost-savings compared with SAVR, in the low-risk sSAS population in Belgium.
Methods
A previously published, two-stage, Markov-based cost-utility model was used. Clinical outcomes were captured using data from PARTNER 3 and the model was adapted for the Belgian context using cost data from the perspective of the Belgian National Healthcare System, indexed to 2022. A lifetime horizon was chosen. The model outputs included changes in direct healthcare costs, survival and health-related quality of life using TAVI versus SAVR.
Results
TAVI with SAPIEN 3 provides meaningful clinical and cost benefits over SAVR, in terms of an increase in quality-adjusted life years (QALYs) of 0.94 and cost-saving of €3 013 per patient. While initial procedure costs were higher for TAVI compared with SAVR, costs related to rehabilitation, disabling stroke, treated atrial fibrillation, and rehospitalization were lower. The cost-effectiveness of TAVI over SAVR remained robust in sensitivity analyses.
Conclusion
TAVI with SAPIEN 3 may offer a meaningful alternative intervention to SAVR in Belgian low-risk patients with sSAS, showing both clinical benefits and cost savings associated with post-procedure patient management.
Introduction
The significant clinical benefits of transcatheter aortic valve implantation (TAVI) over surgical aortic valve replacement (SAVR) in patients with severe symptomatic aortic stenosis (sSAS) at intermediate and high surgical risk have been established several years ago [Citation1,Citation2]. Recently, the multicentre, randomised, controlled Placement of Aortic Transcatheter Valve Study (PARTNER) 3 trial has shown that TAVI using the SAPIEN 3 valve also provided meaningful benefits in patients with sSAS who were considered at low risk of surgical mortality, as demonstrated by a significant reduction in the composite outcome of death, stroke or rehospitalization at 1 and 2 years, compared with SAVR [Citation3,Citation4]. In addition, compared with SAVR at 30-days post-procedure, TAVI was associated with significantly lower rates of disabling stroke and new-onset atrial fibrillation (AF), shorter index hospitalisation duration, and better functional status and quality of life [Citation4]. No significant differences between the TAVI and SAVR groups were observed in major vascular complications, new permanent pacemaker implantations (PPI), or moderate or severe paravalvular regurgitation [Citation4].
The increased clarity on the clinical benefits of TAVI in patients with sSAS are reflected in the updated 2021 European Society of Cardiology (ESC)/European Association for Cardio-Thoracic Surgery (EACTS) guidelines, which recommend that TAVI is considered for all patients aged ≥75 years with sSAS regardless of surgical risk status, providing there are no clinical or anatomical barriers and suitable femoral access [Citation5]. As such, it is important to evaluate the implications on healthcare resources of potentially expanded TAVI use, in order to inform clinicians and policymakers. To date, cost-effectiveness analyses have been published for France [Citation6], Italy [Citation7], Spain [Citation8] and Germany [Citation9], and have shown economic dominance or cost-effectiveness of TAVI with SAPIEN 3 versus SAVR in patients with sSAS at low surgical risk. In Belgium, TAVI reimbursement is currently restricted to patients with sSAS who are considered inoperable or at high surgical risk. This differs from recent practice in other European countries, such as France and Germany, where TAVI use is expanding into the low-risk population, in line with European and national guidelines [Citation5,Citation10]. Furthermore, TAVI reimbursement in Belgium was limited to 500 inoperable/high-risk patients per year until April 2023 [Citation11,Citation12]. Effective 1st of May 2023, it increased by 3-fold up to 1 500 patients, which remains lower than the estimated annual number of potential TAVI candidates in Belgium under current indications of 1 976 patients, and much lower than the estimated 3 740 TAVI candidates including intermediate- and low-risk patients [Citation13]. Given the healthcare resource limitations and restricted TAVI access in Belgium, a cost-effectiveness analysis in the low surgical risk population may be beneficial for Belgian policymakers to assess unmet health benefits that could lead to improved resource allocation with potential cost savings. Therefore, we assessed the cost-effectiveness of TAVI with SAPIEN 3 versus SAVR in Belgian patients with sSAS at low surgical risk, using outcomes from the PARTNER 3 trial alongside country-specific clinical and economic cost data.
Methods
Model structure
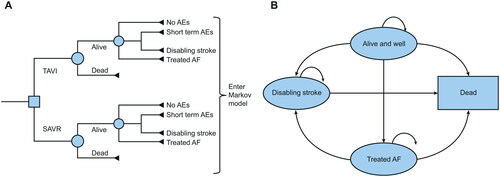
A cost-utility analysis was conducted to estimate changes in both direct healthcare costs and health-related quality of life with the use of TAVI with SAPIEN 3 compared with SAVR in sSAS patients with low risk of surgical mortality (Society of Thoracic Surgeons-Predicted Risk of Mortality [STS-PROM] score <4%) from the perspective of the Belgian National Healthcare Payer (RIZIV/INAMI + patient). Details of the two-stage model structure used to form the basis of the cost-utility analysis have been published previously [Citation6]. Briefly, adverse events (AEs) associated with the TAVI intervention were initially captured utilising the 30-days AEs dataset from the PARTNER 3 trial [Citation4] and entered into a decision tree that assigned patients to a range of AE outcomes () [Citation6]. The outcome data were subsequently fed into a Markov model that included four distinct health states (‘Alive and well’, ‘Treated AF’, ‘Disabling stroke’, and ‘Dead’) to capture longer-term patient outcomes after TAVI or SAVR intervention () [Citation6].
Figure 1. The cost-effectiveness model had two stages: (A) early AEs from the PARTNER 3 trial were captured in a decision tree, which fed into (B) a Markov model that captured longer-term outcomes of patients, with four distinct health states (reproduced from gilard M, et al. Value health 2021; https://doi.org/10.1016/j.jval.2021.10.003 under the terms of the creative commons licence (creative commons attribution license (CC by)). Clinical events were taken from the PARTNER 3 trial and from Belgian-specific literature sources when available and relevant. Costs were based on costing information from the Belgian APR-DRGs, regional tariffs and literature sources when relevant, and actualised to 2022 ( and Supplementary Materials). As there is no formal WTP threshold in Belgium, we adopted a cost-effectiveness ratio threshold of €30 000 per QALY gained. AE: adverse event; AF: atrial fibrillation; APR-DRG: All Patients Refined-Diagnosis Related Group; QALY: quality adjusted life years; SAVR: surgical aortic valve replacement; TAVI: transcatheter aortic valve implantation; WTP: willingness-to-pay.
We adapted the model for the Belgian context using cost data from the perspective of the Belgian National Healthcare System [Citation14]. Given that sSAS necessitates life-long valve replacement, a lifetime horizon was selected to reflect all potential consequences to individuals with sSAS over their lifetime, and applied discounting factors per year of 3% for future costs and 1.5% for future benefits based on the Belgian guidelines for economic evaluations and budget impact analyses [Citation14]. Health-related quality of life was included in the analysis using Quality Adjusted Life Years (QALYs) as an endpoint, measured using the EuroQol-5 Dimensions (EQ-5D) questionnaire for the four different health states in the model, with utility decrements taken from the published literature and adjusted for age and population norms according to Szende et al. [Citation15].
Model inputs
Trial overview
The PARTNER 3 trial (ClinicalTrials.gov number: NCT02675114) included patients with sSAS at low surgical risk of mortality (STS-PROM score <4%) [Citation4]. Patients were excluded if they had clinical frailty, bicuspid aortic valves, or other anatomical features that increased the risk of complications associated with either TAVI or surgery. Patients were randomised 1:1 to TAVI with SAPIEN 3 (n = 503) or SAVR (n = 497), with the “as treated” groups comprising 496 and 454 patients, respectively. The mean age of patients was 73 years, 69% were male, and the mean STS-PROM score at baseline was 1.9%. The primary endpoint was a composite of death from any cause, stroke, or rehospitalization at 1 year after the procedure.
Clinical events
In the base case, clinical events within one month after the procedure were based on PARTNER 3 outcomes (30-days AE dataset) [Citation4]. Monthly transition probabilities between health states for the Markov model, reflecting complications occurring after 3 days, were estimated based on outcome data up to 2 years from PARTNER 3 [Citation3,Citation4] or other literature sources where there were too few events in PARTNER 3 for reliable estimates (Supplementary Material, Table S1). The monthly probability of transition from ‘Alive and well’ to ‘Disabling stroke’ was estimated using Stroke Alliance For Europe (SAFE) data specific for Belgium [Citation16]. Due to the low number of stroke events in PARTNER 3, the transition probability from ‘Treated AF’ to ‘Disabling stroke’ was estimated from a large (n = 8 265) community-based study of AF in the Netherlands [Citation17]. Rehospitalization rates were based on outcomes in PARTNER 3 (using data up to 2 years) [Citation3,Citation4] and were assumed to remain constant over the time horizon of the model after 2 years. The probability of aortic reintervention due to valve deterioration was based on PARTNER 3 data up to 2 years [Citation3,Citation4] and then using data from a durability study on long-term outcomes of pericardial aortic tissue valve bioprothesis using the Carpentier-Edwards Perimount valve [Citation18].
The 2018 annual mortality risk per age (0–105+ years) and per gender was obtained from Belgian federal government data [Citation19] (Supplementary Material, Table S2). Data for years later than 2018 were not included in the base case due to potential influence by COVID-19 deaths. No Belgian-specific data were available, the hazard ratio (HR) of excess deaths from AF and disabling stroke were based on data from a systematic review and meta-analysis of 104 eligible cohort studies involving over 9.5 million participants [Citation20] and a community-based stroke register study in the UK [Citation21], respectively.
Cost inputs
The cost perspective was based on information from the Belgian All Patient Refined-Diagnosis Related Groups (APR-DRGs) and from published literature (). Costs were indexed to 2022 unless otherwise stated. For the base case, costs associated with TAVI and SAVR procedures were estimated from the APR-DRG 163 values for procedures on heart valves [Citation22], using data from the minor and medium severity categories as the best match for low-risk patients (covering 49.8% of the APR-DRG 163 procedure), with logarithmic transformation modelling according to Ishak et al. [Citation23] (Supplementary Material, Table S3). For TAVI, the cost of the SAPIEN 3 valve, indexed to 2022, was added. Due to an absence of robust Belgian data, costs for rehabilitation following TAVI and SAVR were based on the same detailed real-world national database analysis used in the French model adaptation [Citation6], indexed to 2022. Costs associated with health states, 30-days AEs (myocardial infarction, non-disabling stroke, transient ischaemic attack, bleeding, acute kidney injury), intercurrent events (myocardial infarction, transient ischaemic attack, bleeding), rehospitalization, and pacemaker implantation were estimated from APR-DRGs and/or published literature (). Reintervention costs were assumed to be equal to the combined costs of the initial procedure and rehabilitation associated with the procedure.
Table 1. Costs associated with TAVI and SAVR (procedure, complications, long-term).
Utilities
Age-adjusted population utility norms were used. An EQ-5D index value was used to document the population utility scores by age group [Citation15] specific to the Belgian population. Due to too few events in the PARTNER 3 trial, utility decrements were estimated using the published literature. Disabling stroke disutility was estimated based on a study reporting utility (EQ-5D) values in over 500 Belgian patients who had experienced a stroke [Citation29]. As Belgium-specific data were not available, the best source for estimating AF disutility was a French health economic study of the cost-effectiveness of oral anticoagulants in patients with AF [Citation32]. The estimated utility decrements for disabling stroke and AF of 0.388 and 0.121, respectively, were in line with values used in the model adaptation in other countries [Citation6,Citation7]. Disutility data were not included for intercurrent events in order to avoid a risk of double counting with the health state utilities applied to patients in the ‘treated AF’ and ‘disabling stroke’ states.
Model outputs
Details of the model outputs and assumptions have been published previously [Citation6]. All analyses were performed using Microsoft Excel (Microsoft Corporation, Redmond, WA). The model generated total per-patient costs and QALYs for each intervention over the patients’ lifetime, and an incremental cost-effectiveness ratio (ICER) for TAVI with SAPIEN 3 versus SAVR in Belgian low-risk patients with sSAS. As there is no official cost-effectiveness threshold in Belgium, a hypothetical willingness to pay (WTP) threshold of €30 000/QALY for sSAS intervention was assumed, as previously used in a study in Belgium [Citation33] and within the range of thresholds used for other countries in Europe [Citation6–9].
Sensitivity analyses
Uncertainty in the results was evaluated by performing one-way deterministic sensitivity analyses, whereby inputs were varied using confidence intervals and ranges from the literature where available. Overall parameter uncertainty was assessed by a probabilistic sensitivity analysis, whereby Gamma and Beta probability distributions were specified for all input parameters and 1 000 Monte Carlo simulations were run using random draws of all parameters from within their assigned distributions.
Scenario analyses
Multiple scenario analyses were conducted to assess the impact of changing various assumptions on the results of the model. These included the following scenarios, amongst others: more aggressive reintervention rate for TAVI; no survival benefit with TAVI; alternative PPI rates; alternative AF and disabling stroke disutility rates; identical rehabilitation rates between TAVI and SAVR; shorter time horizons than the lifetime horizon used in the base case.
Compliance with ethics guidelines
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Results
Base case
Compared with SAVR, TAVI with SAPIEN 3 was estimated to offer meaningful benefits through increased QALYs (incremental improvement of +0.94 per patient) at a reduced cost (–€3 013 per patient) over a lifetime horizon. As such, TAVI with SAPIEN 3 was determined to be dominant over SAVR in Belgium (). A detailed breakdown of costs revealed higher initial procedure costs for TAVI with SAPIEN 3 versus SAVR, but relatively lower costs related to rehabilitation, disabling stroke, treated AF, and rehospitalization (). An assessment of incremental cost per patient over time suggested that TAVI with SAPIEN 3 was cost saving compared with SAVR by Year 6 post-procedure (, and Supplementary Figure S1a). While the base case assumed a SAPIEN 3 valve cost of €19 610 (VAT included), cost-saving over the long term was estimated to be achievable with a valve cost of greater than €22 000, and a Year 1 cost-saving of TAVI with SAPIEN 3 over SAVR potentially could be achieved if the SAPIEN 3 valve were to cost €17 730 ( and Supplementary Figure S1c). Compared with SAVR, TAVI with SAPIEN 3 was associated with a steep increase in incremental QALYs per patient gained over time, up to a plateau of 0.94 QALYs per patient ( and Supplementary Figure S1b).
Table 2. Base case results with acute and lifetime costs.
Table 3. Change over time in (A) model outputs and (B) cost-saving assessments.
Table 4. Scenario analyses.
Sensitivity analyses
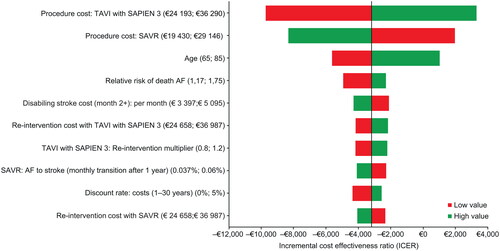
Univariate deterministic sensitivity analysis demonstrated that TAVI with SAPIEN 3 remains cost-effective, compared with SAVR, regardless of plausible changes in individual model parameters (). The model was most sensitive to the procedure costs of TAVI with SAPIEN 3, the starting age of patients entering the model, the relative risk of death from AF, and the discount rate.
Figure 2. Deterministic sensitivity analysis. Tornado diagram showing the 10 parameters with greatest influence on the model. AF: atrial fibrillation; ICER: incremental cost-effectiveness ratio; QALY: quality adjusted life years; SAVR: surgical aortic valve replacement; TAVI: transcatheter aortic valve implantation.
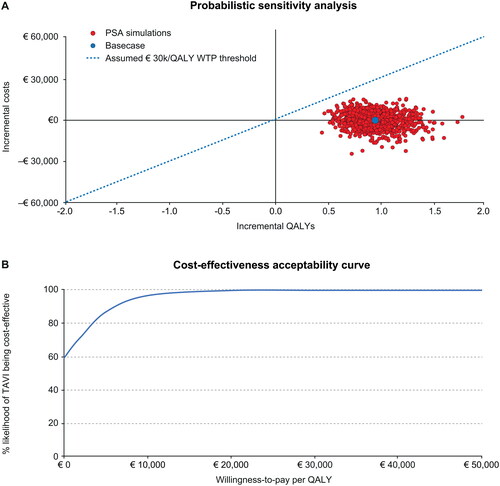
The results of the probabilistic sensitivity analysis confirmed the results of the base case analysis. The probability of TAVI being dominant over SAVR reached 52%. At the assumed WTP threshold of €30 000/QALY or higher, TAVI with SAPIEN 3 remained cost-effective over SAVR in 100% of simulations (). In addition, TAVI with SAPIEN 3 continued to show a 100% probability of being cost-effective over SAVR at a lower WTP threshold of €20 000/QALY ().
Figure 3. (A) Probabilistic sensitivity analysis. (B) Cost-effectiveness acceptability curve. QALY: quality adjusted life years; WTP: Willingness-to-Pay.
Scenario analyses
TAVI with SAPIEN 3 was dominant or cost-effective over SAVR across the wide range of scenarios conducted to assess the impact of changing various assumptions, including the scenario limiting the time horizon to 5 years (, Figure S1). These findings demonstrate the comparative robustness of the base case results.
Discussion
The findings of this cost-effectiveness analysis support that TAVI with SAPIEN 3 is likely to be a dominant intervention alternative to SAVR in Belgian patients with sSAS at low risk of surgical mortality. This result appeared to be driven by lower long-term management costs, particularly those associated with treated AF and disabling stroke, with cost-saving estimated to occur by Year 6 post-intervention. The initial lag before reaching cost-saving was likely due to the relatively higher initial procedure costs for TAVI with SAPIEN 3. Indeed, it was estimated that at Year 1 cost-saving could potentially be achieved if the SAPIEN 3 cost were reduced from the base case assumption of €19 610 to €17 730.
Furthermore, the base case modelling of cost-effectiveness of TAVI with SAPIEN 3 versus SAVR remained robust when considering a plausible WTP threshold in Belgium of €30 000/QALY (based on previous studies in Belgium and other European countries [Citation6–9,Citation33]), and remained robust despite multiple sensitivity analyses that stretched our model with various input modifications.
Adoption of TAVI is varied across European countries; for example, substantial differences are evident between Germany, France, and the UK [Citation38,Citation39]. Germany was an early and enthusiastic adopter of TAVI, with the procedure comprising 59% of aortic valve replacements in 2015, compared with 36% in France for the same year [Citation38,Citation40,Citation41]. Suggested factors contributing to the difference in TAVI numbers performed between European countries included variations in patient presentation and management of sSAS, and also differences in the healthcare systems [Citation38]. In Belgium, the healthcare system currently restricts TAVI reimbursement to 1 500 patients per year, which is substantially lower than the number of sSAS patients who may be eligible for TAVI based on the updated ESC/EACTS guidelines [Citation5]. This could suggest a potential under-valuing of TAVI as a management option for sSAS, perhaps partly due to concerns around cost. In the current study, scenario testing showed that, when considering a device price at parity with the reimbursement price from INAMI (either pre- or post-May 2023), TAVI was dominant over SAVR with an estimated potential cost-saving of around €10 000 per patient (, scenarios 15 and 16).
Our cost-effectiveness results were consistent with those reported for TAVI with SAPIEN 3 versus SAVR in other countries in the European Union. For example, TAVI with SAPIEN 3 was shown to be dominant over SAVR in low-risk patients with sSAS in France [Citation6,Citation42], and was cost-effective over SAVR in Italy (ICER/QALY of €2 989) [Citation7], Spain (ICER/QALY of €6 952) [Citation8], and Germany (ICER/QALY of €12 037) [Citation9]. TAVI with SAPIEN 3 has also been reported to be dominant over SAVR in low-risk patients in Norway [Citation43] and Ireland [Citation44], and cost-effective compared with SAVR in Australia (ICER/QALY of Aus$ 3 521) [Citation45] and Canada (ICER/QALY of Ca$ 27 196) [Citation46].
Our model could also provide convincing insight for “historical” intermediate and high-risk sSAS indications (as no specific randomised controlled trials with SAPIEN 3 exist in these populations as previous trials were conducted with earlier versions of the device). It is likely that the cost-savings component from our current analysis of TAVI versus SAVR in a low-risk population could be even greater in patient populations at intermediate or high risk of surgical mortality. Indeed, as surgical risk increases, the magnitude of clinical benefits of TAVI with SAPIEN 3 vs. SAVR is likely to increase, leading to potentially larger cost-savings and larger incremental QALYs.
In the current global economic environment, healthcare resources in many countries are increasingly limited and efficient healthcare resource utilisation is essential. At the same time, patients tend to prefer minimally invasive interventions as they are usually associated with a lower risk of complications and/or rehospitalization. The clinical benefits of TAVI with SAPIEN 3 in low-risk patients with sSAS have been established in PARTNER 3, which reported a lower risk of infection, fewer complications, and shorter hospital stays, compared with SAVR, whilst also improving patients’ quality of life [Citation3,Citation4]. The current analysis showed that TAVI with SAPIEN 3 is also potentially cost-effective over SAVR in the low-risk population, by offering a reduced impact on organisational aspects and resources (e.g. lower general anaesthesia) over the longer-term.
From the healthcare provider perspective, TAVI presents a capacity-enhancing innovation that also provides efficiencies by reducing healthcare resource use, post-surgical complications and hospital stays (including use of intensive care unit [ICU] beds). Reducing hospital stays allows higher patient intake capacity, which is an important consideration for health systems under high demand and with long waiting lists. Furthermore, these efficiencies could reduce the risk of infections and contamination within the hospital environment. TAVI also presents benefits by reducing the recovery period to resuming normal activity that might not be accounted for in this analysis. Further indirect benefits may include a reduced need for caregiver support and reduced impact on family, such as grand-child support.
In terms of organisational aspects, improving access to TAVI for Belgian sSAS patients in conjunction with latest European guidelines [Citation5,Citation47] recommending (class IA) low surgical risk sSAS patients eligible for the TAVI procedure, means that we can expect the number of TAVI implantations to increase in the future. Moreover, over time, it is likely that the TAVI procedure will be further simplified with shorter admission times, leading to a further reduction in the cost of the TAVI procedure [Citation48,Citation49]. Thus, this study provides additional information for Belgian healthcare providers and policymakers to consider when deliberating optimal management recommendations and healthcare resource allocation for patients with sSAS. In particular, consideration may be needed as to whether expanded endorsement of TAVI in Belgian to include the low surgical-risk population with sSAS could result in robust cost savings overall as well as additional patient benefits.
Limitations
This study has some limitations. Firstly, the results cannot be generalised to all patients with aortic stenosis as the PARTNER 3 trial excluded patients with clinical frailty, bicuspid aortic valves or other unsuitable anatomical features that increased the risk of complications post-intervention. Caution must also be exercised when attempting to generalise the findings from this model to populations outside Belgium. Furthermore, as this cost-utility analysis was based primarily on data from the PARTNER 3 study, the cost-effectiveness findings reported here cannot be generalised to other TAVI devices beyond the SAPIEN 3 device. Secondly, there are inherent limitations in any cost-effectiveness analysis including: assumptions made in the presence of ‘best fit’ data or paucity of data; extrapolations modelled for time horizons beyond the scope of existing input data; and the potential for under- and over-estimations as a result of differences in healthcare systems and/or the intervention and treatment selection criteria within a specific system. In the current model, it was assumed that the rate of rehospitalization, based initially on PARTNER 3 outcomes at 1- and 2-years, remained constant over the time horizon of the model after 2 years. The reintervention rate was also assumed to remain constant after 22 years, on the assumption that few patients (approximately 8%) would still be alive after this time, with limited need for reintervention. However, reintervention rates for younger patients could feasibly be higher than modelled, given uncertainty around the long-term durability of the latest generation of TAVI device. While longer follow-up is needed, current data at 5 years for the latest TAVI devices show no early signs of durability issues [Citation50]. To avoid a potential risk of double counting with the health state utilities applied to patients in the ‘treated AF’ and ‘disabling stroke’ states, disutility data were not included for intercurrent events; the few short-term cases of these AEs were assumed to have been treated successfully within 30 days without incurring any disutility. This assumption was considered conservative as, apart from pacemaker complications, intercurrent event rates were generally lower for TAVI with SAPIEN 3 compared with SAVR. Although only methodologically sound data from the literature that were considered the best available source were used to calculate some input data, in some instances (e.g. the utility decrement for AF) these data were based on non-Belgian patients.
Conclusions
The PARTNER 3 trial showed that TAVI provides significant clinical benefits over SAVR in patients with sSAS at low risk of surgical mortality [Citation3,Citation4], leading to updated European guidelines recommending consideration of TAVI in all patients with sSAS regardless of their surgical risk status [Citation5]. Guidelines in Belgium currently restrict TAVI to the population with sSAS who are inoperable or have a high risk of surgical mortality. This current analysis suggests that TAVI with SAPIEN 3 is likely to offer a cost-effective intervention in low-risk patients with sSAS in Belgium, showing economic dominance over SAVR driven by robust cost savings associated with post-procedure management of patients. These data may be helpful for informing clinicians, policymakers and healthcare budget holders in Belgium in their deliberations on how best to optimise both health outcomes and resource allocation in the management of patients with sSAS.
Medical Writing and/or editorial assistance
Writing support was provided by Vanessa Cobb of Zenith Healthcare Communications Ltd (Chester, United Kingdom), funded by Edwards Lifesciences.
Author contributions
The first draft of the manuscript was developed by PC, with editorial assistance provided by Zenith Healthcare Communications Ltd, UK. All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, provided critical revisions for important intellectual content, and approved the final version submitted for publication. All authors take responsibility for the integrity of the work as a whole. Christophe Dubois provided critical revisions for important intellectual content, and approved the final version submitted for publication.
Supplemental Material
Download MS Word (267.8 KB)Disclosure statement
Christophe Dubois is proctor for Edwards Lifesciences. PC is an employee of Edwards Lifesciences. All other authors have nothing to disclose.
Additional information
Funding
References
- Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363(17):1597–1607. doi:10.1056/NEJMoa1008232.
- Leon MB, Smith CR, Mack MJ, et al. Transcatheter or surgical Aortic-Valve replacement in Intermediate-Risk patients. N Engl J Med. 2016;374(17):1609–1620. doi:10.1056/NEJMoa1514616.
- Leon MB, Mack MJ, Hahn RT, et al. Outcomes 2 years after transcatheter aortic valve replacement in patients at low surgical risk. J Am Coll Cardiol. 2021;77(9):1149–1161. doi:10.1016/j.jacc.2020.12.052.
- Mack MJ, Leon MB, Thourani VH, et al. Transcatheter Aortic-Valve replacement with a Balloon-Expandable valve in Low-Risk patients. N Engl J Med. 2019;380(18):1695–1705. doi:10.1056/NEJMoa1814052.
- Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J. 2022;43(7):561–632. doi:10.1093/eurheartj/ehab395.
- Gilard M, Eltchaninoff H, Iung B, et al. Cost-Effectiveness analysis of SAPIEN 3 transcatheter aortic valve implantation procedure compared with surgery in patients with severe aortic stenosis at low risk of surgical mortality in France. Value Health. 2022;25(4):605–613. doi:10.1016/j.jval.2021.10.003.
- Mennini FS, Meucci F, Pesarini G, et al. Cost-effectiveness of transcatheter aortic valve implantation versus surgical aortic valve replacement in low surgical risk aortic stenosis patients. Int J Cardiol. 2022;357:26–32. doi:10.1016/j.ijcard.2022.03.034.
- Pinar E, García de Lara J, Hurtado J, et al. Cost-effectiveness analysis of the SAPIEN 3 transcatheter aortic valve implant in patients with symptomatic severe aortic stenosis. Rev Esp Cardiol (English ed). 2022;75(4):325–333. doi:10.1016/j.recesp.2021.02.006.
- Kuck KH, Leidl R, Frankenstein L, et al. Cost-Effectiveness of SAPIEN 3 transcatheter aortic valve implantation versus surgical aortic valve replacement in german severe aortic stenosis patients at low surgical mortality risk. Adv Ther. 2023;40(3):1031–1046. doi:10.1007/s12325-022-02392-y.
- Kuck K-H, Bleiziffer S, Eggebrecht H, et al. Consensus paper of the german society of cardiology (DGK) and the german society of thoracic, cardiovascular and vascular surgery (DGTHG) on catheter-assisted aortic valve implantation (TAVI) 2020. Kardiologe. 2020;14(3):182–204. doi:10.1007/s12181-020-00398-w.
- Federale Overheidsdienst Sociale Zekerheid. Ministerieel besluit tot wijziging van hoofdstuk "F. Heelkunde op de thorax en cardiologie" van de lijst en van de nominatieve lijsten, gevoegd als bijlagen 1 en 2 bij het koninklijk besluit van 25 juni 2014 tot vaststelling van de procedures, termijnen en voorwaarden inzake de tegemoetkoming van de verplichte verzekering voor geneeskundige verzorging en uitkeringen in de kosten van implantaten en invasieve medische hulpmiddelen. 2023. http://www.ejustice.just.fgov.be/eli/besluit/2023/03/27/2023010148/staatsblad
- Le Chapitre F, Service Public Federal Securite Sociale. Arrêté ministériel modifiant Chirurgie thoracique et cardiologie » de la liste et les listes nominatives jointes comme annexes 1 et 2 à l‘arrêté royal du 25 juin 2014 fixant les procédures, délais et conditions en matière d‘intervention de l‘assurance obligatoire soins de santé et indemnités dans le coût des implants et des dispositifs médicaux invasifs. 2023. http://www.ejustice.just.fgov.be/eli/arrete/2023/03/27/2023010148/moniteur
- Durko AP, Osnabrugge RL, Van Mieghem NM, et al. Annual number of candidates for transcatheter aortic valve implantation per country: current estimates and future projections. Eur Heart J. 2018;39(28):2635–2642. doi:10.1093/eurheartj/ehy107.
- Cleemput I, Neyt M, Van De Sande S, et al. Belgian guidelines for economic evaluations and budget impact analyses: second edition. KCE Reports. 2012.
- Szende A, Janssen B, Cabases J. Self-Reported population health: an international perspective based on EQ-5D. Dordrecht (NL): Springer Copyright; 2014.
- SAFE. Stroke Alliance For Europe. The burden of stroke in Belgium. 2017. https://www.safestroke.eu/wp-content/uploads/2017/12/SAFE_STROKE_BELGIUM.pdf
- Vermond RA, Geelhoed B, Verweij N, et al. Incidence of atrial fibrillation and relationship with cardiovascular events, heart failure, and mortality: a Community-Based study from The Netherlands. J Am Coll Cardiol. 2015;66(9):1000–1007. doi:10.1016/j.jacc.2015.06.1314.
- Bourguignon T, Bouquiaux-Stablo AL, Candolfi P, et al. Very long-term outcomes of the Carpentier-Edwards perimount valve in aortic position. Ann Thorac Surg. 2015;99(3):831–837. doi:10.1016/j.athoracsur.2014.09.030.
- StatBel. Mortality tables and life expectancy. 2022. https://statbel.fgov.be/sites/default/files/files/documents/bevolking/5.4%20Sterfte%2C%20levensverwachting%20en%20doodsoorzaken/5.4.3%20Sterftetafels%20en%20levensverwachting/sterftetafelsAE.xls
- Odutayo A, Wong CX, Hsiao AJ, et al. Atrial fibrillation and risks of cardiovascular disease, renal disease, and death: systematic review and meta-analysis. BMJ. 2016;354:i4482. doi:10.1136/bmj.i4482.
- Dennis MS, Burn JP, Sandercock PA, et al. Long-term survival after first-ever stroke: the oxfordshire community stroke project. Stroke. 1993;24(6):796–800. doi:10.1161/01.str.24.6.796.
- APR-DRG. TCT (Technical cell for the processing of the data related to the hospitals), "National database medical diagnosis/care & cost - Financial feedback by pathology: APR-DRG. 2020. https://tct.fgov.be/webetct/etct-web/national_data?lang=nl&menuSelected=apr_drg&selectedSideMenu=default&reset=true
- Ishak KJ, Stolar M, Hu MY, et al. Accounting for the relationship between per diem cost and LOS when estimating hospitalization costs. BMC Health Serv Res. 2012;12(1):439. doi:10.1186/1472-6963-12-439.
- De Smedt DM, Elseviers MM, Lins RL, et al. Economic evaluation of different treatment modalities in acute kidney injury. Nephrol Dial Transplant. 2012;27(11):4095–4101. doi:10.1093/ndt/gfs410.
- Elseviers MM, Lins RL, Van der Niepen P, et al. Renal replacement therapy is an independent risk factor for mortality in critically ill patients with acute kidney injury. Crit Care. 2010;14(6):R221. doi:10.1186/cc9355.
- Neyt M, Stroobandt S, Obyn C, et al. Cost-effectiveness of cardiac resynchronisation therapy for patients with moderate-to-severe heart failure: a lifetime markov model. BMJ Open. 2011;1(2):e000276–e000276. doi:10.1136/bmjopen-2011-000276.
- Pirson M, Di Pierdomenico L, Gusman J, et al. Evaluation of the cost of atrial fibrillation during emergency hospitalization. Acta Cardiol. 2013;68(5):469–474. doi:10.1080/ac.68.5.2994469.
- Van Brabandt H, Neyt M, Devos C. Catheter ablation of atrial fibrillation. Health Technology Assessment (HTA). Brussels. Belgian Health Care Knowledge Centre (KCE). KCE Reports 184. 2012. https://kce.fgov.be/en/publications/all-reports/catheter-ablation-of-atrial-fibrillation
- Dewilde S, Annemans L, Lloyd A, et al. The combined impact of dependency on caregivers, disability, and coping strategy on quality of life after ischemic stroke. Health Qual Life Outcomes. 2019;17(1):31. doi:10.1186/s12955-018-1069-6.
- Neyt M, Van Brabandt H, Van De Sande S, et al. Transcatheter Aortic Valve Implantation (TAVI): a Health Technology Assessment Update. Health Technology Assessment (HTA). Brussels. Belgian Health Care Knowledge Centre (KCE). KCE Report 163. 2011. https://kce.fgov.be/en/publications/all-reports/transcatheter-aortic-valve-implantation-tavi-a-health-technology-assessment-update
- RIZIV. Analysis of the distribution and evolution of medical practices in Belgium, in terms of volume and expenditure per insured, for 2021 - Pacemaker (1st implant). 2022.
- Lanitis T, Cotté FE, Gaudin AF, et al. Stroke prevention in patients with atrial fibrillation in France: comparative cost-effectiveness of new oral anticoagulants (apixaban, dabigatran, and rivaroxaban), warfarin, and aspirin. J Med Econ. 2014;17(8):587–598. doi:10.3111/13696998.2014.923891.
- Hettle R, Wouters H, Ayres J, et al. Cost-utility analysis of tiotropium versus usual care in patients with COPD in the UK and Belgium. Respir Med. 2012;106(12):1722–1733. doi:10.1016/j.rmed.2012.09.006.
- Makkar RR, Thourani VH, Mack MJ, et al. Five-Year outcomes of transcatheter or surgical Aortic-Valve replacement. N Engl J Med. 2020;382(9):799–809. doi:10.1056/NEJMoa1910555.
- Beyersdorf F, Bauer T, Freemantle N, et al. Five-year outcome in 18 010 patients from the german aortic valve registry. Eur J Cardiothorac Surg. 2021;60(5):1139–1146. doi:10.1093/ejcts/ezab216.
- Jacobs MS, de Jong LA, Postma MJ, et al. Health economic evaluation of rivaroxaban in elective cardioversion of atrial fibrillation. Eur J Health Econ. 2018;19(7):957–965. doi:10.1007/s10198-017-0942-2.
- Rapoport J, Teres D, Zhao Y, et al. Length of stay data as a guide to hospital economic performance for ICU patients. Med Care. 2003;41(3):386–397. doi:10.1097/01.MLR.0000053021.93198.96.
- Lutz M, Messika-Zeitoun D, Rudolph TK, et al. Differences in the presentation and management of patients with severe aortic stenosis in different european centres. Open Heart. 2020;7(2):e001345. doi:10.1136/openhrt-2020-001345.
- Mylotte D, Osnabrugge RL, Martucci G, et al. Adoption of transcatheter aortic valve implantation in Western Europe. Interv Cardiol. 2014;9(1):37–40. doi:10.15420/icr.2011.9.1.37.
- Nguyen V, Michel M, Eltchaninoff H, et al. Implementation of transcatheter aortic valve replacement in France. J Am Coll Cardiol. 2018;71(15):1614–1627. doi:10.1016/j.jacc.2018.01.079.
- Stachon P, Zehender M, Bode C, et al. Development and in-Hospital mortality of transcatheter and surgical aortic valve replacement in 2015 in Germany. J Am Coll Cardiol. 2018;72(4):475–476. doi:10.1016/j.jacc.2018.04.077.
- HAS-Sante. SAPIEN 3 treatment of severe symptomatic aortic stenosis in low-risk surgical patients in France 2021. https://www.has-sante.fr/upload/docs/application/pdf/2021-04/sapien3_9022021_avis_economique_vf2.pdf
- NIPH (Norwegian Institute of Public Health). Transcatheter aortic valve implantation (TAVI) versus surgical aortic valve replacement (SAVR) for patients with severe aortic stenosis and low surgical risk and across surgical risk groups: a health technology assessment. 2021. https://www.fhi.no/en/publ/2021/TAVI-vs-SAVR-for-patients-with-severe-aortic-stenosis-and-low-surgical-risk-and-across-surgical-risk-groups/
- HIQA (Health Information and Quality Authority). Health Technology Assessment of transcatheter aortic valve implantation (TAVI) in patients with severe symptomatic aortic stenosis at low and intermediate risk of surgical complications. 2019. https://www.hiqa.ie/sites/default/files/2019-12/TAVI_HTA.pdf
- Zhou JY, Liew D, Duffy SJ, et al. Cost-Effectiveness of transcatheter versus surgical aortic valve replacement in Low-Risk patients with severe aortic stenosis. Heart Lung Circ. 2021;30(4):547–554. doi:10.1016/j.hlc.2020.09.934.
- Tam DY, Azizi PM, Fremes SE, et al. The cost-effectiveness of transcatheter aortic valve replacement in low surgical risk patients with severe aortic stenosis. Eur Heart J Qual Care Clin Outcomes. 2021;7(6):556–563. doi:10.1093/ehjqcco/qcaa058.
- Beyersdorf F, Vahanian A, Milojevic M, et al. Erratum to: 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur J Cardiothorac Surg. 2022;61(4):964–964. doi:10.1093/ejcts/ezab557.
- Durand E, Tchétché D, Leroux L, et al. Multicenter cluster randomized controlled study evaluating the efficacy of an intervention aimed at reducing the length of stay after transfemoral transcatheter aortic valve implantation: the FAST-TAVI II study. EuroPCR. Paris, France. 2023.
- Frank D, Durand E, Lauck S, et al. BENCHMARK: a streamlined TAVI pathway with uncompromised safety in 28 european centers. EuroPCR. Paris, France. 2023.
- Pibarot P, Ternacle J, Jaber WA, et al. Structural deterioration of transcatheter versus surgical aortic valve bioprostheses in the PARTNER-2 trial. J Am Coll Cardiol. 2020;76(16):1830–1843. doi:10.1016/j.jacc.2020.08.049.

