
Abstract
Objective: This study aims at presenting the feasibility of using the public oral health clinics in indigenous Sámi communities, as arena for a comprehensive data collection for population-based epidemiological oral health research among adults (age, 18–75 years) in a multi-ethnic setting.
Material and methods: The study design was cross-sectional. The data collection was incorporated into the clinical procedure at six public dental clinics situated in the Administrative Area for the Sámi Language in Finnmark County, Northern Norway, during 2013–2014. Both clinical- and questionnaire-data were collected. The quality of clinical data was thoroughly calibrated and validated.
Results: Altogether, 2235 people participated in the study gave a crude response rate at 88.7%. In the final data sample (n = 2034), 56.9% were female. We constructed three ethnic groups (Sámi, Mixed Sámi/Norwegian and Norwegian). Altogether, 67.7% reported Sámi or mixed Sámi ethnicity. The internal validity of the clinical data was found to be satisfactory when assessed by comprehensive quality procedure, calibration and reliability assessments.
Conclusion: This study design and method assessments provide solid documentation that public dental clinics are suitable as arenas for data collection in epidemiological oral health studies in the Sámi population in this region.
Introduction
The Sámi people are an indigenous people primarily living in the northern part of Norway, Sweden, Finland and the Kola Peninsula in Russia. There is no direct means to estimate the number of Sámi in Norway due to the lack of ethnicity registries [Citation1] although it is assumed that Norway has the largest proportion of the total Sámi population [Citation2]. Sámi resides all over Norway, but the highest Sámi density is found in the areas north of the Arctic Circle and in the northern most county Finnmark in particular.
The research project The Dental Health in the North Study was initiated based on the Norwegian Government White Paper from 2006/2007 [Citation3] Tilgjengelighet, kompetanse og sosial utjevning – Framtidas tannhelsetjenester [Access, Competence and removing Social Gradients – The Future’s Dental Services], where concern was raised due to the lack of scientific knowledge on oral health in the adult Sámi indigenous population. Concern was also related to some indications, however not scientific based, on poorer oral health for the Sámi population in Northern Norway.
In general, there have only been conducted a few population-based studies on adults describing oral and dental health using epidemiological research methodology in Norway [Citation4–10]. Apart from a small study published as a report in 1988, where dental health data from 300 patients were collected in collaboration with public health clinics in Finnmark [Citation9], to the best of our knowledge, no epidemiological research focusing on oral health status in Sámi population has been conducted in Norway. However, studies among indigenous people worldwide have shown substantial oral health inequalities between these populations compared to reference populations [Citation11]. Challenges related to oral health among northern indigenous people have been actualized as well as the need for evidence as basis in oral health policy decisions in order to improve oral health for these populations [Citation12].
The concern raised in the mentioned White Paper [Citation3] was based on register-data on children (<18 years) from the Public Dental Services in Norway. These data showed clearly that dental health in Norway had improved; however, still large regional differences were revealed. The incidence of caries in children in the northernmost part of Norway i.e. the county of Finnmark has for long been the highest in the nation [Citation13]. There has also formerly been registered a higher prevalence of edentulousness among adults in this region (23 vs. 10% nation average), compared to the south of Norway [Citation14,Citation15]; however, recent data on the current situation among adults in the region have been lacking. Registry-based analysis on oral health among children in Finnmark county and one of the main Sámi core areas [Citation13] has shown that oral health in this region has improved remarkably during a 10-year period (2004–2014). This improvement was found in 5-, 12- and 18 years old. The proportion of children with no caries experience in this region is now close to the nation-average [Citation13].
In Norway, children and adolescents (up to 19 years) have access to free dental and oral health services. In addition, some prioritized groups (young adults up to 20–21 years; cognitive impairment, or persons with mental disorders; elderly; disabled or chronically ill; addicted to drugs, or imprisoned persons) are under given conditions, fully or partly covered under the social welfare systems. Nationally, the public dental clinics provide services to adults, only to a minor extent. This is mainly due to capacity limitations. Thus, private clinics are the main provider for oral health services to the Norwegian adult population; the service is paid out of pocket and relatively costly. However, in rural Finnmark county, private clinics are more or less absent. The public dental clinics in Finnmark were former known for being understaffed and affected by instability with high turnover of dentists, but the establishment of a new dentist school in 2004 at the Arctic University of Norway has started to contribute to the recruiting and stability of dentist with both local cultural and language competence at all dental clinics in Finnmark [Citation13].
In recent years, a few population-based surveys on oral health, with both questionnaire and clinical oral examination data, have been conducted in the region of Northern Norway like the THONN study (Tromstannen-Oral Health in Northern Norway) [Citation16] and The Tromsø Study [Citation17], where oral health was included as one of the several research topics in the data collection entitled Tromsø 7 conducted in 2015–2016. In the SAMINOR 2 study [Citation18], some questionnaire data on oral health were collected and have been published as two Master Theses in Public Health [Citation19,Citation20]. However, as mentioned no oral health study using clinical data has, to our knowledge, been conducted with the adult Sámi indigenous people in Norway as a target group.
As part of the methodological preparation and planning for the The Dental Health in the North Study, a pilot study was carried out in Finnmark in 2010, to test both questionnaires and the population’s willingness to take part in an epidemiological study focusing on oral health. The pilot study has been described elsewhere [Citation21]. People were recruited by postal invitation sent from UIT The Arctic University of Norway. Altogether, 34% answered and returned the questionnaires, and only 27% actually showed up for the clinical examination. Based on this experience, a need for improvement in the recruiting procedure was obvious, in order to improve participation by changing the arena for recruiting from an academic to health service institutions.
Using clinics and hospitals as arena for enrolling participants and using patients’ journal information as source for clinical data are, in general, common in epidemiological studies. To the best of our knowledge, in Norway there are no published population-based oral health study on adults where the data collection has been an incorporated part of the daily clinical routines at public dental clinics. Such study design can, however, have cost-effective benefits as well as quality improvements spin-off effects in the clinical work. The participation, representativeness as well as validity of clinical and questionnaire data need, however, to be carefully considered in such a study design.
The main purpose with this article has been to present and describe the method, data-collection procedure and participation in The Dental Health in the North Study. Because Sámi ethnicity has been the focus in this project, special attention has been on the ethnicity-data and ways of categorizing the participants into different ethnic groups. Finally, we aimed at illuminating the methodological strengths and weaknesses of using the Public Dental Services in Sámi communities as arena for such a comprehensive data collection for epidemiological oral health research.
Methods
Setting, study participants and ethics
As the focus for this research was oral health in the Sámi population, the municipalities of the Administrative Area for the Sámi Language within the Finnmark county in Northern Norway were selected as geographical area for the data collection (). The municipalities for the study were Tana, Nesseby, Porsanger, Karasjok and Kautokeino. These are all rural communities that are sparsely populated with a population size ranging from around 900 in Nesseby and up to 4000 in Porsanger, whereas the three others have close to 3000 inhabitants each. The Sami culture are strong in these communities and use of Sami language is common. Norway does not have ethnicity registry; however, population-based surveys conducted in these areas have shown that the majority in all these municipalities report Sami affiliation [Citation22].
Figure 1. Map of Norway. The municipalities included in the survey are marked in blue (Nesseby, Tana, Prosanger, Karasjok and Kautokeino).
During 2013–2014, all patients at the Public Dental Services in the selected municipalities between the ages 18–75 years old who were on the re-call list or had booked an appointment at any of the clinics during the data-collection period (dental check-up or treatment), were invited to participate in the ‘Tannhelse i nord’ study [Dental Health in the North study]. Information about the study and questionnaire were either sent out together with the clinics’ regular convene card or distributed upon arrival at the clinics. Information about the study were announced on the local radio station, to increase the awareness of the study and hence facilitate the recruitment of study participants.
The study was carried out with a cross-sectional epidemiological design. Both questionnaire information and clinical examination data were collected.
The study has been approved by the Regional Committees for Medical and Health Research Ethics (REC) in Norway (2012/1902/REK Nord). All participants gave their signed informed consent before inclusion in the study and they were informed that they could withdraw at any time without any reasons. The clinical examination was free of charge. Permission has been obtained from REC to store, until 2027, the identification key for follow-up studies or linkage to national registers for further oral health research purposes. However, separate approvals are required to conduct such new research activities.
Questionnaire
The four-page questionnaire included questions about background characteristics, socioeconomic status, oral health-related behaviours and oral health-related quality of life. Most of the questions included in the questionnaire have been used in population-based surveys. An overview of the themes included in the questionnaire is summarized in . The participants could choose either a Sámi or a Norwegian language version of the questionnaire. Most participants filled out the questionnaire before the clinical examination. All participants could, if needed, ask for help from the dental health personnel at each clinic on filling out the questionnaire or other questions related to the study.
Table 1. List of self-reported information collected in the questionnaire.
Questions on ethnicity
As this study aimed at investigation of oral health in the Sámi population, the self-reported questionnaire instrument on Sámi ethnic affiliation developed and used in the ‘Population-based study of health and living conditions in areas with both Sámi and Norwegian populations – the SÁMINOR study’ [Citation18,Citation23] was included in the questionnaire. Thus, the following questions were used in the questionnaire to collect data on ethnicity: ‘Which language do you/did you use at home?’, ‘Which language did your parents use at home?’, ‘Which language did your grandparents use at home?’ and ‘What do you consider yourself as?’. The response options were as follows: ‘Norwegian’, ‘Sámi’ and ‘Kven1’, or ‘Other, describe’ with the option to tick off more than one answer. Questions on the ethnic background of the respondents and the respondents’ parents had the same response options. Respondents were also asked about their self-perceived ethnicity; specifically, ‘What do you consider yourself as?’. For each of the above questions, respondents were allowed to provide more than one answer.
Ethnicity categorization
Based on the responses to these questions, three categories for ethnic affiliation were defined i.e. Sámi affiliation, Mixed Sámi-Norwegian and Norwegian.
The Sámi’ category represented those answering ‘Yes’ to the three following questions: ‘I consider myself Sámi’; ‘My ethnic background is Sámi’ and ‘My home language is Sámi’. Another sub-population termed Mixed Sámi-Norwegian represented those answering ‘Yes’ to either one or two (but not three) of the questions. All other respondents were categorized as Norwegian including respondents who reported use of the Sámi language by, or the Sámi ethnicity of, their grandparents or parents, but did not consider themselves to be Sámi, or reported that they did not have a personal Sámi background/home language. Responders who reported Kven ethnicity were merged with the Norwegian ethnicity due to low numbers.
Clinical and radiographic examination
A total of nine dentists and six dental hygienists with assisting nurses, at six Public Dental Services clinics (one in each municipality), examined all teeth except the third molar, and corresponding teeth surfaces clinically and radiographically. All personnel had long clinical experience, were highly motivated and had participated in workshops on clinical research methodology. Clinical measures collected in the study were previous dental treatment, dental caries and periodontal conditions. An overview of the clinical measures is summarized in . In addition, intraoral radiographs were taken, 2 or 4 bitewing depending on number of teeth and quality needs for analyses. The images where exported by Soredex Digora Optime intraoral X-ray reader. All clinical data were registered in a computerized protocol (OPUS dental 7.1.107) on a secured server.
Table 2. Overview of clinical parameters.
Caries registered in the clinics
A five-grade diagnostic scale [Citation29] was used to register caries severity radiographically on proximal tooth and occlusal surfaces not accessible for clinical examination. Caries grades 1–2 were denoted as enamel caries, and grades 3–5 as dentine caries. Caries on root surfaces and secondary caries were included in the registration of caries and all caries were registered at surface level. Missed and filled surfaces were also registered. Dental crowns were registered as filled surfaces. Decayed surface (DS), filled surface (FS), missed surface (MS), decayed and filled surface, decayed-, missed-, filled surface (DMFS), decayed teeth (DT), missed teeth (MT), filled teeth (FT), decayed and filled teeth and decayed-, missed- and filled teeth (DMFT) were calculated. Grades 3–5 lesions reaching into dentine were included in the DMF-scores, whereas grades 1 and 2 (enamel lesions) were assigned to initial caries and not included in the DMF-scores. The DMF index values were calculated by adding all ‘decayed’, ‘missing’ and ‘filled’ (due to caries) permanent teeth (DMFT)/surfaces (DMFS).
Post-clinic caries registration by X-ray and examiner calibration
To investigate reliability and consistency of the dental caries registration, an inter-examiner agreement was assessed post-clinically. The inter-examiner agreement for premolar and molar regions was estimated by comparing caries registrations from three examined participants, randomly chosen from the OPUS Journal software, from each examiners (15 in total). A calibrated examiner (A-KSB) was used as a Golden standard. Prior to the inter-examiner assessment, A-KSB was calibrated using a special designated software system for examiner calibration (DIL ver 1.21; University of Bergen, Bergen, Norway) and re-analyzed the radiographs. The DIL-calibration is based on the judgement of 51 occlusal and approximal surfaces on random radiographs. Two different exercises were performed on different tooth surfaces.
For the inter-examiner agreement analysis, the caries registration was categorized as ‘no caries’ (grades 1 and 2) and ‘manifest caries’ (grades 3–5). The Cohen’s Kappa value for each of the 15 examiners compared to the calibrated examiner (A-KSB) was calculated.
Periodontal parameters
Bleeding on probing (BOP) and periodontal probing depth (PPD) were assessed at six sites per tooth for all teeth (except the third molar). Periodontal probing depth was measured to the nearest millimetre with a periodontal probe, WHO-probe LM555B. Bleeding on probing was measured in conjunction with the periodontal probing. To improve and secure measurements and inter-examiner reliability, different precautions were taken. Prior to study start, all examiners were trained and calibrated towards an experience periodontist who was the gold standard (NO), regarding the diagnostic criteria and examination procedures including radiographic examination technique and periodontal pocket probing on one patient. The measurement with pocket probing was repeated for three teeth (six surfaces). In addition, each examiner received a diagnostic manual in which all measurements and the procedures for diagnostics were described.
Post-clinical measurement of bone levels
To be able to estimate the prevalence and severity of periodontitis, a categoric case definition was necessary. The case definition was based on a method used in a previous cross-sectional study [Citation30]. Hence, alveolar bone level (ABL) was measured on radiographs post-clinically on all participating patients by one experienced examiner (A-KSB). In addition, furcation involvement clearly visible on e-rays was registered (i.e. grades 2 and 3). The cervico-occlusal lengths of the crown, described by Bath-Balogh and Fehrenbach [Citation18] was used as reference marker. The distance from cementoenamel junction (CEJ) to alveolar crest (AR) was measured to the nearest, 0.5 mm. As only bitewing radiographs were available, mean root length values were used as described by Bath-Balogh and Fehrenbach [Citation31] to make it possible to estimate the relation between the total root length and ABL.
Prior to the measurements of radiographic ABL, the examiner (A-KSB) was trained by an experienced periodontist (NO) and an inter-examiner agreement was conducted. In addition, A-KSB did an intra-examiner agreement. Bitewing-radiographs from 10 study-participants were randomly selected and the distance from the CEJ to the AC was measured. All post-clinical data were registered using Microsoft Excel 2013, and the classification of severity of disease was calculated.
Data managing and the final data set
The questionnaire and informed consents were sent to the study coordinator who consecutively punched the questionnaire data into an excel file as the questionnaires were received. All the punched questionnaire-data as well as the OPUS ID versus questionnaire ID were controlled once.
Each questionnaire had a unique id-number. At the clinics, lists were made with these id numbers and each participant corresponds to the medical record number based on the computerized medical record system, OPUS. The OPUS data and questionnaire data were punched and stored in computers disconnected to the Internet, during the whole data-collection period. Backups and the computer were locked in when they were not in use.
Information on age and gender were manually obtained for each participant from OPUS and registered in the data file after the main data collection was completed and the questionnaire data and OPUS data were merged. Age was rounded off to the nearest year.
Local involvement
Through all stages in the research project’s planning and data collection, representatives from the administrative unit of the Public Dental Services in the region worked closely with the research group. Seminars/workshops were arranged before, during and after the data collection. At these gatherings, the recruiting of participants, data collection procedures and the content of the questionnaire were thoroughly discussed with the employees at the participating clinics, as well as the cost-benefits for the clinics and the workers were involved. Based on the initiative from workers at the dental clinics at such a workshop, questions on use of e.g. traditional healers as pain management were developed and included in the questionnaire. These workshops were also valuable, together with the local dental health workers, to make strategies for recruiting participants to the study. The seminars/workshops also included lectures on general epidemiological research design, and research methodology for oral health studies in particular. In addition, information and process evaluation of the on-going data collection were the focus in these seminars.
After the data collection was completed and validated, preliminary clinic-wise results were presented at a workshop for the employees at the clinics. In this meeting, the use of the ethnicity data was in particular a topic and the local health workers were invited to give input on how ethnic classifications should be handled in the analysis.
Statistics
Stata/MP 15.0 for Windows (StataCorp LLC) was used for the statistics presented in this article. Due to the nature and scope of this article, only descriptive statistics were presented. The agreements were calculated by utilizing Cohen’s kappa (κ) and Intraclass Correlation Coefficients (ICC) values in SPSS.
Results
Participation
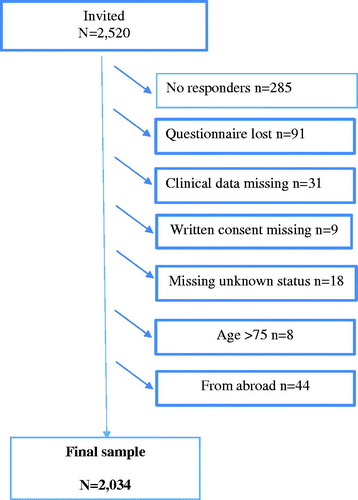
In total, out of 2520 invited 2235 of the adult patients (age, 18–75 years) who had an appointment at, or came to any of the six clinics during the data-collecting period, participated in the study, giving a crude response rate at 88.7%.
As shown in , 157 participants were not included in the final sample due to questionnaire data, clinical data or both were missing, not within the target age, or missing written content, or could not be accounted for and thus given missing unknown status. Participants who reported a foreign ethnicity and who did not report Norwegian, Kven or Sámi ethnicity were excluded. The final sample consisted of 2034 participants.
Figure 2. Flowchart of the study sample and participation.
summarizes the participation by municipality units. The municipality of Porsanger had a considerably larger portion of no-responders compared to the rest of the clinics. The participants from Nesseby constituted only 4% of the total sample. The contribution from the other municipality ranged from around 20 to 28% of the total sample. The response-rate ranged from 70.6 to 100%.
Table 3. Participation by municipality.
Characteristics of the study sample
In , selected characteristics for the study sample are summarized. One quarter of the sample was below the age of 38 years. More women participated than men. Nearly, 30% of the study sample reported a household gross annual income above NOK 750,000 and about 10% reported gross annual income below NOK 300,000. Slightly above 60% of the sample reported more than 12 years of education. The majority of the study sample (54%) reported to be in fulltime occupation. Around 14% of the study sample reported not living in the County of Finnmark at the age of 10 years. Three quarters (76%) of the participants in the study reported Sámi affiliation.
Table 4. Selected characteristics for the study sample n = 2034b.
The majority of the sample reported a full-time income (54%), about one-tenth reported being on any kind of welfare-income and the sample consisted of 85 students (4%). Based on the question on occupation altogether 131 participants (6.4%) reported being self-employed within the reindeer herding industry.
Altogether, 91% of the participants reported that time since last visit to the dental clinic was <3 years and slightly more than half of the participants reported <1 year since last visit.
Inter-examiner agreement
Caries registration
Result of the inter-calibration with the software was κ = 0.67 for the first data set, and κ = 0.70 for the second. The mean κ for all 15 examiners compared to the golden standard (A-KSB) was κ = 0.84 (range, 0.55–1.0).
Periodontal pocket probing and measurement of distance from CEJ to AC
The inter-examiner agreement on ABL measurement on radiographs was κ = 0.97 and the intra-examiner reliability was κ = 0.95.
Ethnicity
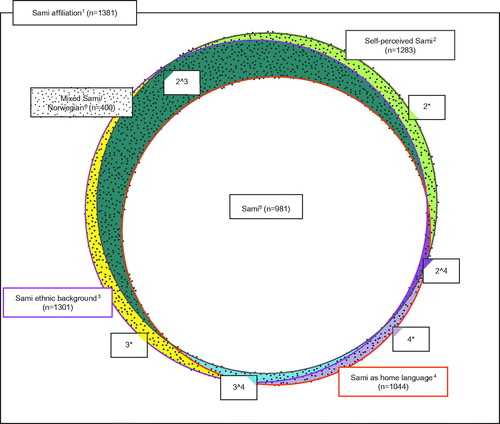
sumaarizes the distribution of answers on the ethnicity-related questions by our defined three ethnic groups Sámi, Mixed Sámi/Norwegian and Norwegian. In total, 1381 (67.9%) of the participants reported some Sámi affiliation, and out of these, 981 participants (71.0%) reported Sámi as home language, considered themselves to be Sámi with Sámi ethnic background and reported Sámi self-perceived belonging. These were defined as belonging to the ethnic category ‘Sámi’ (n = 981). Altogether, 400 of the participants reported ‘Yes’ to either one or two (but not three) of the questions ‘I consider myself Sámi’; ‘My ethnic background is Sámi’ or, ‘My home language is Sámi’ and thus belonging to the ethnic category Mixed Sámi-Norwegian. Most participants in this category (n = 236; 59%) reported Sámi ethnic background and self-perceived Sámi ethnicity, but not Sámi as home language, shown as the area 2^3 in ; where the distribution of sub-populations among participants with Sámi affiliation and the degree of overlap between these groups are shown.
Figure 3. Distribution of sub-populations among participants with Sámi affiliation: The Dental Health in the North Study. 1 Sámi affiliation is defined as Sámi language being spoken at home by at least one of the grandparents, parents or the respondent, or Sámi ethnic background reported for respondent or a parent, or that the respondent considers himself/herself as Sámi (n = 1381). 2 Self-perceived Sámi is defined as yes to the question: I consider myself Sámi (n = 1283). 3 Sámi ethnic background is defined as yes to the question: My ethnic background is Sámi (n = 1301). 4 Sámi as home language is defined as yes to the question: My home language is Sámi (n = 1044). 5 Answered yes to all three questions in footnote: 2, 3 and 4 (n = 981). 6 ‘Mixed Sámi/Norwegian’ is defined as yes to one or two of the question(s) in footnote 2 or 3 or 4 (2*+3*+4*+2∧3 + 2∧4 + 3∧4) (n = 400). 2*: Reported only self-perceived Sámi (n = 48). 3*: Reported only Sámi ethnic background (n = 53). 4*: Reported only Sámi as home language (n = 14). 2∧3: Reported Sámi ethnic background and self-perceived Sámi (n = 236). 2∧4: Reported self-perceived Sámi and Sámi as home language (n = 18). 3∧4: Reported Sámi ethnic background and Sámi as home language (n = 31).
summarizes self-reported ethnicity, self-perceived ethnicity and language at home according to our ethnic definition. All defined as belonging to the Sámi group consider themselves as Sámi and of Sámi ethnicity and had Sámi language as home language. The ‘Mixed Sámi/Norwegian’ group had strong affiliation to both Sámi and Norwegian ethnicity (80.0%; 58.0%) and self-perceived Sámi, and Norwegian ethnicity (75.5%; 66.3%), but few Sámi in the ‘Mixed Sámi/Norwegian’ had Sámi as home language (15.8%) and 87.3% with Norwegian as home language. In this latter group, one out of seven reported Kven ethnicity.
Table 5. Self-reported ethnicity, self-perceived ethnicity and language at home according to our ethnic definition.Table Footnotea
Discussion
To increase knowledge about oral health conditions in the indigenous population in the circumpolar areas, a development of good epidemiological research designs with high methodological quality is required. Local ownership and participatory models in the planning, implementation and interpretation of results are all essential elements to achieve reliable and valid data.
This study has several methodological strengths. In summary, these advantages are as follows. First, the external validity of the results is likely to be strong, due to the high participation rate. Second, the comprehensive questionnaire with questions and established instruments used in other population-based surveys, and questions of particular cultural relevance for the Sámi population provide data for analysis of a broad spectra of predictors for oral health. The collected data can thus be analyzed from a cultural relevant perspectives, and in relation to other comparable investigations for comparison purposes. The linkage of both questionnaire data and dental record is considered of great methodological benefit. Finally, the test for reliability and calibration assessments done on the clinical data showed satisfactory accuracy in the measurements.
The indigenous Sámi population’s oral health conditions were an essential focus in this study. Ethnicity is, however, a complex phenomenon. It has both objective and subjective dimensions [Citation32]. To measure ethnicity, at least some reasonable indicators of each one of these dimensions are needed. Objective aspects are those that can be observed as facts, including that of kinship, descent and spoken language. Subjective approaches refer to subjective dimensions as attitudes, values and feeling of belonging at the individual level. In our definition of the Sámi, we used both objective and subjective criteria to define Sámi ethnicity. To be categorized into ‘The Sámi’ group, the participants reported on an objective level Sámi kinship (parents, grandparents being Sámi) and Sámi language spoken at home, together with subjective feeling of belonging to the Sámi culture (subjective Sámi criteria). This group had, so to speak, a very strong Sámi ethnicity. ‘The mixed Sámi/Norwegian’ group had a multiple ethnic identity with individual’s identification to both the society at large and Sámi and Kven ethnicity. ‘The Norwegian’ group were manly Norwegians, including Kven affiliation (n = 99) (without Sámi affiliation) and Sámi with some affiliation, but without subjective Sámi criteria (n = 165). Those respondents reported use of the Sámi language or ethnicity for grandparents and/or parents, but did not consider themselves to be Sámi or personally consider they were having a Sámi ethnic background or had Sámi as home language. This group reported similar ethnic characteristics as the Norwegians (93.3% reported Norwegian ethnicity; 97.0% reported self-perceived Norwegian ethnicity and 99.4% reported Norwegian as home language, data not shown) and therefore we merged them with the Norwegians.
Due to its diverse nature, both the classification of ethnicity and its use as an independent variable in epidemiological research are complex and have been described as controversial [Citation2,Citation33]. Thus, for future analysis and work based on this data collection, we recommend ethnic categorizations to be created in line with and transparently explained for each research theme/question under study.
We achieved a remarkable high participation rate. The external validity of the study could still be questioned due to the fact that the eligible for the study where those in contact with the public dental clinic during the data-collection period. The question is whether the population who attended the clinics reflects the population, in general. The proportion of the population regularly attending the public clinics in these municipalities is likely to be high because, except for one municipality (Porsanger), there are no private clinics, unless crossing the border to Finland or going to larger towns in the region. Nationally about 70% of the adult population report using the dental clinics at a regular basis [Citation34]. Unpublished data from the SAMINOR 2 study [Citation18], 83% of the adult population reported using dental clinics regularly, among study participants living in the core area for Sámi settlement. In a recent epidemiological population-based study conducted in Northern Norway, about 67% of the adult population reported dental attendance at least every other year. However, in that study the youngest participants (<35 years) reported least regular attendance (50%), whereas about 72% of the older participants (35–79 years) reported regularly dental attendance [Citation35].
As summarized in , more than 90% of the participants had been to the clinic during the last years, thus indicating that the actual participants in the study, to a large extent, represented the part of the population attending the clinics frequently. It is likely that the proportion of the population not or seldom attending the dental clinic could differ with respect to oral health, lifestyle and oral health-related behaviours compared to the regular attenders. That non-attendees differ from participants in epidemiological surveys are well known [Citation36]. Because the general adult population in Norway is not prioritized under the legislation on dental health care, dental care can be costly. As such, one may expect social inequality in oral health status and in the use of dental health services, as they have been observed in other aspects of health [Citation37,Citation38].
We experienced in the former mentioned pilot study conducted in Finnmark [Citation21] that participation was very low when posting an invitation directly from the research institution to the general population with a questionnaire and invitation to come for an oral health check (<30%). Response rate in population-based oral health projects conducted in recent years in Scandinavia whit similar recruitment approach as our pilot have been reported at around 50–68% [Citation16,Citation30]. In the five municipalities where our study was conducted, only one private clinic was available. Thus, the Public Dental Services are the only accessible unless going abroad for oral health treatment; however, the extent of this is unknown.2 This situation where the majority of the adult population is covered by Public Dental Services (as paying patients), is somewhat unique for this northern region in Norway. This was one of the main reasons why we decided to change the recruitment procedure from the pilot to the main study, by using the local public dental clinics (and not the UiT The Arctic University of Norway) as the arena for recruiting participants.
Advantages of the study design are related to local ownership, credibility and cultural sensitivity. The large majority of employees at the clinics were from the local communities and all clinics had Sámi-speaking health workers. More than half of the employees were of Sámi ethnicity (16 out of 29) (personal communication, A-KSB December 2018). In this perspective, the dental clinics represent institutions with strong ties to the local communities and the Sámi population. However, these listed advantages could also be viewed at as potential weaknesses as our recruiting lays more to the convenience sampling procedure where people easy to reach are invited. This, in combination with social desirability bias where people tend to participate based on loyalty or report in line whit what are assumed favourable, could have affected both the external and the internal validity of our study. In this perspective, an ethical awareness on the implications of recruiting individuals to a research project in a setting where health treatment is being sought, is essential.
Local involvement, like enrolling the data collection into daily clinical work at the clinics and inviting the employees to take part in all parts of the project journey, could cause positive spin-off effects for the included clinics. Especially related to quality improvements in the clinical routine-work, but also local capacity building related to increased knowledge and skills on how to do epidemiological oral research. These likely benefits must, however, be viewed at in relation to any potential extra work burden for the clinics involved.
The internal validity of the clinical data has shown to be satisfactory based on the comprehensive calibration, reliability assessments and quality procedure thoroughly described in our study. These method assessments provide solid documentation that public dental clinics are suitable as arenas for data collection in epidemiological oral health studies in the Sámi population in this region. We do recommend that this approach can be considered in epidemiological studies in other communities, provided a broad population coverage for the public oral health clinics and a tradition of frequent visits to the Public Dental Services.
As summarized in , the questions in the questionnaire have been used in other oral health studies in the Nordic countries and some are based on well-established scale instruments like the Q36 Oral health related quality of life (OHIP-14) and Q37 Dental anxiety scale. Both scales have been validated in a Norwegian context and found to be satisfactory [Citation28,Citation39]. However, the questionnaire was not validated in the Sámi population prior to the study. Nor was the Sámi version of the questionnaire back translated in the traditional way, but workers at the clinics critically reviewed the questionnaire at workshops together with the research-team in charge of the study, and gave their input before the final questionnaire was settled.
Conclusion
In conclusion, our study has shown that enrolling and incorporating an epidemiological data collection into public dental clinics daily work routines was feasible and gave clinical data with satisfactory level of validity. We have presented a transparent way of creating ethnic categories for use in further analysis on dental health.
The outlined potential challenges related to the external validity, specifically the calibration of a high number of examiners must be taken into consideration when interpreting the data in a population perspective. The study is the first in its kind, providing questionnaire and clinical data on oral health from a Sámi population attending the Public Dental Services in Norway. Given the majority of the population do attend dental health services regularly, the methodological advantages described indicate that this study will be of great value for further analytical approaches to investigate the predictors for oral and dental health in the Sámi population.
In general, we recommend that relevant representatives from the involved ethnic groups are invited to take part in the process from planning to the interpreting of the results in epidemiological research where ethnicity is a variable. When questionnaire data are developed, concerns related to cultural sensitive issues, especially when life-style related questions are included, must be validated in relevant fora with adequate representations. Finally, potential selection and information bias caused by conducting data collection in a setting where the study participants initially are searching health services and help must be carefully addressed.
Acknowledgements
The authors want to thank Torill H. Lauritsen (Dental Manager for Public Dental Services, Finnmark County Council), Anne-Line Trøften (Over Dentist in Central Finnmark), Lasse Hove (Over Dentist in West Finnmark), Ann-Karin Pilskog Olsen (Dental Hygienist, North Cape, Finnmark), all staff at the participating public dental clinics in Finnmark, and last but not least our gratitude goes to all the patients who participated in the study.
Disclosure statement
The authors report no conflict of interest.
Notes
Additional information
Funding
Notes
1 Kven is an ethnic minority group in Norway. They descended from Finnish farmers and fishermen who emigrated from the northern parts of Finland and Sweden to Northern Norway from the 16th to 19th centuries. In 1996, the Kvens were granted minority status in Norway, and in 2005 the Kven language was recognized as a minority language in Norway.
2 For this geographical area, the use of dental care services in Finland (most of these municipalities are located near the Finish border), due to lower costs is a relevant issue, but the extent of this is also unknown.
References
- Sønstebø A. Samisk statistikk 2018 [Sami Statistics 2018]. Oslo-Kongsvinger: Statistics Norway (SSB); 2018.
- Pettersen T, Brustad M. Which Sami? Sami inclusion criteria in population-based studies of Sami health and living conditions in Norway – an exploratory study exemplified with data from the SAMINOR study. Int J Circumpolar Health. 2013;72:21813.
- St.meld. nr. 35 (2006-2007). Tilgjengelighet, kompetanse og sosial utjevning – Framtidas tannhelsetjenester. Oslo: Det kongelige helse- og omsorgsdepartemen; 2007.
- Holst D. Oral health equality during 30 years in Norway. Community Dent Oral Epidemiol. 2008;36:326–334.
- Holst D, Schuller AA. Equality in adults’ oral health in Norway. Cohort and cross-sectional results over 33 years. Community Dent Oral Epidemiol. 2011;39:488–497.
- Schuller AA, Holst D. Changes in the oral health of adults from Trøndelag, Norway, 1973-1983-1994. Community Dent Oral Epidemiol. 1998;26:201–208.
- Skudutyte-Rysstad R, Eriksen HM. Changes in caries experience among 35-year-old Oslo citizens, 1973–2003. Acta Odontol Scand. 2007;65:72–77.
- Skudutyte-Rysstad R, Eriksen HM, Hansen BF. Trends in periodontal health among 35-year-olds in Oslo, 1973-2003. J Clin Periodontol. 2007;34:867–872.
- Evjen G, Holst D. Levekår og tannhelse i Finnmark: en rapport fra et samarbeidsprosjekt mellom Den offentlige tannhelsetjeneste i Finnmark og Institutt for samfunnsodontologi. Oslo: Institutt for samfunnsodontologi, Universitetet i Oslo; 1988.
- Gulcan F, Nasir E, Ekback G, et al. Change in oral impacts on daily performances (OIDP) with increasing age: testing the evaluative properties of the OIDP frequency inventory using prospective data from Norway and Sweden. BMC Oral Health. 2014;14:59.
- Mejia GC, Parker EJ, Jamieson LM. An introduction to oral health inequalities among Indigenous and non-Indigenous populations. Int Dent J. 2010;60:212–215.
- Schroth RJ. The state of dental health in the north. Int J Circumpolar Health. 2006;65:98–100.
- Brustad M, Lauritsen TH. Tannhelse i samisk befolkning i Finnmark. Den Norske Tannlegeforenings Tidende. 2015;125:966–970.
- Evjen G, Holst D. Levekår og tannhelse i Finnmark: en rapport fra et samarbeidsprosjekt mellom Den offentlige tannhelsetjeneste i Finnmark og Institutt for samfunnsodontologi. Oslo: University of Oslo; 1988.
- Holst D, Grytten J. Overkommelige tannlegeutgifter for de fleste. Samfunnsspeilet. 1997;3:36–40.
- Holde GE, Oscarson N, Tillberg A, et al. Methods and background characteristics of the TOHNN study: a population-based study of oral health conditions in northern Norway. Int J Circumpolar Health. 2016;75:1–7.
- Jacobsen BK, Eggen AE, Mathiesen EB, et al. Cohort profile: the Tromso Study. Int J Epidemiol. 2012;41:961–967.
- Brustad M, Hansen KL, Broderstad AR, et al. A population-based study on health and living conditions in areas with mixed Sami and Norwegian settlements – the SAMINOR 2 questionnaire study. Int J Circumpolar Health. 2014;73:23147.
- Vakulenko I. Aspects of self-reported oral health among adults in selected municipalities in Northern- and Mid-Norway. A cross-sectional study. Based on material from the SAMINOR-2 study. Tromsø: UiT the Arctic University of Norway; 2016.
- Teterina A. Self-reported oral health. A cross sectional study in the municipalities with mixed Sami and Norwegian population in Northern and Mid-Norway. [Master in MPH]. Tromsø: UIT the Arctic University of Norway; 2018.
- Adekoya SM, Brustad M. Oral health of adults in northern Norway – a pilot study. Nor J Epidemiol. 2012;22:31–38.
- Broderstad AR, Melhus M, Lund E. Iron status in a multiethnic population (age 36–80 yr) in northern Norway: the SAMINOR study. Eur J Haematol. 2007;79:447–454.
- Lund E, Melhus M, Hansen KL, et al. Population based study of health and living conditions in areas with both Sámi and Norwegian populations-the SAMINOR study. Int J Circumpolar Health. 2007;66:113–128.
- Doring N, Hansson LM, Andersson ES, et al. Primary prevention of childhood obesity through counselling sessions at Swedish child health centres: design, methods and baseline sample characteristics of the PRIMROSE cluster-randomised trial. BMC Public Health. 2014;14:335.
- Ajzen I. The theory of planned behaviour: reactions and reflections. Psychol Health. 2011;26:1113–1127.
- Buunk-Werkhoven YA, Dijkstra A, van der Schans CP. Determinants of oral hygiene behavior: a study based on the theory of planned behavior. Community Dent Oral Epidemiol. 2011;39:250–259.
- Dahl KE, Wang NJ, Skau I, et al. Oral health-related quality of life and associated factors in Norwegian adults. Acta Odontol Scand. 2011;69:208–214.
- Kvale G, Berg E, Raadal M. The ability of Corah’s Dental Anxiety Scale and Spielberger’s State Anxiety Inventory to distinguish between fearful and regular Norwegian dental patients. Acta Odontol Scand. 1998;56:105–109.
- Amarante E, Raadal M, Espelid I. Impact of diagnostic criteria on the prevalence of dental caries in Norwegian children aged 5, 12 and 18 years. Community Dent Oral Epidemiol. 1998;26:87–94.
- Edman K, Ohrn K, Nordstrom B, et al. Prevalence of dental caries and influencing factors, time trends over a 30-year period in an adult population. Epidemiological studies between 1983 and 2013 in the county of Dalarna, Sweden. Acta Odontol Scand. 2016;74:385–392.
- Bath-Balogh M, Fehrenbach MJ. Illustrated dental embryology, histology, and anatomy. 3rd ed. Dolan J, editor. USA: Elsevier Saunders; 2011.
- Pettersen T, Magritt B. Sámi ethnicity as a variable. Premises and implications for population-based studies on health and living conditions in Norway. UiT The Arctic University of Norway; 2015.
- Senior PA, Bhopal R. Ethnicity as a variable in epidemiological research. BMJ. 1994;309:327–330.
- Vikum E, Krokstad S, Holst D, et al. Socioeconomic inequalities in dental services utilisation in a Norwegian county: the third Nord-Trondelag Health Survey. Scand J Public Health. 2012;40:648–655.
- Holde GE, Oscarson N, Trovik TA, et al. Periodontitis prevalence and severity in adults: a cross-sectional study in Norwegian circumpolar communities. J Periodontol. 2017;88:1012–1022.
- Galea S, Tracy M. Participation rates in epidemiologic studies. Ann Epidemiol. 2007;17:643–653.
- Gulcan F, Ekback G, Ordell S, et al. Exploring the association of dental care utilization with oral impacts on daily performances (OIDP) – a prospective study of ageing people in Norway and Sweden. Acta Odontol Scand. 2018;76:21–29.
- Gulcan F, Ekback G, Ordell S, et al. Inequality in oral health related to early and later life social conditions: a study of elderly in Norway and Sweden. BMC Oral Health. 2015;15:20.
- Holst D, Dahl KE. OHIP-14: Påvirker oral helse livskvaliteten? Den Norske Tannlegeforenings Tidende. 2008;118:212–218.