
Abstract
Objectives
The objectives of the present study were to assess the consumption of acidic beverages, knowledge and concern about preventing dental erosive wear, and to examine potential associations between these variables, in a sample of high school students.
Materials and methods
A survey measuring acidic beverage consumption, knowledge and concern about erosive tooth wear was conducted at 13 high schools in Rogaland county, Norway.
Results
Of the 850 students who completed the questionnaire, 26% reported that they drink acidic beverages every day. There were significant gender differences for the consumption of acidic drinks. The survey also demonstrated that a high proportion of students lacks basic knowledge of what erosive tooth wear is, and that this lack of knowledge is associated with a more frequent intake of acidic beverages. However, students who responded that they are concerned about preventing dental erosive wear reported that they drink soft drinks and energy drinks less frequently than students who are not concerned about this.
Conclusions
Results from this study support assumptions about a lack of knowledge about dental erosive wear in youth, and that this lack of knowledge is associated with a more frequent intake of acidic drinks.
Introduction
Knowledge and prevention of caries have drastically reduced the prevalence of caries in Norwegian youth over the last decades [Citation1]. In comparison, there has been little focus on erosive lesions, even though both research and practice report high prevalence of this kind of dental damage in adolescents. Two recent Norwegian studies reported prevalences of 59% [Citation2] and 38% [Citation3] among 16–18-year-olds (n = 795) and 16-year-olds (n = 392), respectively. In a Swedish survey of prevalence and risk factors among 15- and 17-year-olds (n = 1071), the incidence was somewhat lower, but still sizeable; 28% and 34%, respectively [Citation4]. Moreover, a systematic review from 2015 has estimated the global prevalence of erosive wear in permanent teeth of adolescents to approximately 30% [Citation5]. Several studies also show that boys have a higher incidence than girls [Citation6–9]. The high incidence of dental erosive wear is problematic since the damage is irreversible. The erosive process results in softening of enamel and dentine, and loss of tooth substance, which may give rise to both aesthetic, orthodontic and functional complications and/or endodontic impact including sensitivity to cold and pain [Citation10–12]. Dental erosive wear may be caused by internal or external factors. Internal factors include gastroesophageal reflux and eating disorders with vomiting, while intake of acidic foods and drinks are external factors. A high intake of acidic beverages is considered to be the main external cause of erosive tooth wear among today’s adolescents [Citation4,Citation13–16], and a higher consumption of acidic drinks has been shown in boys compared to girls [Citation17]. In line with this, Skudutyte-Rysstad et al. [Citation18] found associations between erosive wear and daily consumption of acidic beverages and between erosive wear and gender in Norwegian 18-year-olds. In a Swedish study among adolescents aged 13–19 years, Hasselkvist et al. [Citation16] found that a high intake of soft drinks was significantly associated with a generally unhealthy lifestyle and an increased incidence of both erosive lesions and caries (DMTF/DMTS). Other studies have found associations between soft drink consumption and overweight, screen time (TV, PC, etc.), participation in team sports and other physical activities [Citation19–21]. Research also suggests that adolescents have insufficient knowledge about erosive tooth wear [Citation22–24]. In a qualitative study by May and Waterhouse [Citation22], 8–9-year-olds and 13–14-year-olds from two different socio-economic groups were divided into four focus groups (four boys and four girls in each group) and asked what effects they thought different types of beverages could have on their teeth. Results from this study demonstrated that knowledge about the effects of beverages on teeth was confused. The 13–14-year-olds from the high socio-economic status group knew that acidic beverages were harmful to their teeth, but thought that they rotted them. The participants in the other groups believed that sugar in beverages eroded the teeth. A Norwegian survey of 13–20-year-olds (n = 222) reported that 52% of the participants lacked knowledge about the causes of dental erosive wear, 23% had some knowledge, while 25% had good knowledge [Citation24]. In a recent Dutch survey among young adults aged 20–25 years (n = 331), inadequate knowledge of erosive wear was also revealed. While the majority (71%) was aware of the definition of dental erosive wear, only half (52%) of the participants were aware of external causal factors (intake of acidic foods and beverages), and even less (42%) were aware of the consequences of such damage to the teeth [Citation23]. This survey also showed that participants who previously had received or searched for information about dental erosive wear, and who had a higher level of education, had a significantly higher level of knowledge about erosive wear when controlled for factors such as gender, living situation, work situation and frequency of dental visits. A recent review by Gulati and Mittal [Citation13] emphasized that it is a problem that many people are not aware of the damaging effects of acidic beverages.
In the field of consumer psychology, a distinction is often made between subjective and objective knowledge. According to Park and Lessig [Citation25], subjective knowledge constitutes an individual’s perceptions of his/her own knowledge. Objective knowledge, however, is often described as actual, or fact-based, knowledge stored in the individual’s memory [Citation26]. When it comes to subjective knowledge, it is reasonable to assume that people who report high levels of such knowledge about a topic, object/product or behaviour, believe that they have sufficient knowledge, and thus do not have to worry about potential negative consequences of insufficient knowledge. In terms of objective (actual) knowledge, it is important to note that high levels of such knowledge are only advantageous if the person is conscious of his/her own level of knowledge [Citation27]. In the present context, this might suggest that adolescents who are not conscious of, or care about, their own objective knowledge of erosive tooth wear, are less concerned about potentially adverse consequences when consuming acidic beverages. However, it is also reasonable to assume that adolescents who are concerned about preventing dental erosive wear will be conscious of, and try to limit, the intake of acidic beverages. Based on these assumptions, the aims of the present study were to assess the consumption of acidic beverages, subjective- and objective knowledge, and concern about preventing erosive tooth wear in a sample of high school students, and to examine potential associations between these variables.
Materials and methods
Participants and procedures
In October 2018, a survey was conducted in a convenience sample of students attending 13 high schools in Rogaland county, Norway. Students aged 15–20 years attending general or vocational studies were included, while students in adapted educational programmes were not. In total, 889 students completed the questionnaire. After reviewing the raw data, 39 observations were excluded: four as a result of unserious completion, 17 as a result of affiliation to adapted educational programmes, and 18 because of age > 20 years. The final sample consisted of 850 students where 59% were female and 86% were of Norwegian/Nordic ancestry. Sixty-seven percent attended general studies, while 33% attended vocational study programmes. The average age was 17 years (standard deviation: 1.10). Dental hygienists, dentists and community nurses recruited participants for the survey by standing at booths located in the high school entries or cantinas. The students were verbally informed about the survey and invited to fill out a two-page questionnaire with questions about consumption of various types of beverages (both acidic and ‘neutral’), knowledge and concern about dental erosive wear. Students who wished to participate gave their consent by completing the questionnaire. The participants received a toothbrush and toothpaste after filling out the questionnaire, and were offered the opportunity to participate in a raffle with the chance to win a small prize (bluetooth loudspeaker or movie tickets). Participation in the raffle could not be linked to the questionnaire, which was totally anonymous. There was no need for the survey to be approved by the Regional Ethics Committee (REC) or the Norwegian Centre for Research Data (NSD), since the participants were fully competent to give their consent and since the information that was collected was neither of a sensitive nature, nor could it be traced back to individuals.
Questionnaire
The questions were developed based on previous investigations and in cooperation with researchers and dental staff at the Oral Health Centre of Expertise in Rogaland, Norway. The questionnaire was pre-tested on representatives from the target group (one boy aged 15, three girls aged 19), and revisions were made based on their feedback. The consumption of 12 different types of beverage (seven acidic and five ‘neutral’ ones) was measured with the question ‘How often do you drink the following types of beverage during the course of a week?’. Nine response options were given: never/rarely (1), one day/week (2), two days/week (3), three days/week (4), four days/week (5), five days/week (6), six days/week (7), every day (8) and several times every day (9). The responses were recoded to create a common denominator reflecting consumption in days/week (0–7) before further analyses were undertaken (i.e. 1 = 0 days/week, 2 = 1 day/week… 8 = 7 days/week, 9 = 7 days/week). Since the present study focussed on acidic beverage consumption, data on the five ‘neutral’ types of drinks (i.e. milk, coffee, iced coffee, tea, tap water) were excluded from the analyses. Knowledge about dental erosive wear was measured using eight statements. Two statements were designed to measure subjective knowledge: ‘I know what erosive tooth wear is’ and ‘I know how erosive tooth wear occurs’. Six statements were designed to measure objective knowledge: ‘Erosive tooth wear can be prevented (avoided) by brushing your teeth after consumption of acidic beverages’, ‘Erosive tooth wear can be prevented (avoided) by spreading out the consumption of acidic beverages throughout the day’, ‘Erosive tooth wear can be prevented (avoided) by concentrating the consumption of acidic beverages to short periods of time during the day’ (reversed), ‘Erosive tooth wear is reversible (can be repaired/disappear)’, ‘Erosive tooth wear can be reversed by good dental hygiene (e.g. regular brushing of teeth)’ and ‘Erosive tooth wear can be reversed through dental treatment’. The knowledge statements were designed so that high scores for subjective knowledge indicated strong beliefs in one’s own knowledge about dental erosive wear, whereas high scores for objective knowledge indicated deficient factual knowledge about dental erosive wear. Thus, the term ‘deficient objective knowledge’ will be used throughout the subsequent parts of this paper. Concern about preventing dental erosive wear was measured using one statement: ‘I am concerned about preventing erosive tooth wear’. Response options for the knowledge and concern measures were provided on a five-point Likert scale: totally disagree (1), somewhat disagree (2), neutral/neither agree nor disagree (3), somewhat agree (4) and totally agree (5). The questionnaire also included questions about sociodemographic variables (gender, age, ethnicity, and field of study). These variables were used to describe the sample, to investigate gender differences and as control variables in model analyses.
Statistical analyses
All analyses were conducted using IBM SPSS Statistics for Windows, Version 24.0 (IBM SPSS Statistics, Armonk, NY). Initially, a psychometric evaluation of the knowledge measures was carried out to investigate the factor structure and reliability of this battery of questions, and to condense the knowledge data for subsequent testing of associations between knowledge about dental erosive wear and consumption of acidic beverages. The psychometric evaluation included factor analysis and computation of internal consistency reliability (Cronbach’s alpha). We used Hair et al.’s [Citation28] recommendations for assessment of the appropriateness of our data for factor analysis: a correlation matrix with coefficients >0.30, a KMO value ≥0.60 and a significant Bartlett’s test (p < .05). The Kaiser criterion (Eigen value > 1) and Oblique rotation (based on assumptions about inter-correlations between items belonging to different factors) were used to determine the factor structure of the data. Factor loadings ≥0.40 were used as criteria for convergent validity, whereas cross-loadings of < 0.40 were used as criteria for discriminant validity [Citation28]. The evaluation also included omission of overlapping/redundant statements from further analyses. Internal consistency reliability (Cronbach’s alpha) was classified as alpha ≥ 0.60 = acceptable and alpha ≥ 0.70 = good [Citation29]. Descriptive analyses included relative frequencies of agreement (i.e. the combined scores for somewhat agree and totally agree) for each of the knowledge statements, in addition to the calculation of means, standard deviations, skewness and kurtosis for all study variables. In line with Kline [Citation30], we used cut-off values of ±3 and ±8 for skewness and kurtosis, respectively. Independent samples t-tests were used to reveal potential differences between genders regarding the consumption of acidic beverages. Prior to model analyses, bivariate correlation analyses were performed to test for multicollinearity between independent variables. We used a cut-off value of ≥0.80 for multicollinearity as proposed by Haerens et al. [Citation31]. Multiple linear regressions were run to explore potential associations between consumption of acidic beverages, subjective knowledge, deficient objective knowledge and concern about preventing dental erosive wear. More specifically, three models were tested: one model with ‘all acidic beverages’ (i.e. the total consumption of all types of acidic beverages) as the dependent variable (model 1); one model with the consumption of ‘healthy acidic beverages’ (i.e. beverages with a ‘healthy profile’ such as juice/nectar,Footnote1 smoothie, sports drinksFootnote2 and flavoured water) as the dependent variable (model 2); and one model with the consumption of ‘unhealthy acidic beverages’ (i.e. beverages with an ‘unhealthy profile’ such as soft drinks with sugar,Footnote3 soft drinks without sugarFootnote4 and energy drinksFootnote5) as the dependent variable (model 3). All models were adjusted for sociodemographic variables (gender, age, ethnicity and field of study).
Results
Psychometric evaluation of the knowledge measures
The aforementioned prerequisites for factor analysis were fulfilled in our data (several correlation coefficients over 0.30, a significant Bartlett’s test and a KMO > 0.60). Since the two statements ‘Erosive tooth wear can be prevented (avoided) by spreading out the consumption of acidic beverages throughout the day’ and ‘Erosive tooth wear can be prevented (avoided) by concentrating the consumption of acidic beverages to shorter periods during the day’, were partially overlapping and with reversed wordings, only the first statement was included in further analyses. The factor analysis resulted in a two-factor solution that explained 61% of the variance in our data. Five statements that reflected deficient fact-based knowledge loaded on the first factor, while two statements that reflected perceptions of one’s own knowledge loaded on the second. The factor loadings ranged from 0.51 to 0.86, and no cross-loadings were revealed. The criteria for convergent and discriminant validity were thus fulfilled. Based on the theoretical division of knowledge into objective and subjective knowledge as described in the introduction, the factors were named ‘deficient objective knowledge’ (factor 1) and ‘subjective knowledge’ (factor 2). Cronbach’s alpha for the two knowledge factors were 0.75 and 0.79, respectively. Results from psychometric evaluation of the knowledge measures are presented in . As our analyses provided support for a presumptive factor structure, and good internal consistency reliability was shown for each of the factors, they were considered to be valid and suitable for measuring subjective knowledge and deficient objective knowledge about dental erosive wear among adolescents attending high school. The overall score for the statements in each of the two factors was calculated and the condensed knowledge measures were used as independent variables in subsequent regression analyses.
Table 1. Factor loadings, Cronbach's alpha (α) and variance explained (R2) for the knowledge measures.
Descriptive analyses and independent sample t-tests
Means, standard deviations, skewness and kurtosis for the study variables (i.e. condensed measures for subjective knowledge and deficient objective knowledge, concern about preventing dental erosive wear and the consumption frequencies for acidic beverages) are presented in . All study variables (with one exception; the consumption frequency of sports drinks) had values within the range of chosen cut-offs for skewness and kurtosis, and no multicollinearities were revealed among the independent variables included in regression analyses. Thus, the choice of parametric statistical techniques for further analyses was considered unproblematic.
Table 2. Means, standard deviations (SD), skewness and kurtosis for the condensed knowledge measures (subjective knowledge and deficient objective knowledge), concern about preventing erosive tooth wear and the consumption frequency (days per week) for acidic beverages.
Consumption of acidic beverages
Mean consumption frequencies for each of the seven types of acidic beverages and the collapsed variables named ‘all acidic beverages’ (including all seven types), ‘unhealthy acidic beverages’ (including energy drinks and soft drinks with/without sugar) and ‘healthy acidic beverages’ (including fruit juice/nectar, smoothie, sports drinks and flavoured water) are displayed in . Twenty-six percent (n = 221) of the students in our sample (n = 850) stated that they drink at least one acidic beverage on a daily basis. Furthermore, 20% (n = 170) reported that they consume ‘unhealthy acidic beverages’ every day, while 12% (n = 102) stated that they drink ‘healthy acidic beverages’ every day (). Independent samples t-tests revealed statistically significant differences between male and female students. Males had a significantly higher frequency of consumption for ‘all acidic beverages’ (t (843) = 2.99, p = .003), for ‘unhealthy acidic beverages’ (t (843) = 3.93, p < .001) and for ‘healthy acidic beverages’ (t (843) = 2.51, p = .014) (). The biggest difference was found for consumption of ‘unhealthy acidic beverages’; 24% (n = 84) of the male students (n = 348) stated that they drink an ‘unhealthy acidic beverage’ every day as opposed to 17% (n = 85) of the female students (n = 502) ().
Figure 1. Consumption of at least one type of acidic beverage (days per week) in the total sample (n = 850). Both ‘healthy’ and ‘unhealthy acidic beverages’ are included.
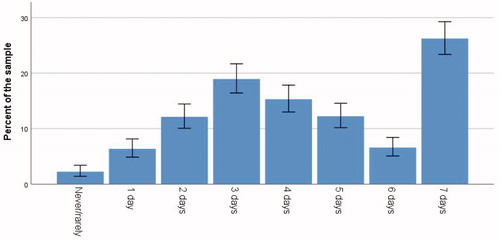
Figure 2. Differences between male (n = 348) and female (n = 502) students regarding the consumption of 'unhealthy acidic beverages' (days per week).
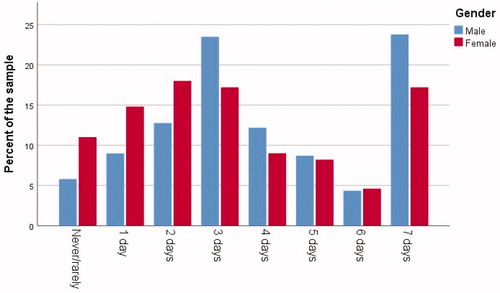
Table 3. Differences in consumption frequency between genders.
Knowledge and concern about dental erosive wear
Mean scores for subjective knowledge and concern about preventing dental erosive wear were above the neutral point (i.e. somewhat agree), while the mean score for deficient objective knowledge was lower (around the neutral point, i.e. neither agree nor disagree) (). Relative frequencies of agreement (based on the sum of scores for the response alternatives somewhat agree (4) and totally agree (5)) for each of the knowledge statements (i.e. before collapsing them into condensed knowledge measures), and for concern about preventing dental erosive wear, are presented in . As can be seen from this table, the proportion of students with high scores for subjective knowledge was larger than the proportion of students with high scores for deficient objective knowledge and concern about preventing dental erosive wear.
Table 4. Relative frequencies of agreement for items measuring knowledge and concern about preventing erosive tooth wear.
Regression analyses
Three multiple linear regression models were tested. All models included the independent variables subjective knowledge, deficient objective knowledge and concern about preventing dental erosive wear, as well as the control variables age, gender, field of study and ethnicity. Results from multiple linear regression analyses are presented in . Statistically significant associations were found in all models. In model 1, a positive association was found between deficient objective knowledge and total consumption of ‘all acidic beverages’ (β = 0.15, p < .001). In model 2, a positive association was found between deficient objective knowledge and consumption of ‘healthy acidic beverages’ (β = 0.14, p < .001). In model 3, a positive association between deficient objective knowledge and consumption of ‘unhealthy acidic beverages’ (β = 0.11, p < .01), and a negative association between concern about preventing dental erosive wear and consumption of ‘unhealthy acidic beverages’ (β = −0.12, p < .01), was revealed.
Table 5. Regression coefficients (β) and variance explained (R2) for associations between subjective knowledge, deficient objective knowledge, concern about preventing erosive tooth wear and the consumption of acidic beverages.
Discussion
The objectives of this study were to assess high school students’ consumption of acidic beverages, knowledge and concern about preventing dental erosive wear, and to explore potential associations between these variables.
Consumption of acidic beverages
We identified a large risk group for developing erosive tooth wear as 26% of the students reported that they drink some sort of acidic beverage every day. Furthermore, boys reported significantly higher consumption frequencies than girls, especially when it comes to ‘unhealthy acidic beverages’. A frequent consumption of ‘unhealthy acidic beverages’ such as soft drinks is considered particularly risky regarding the development of erosive wear because these products are often consumed over a prolonged period of time and in greater volumes than ‘healthy acidic beverages’ like fruit juices. Additionally, soft drinks are often consumed in the absence of food, while fruit juices are typically consumed as part of a meal. Research has shown that boys have a higher prevalence of erosive tooth wear than girls, and that this can be related to more frequent consumption of acidic beverages [Citation6–8]. Furthermore, numerous studies have shown that boys generally consume more soft drinks than girls, thereby supporting our findings on gender differences [Citation16,Citation32–35]. However, figures from the report ‘Developments in the Norwegian Diet 2018’ [Citation36] show that the consumption of sugar-sweetened soda (carbonated soft drinks) has decreased by almost 30% since 2000, while the consumption of artificially sweetened soda and mineral water increased significantly during this period. This is in line with international research that reports an increased consumption of artificially sweetened soft drinks [Citation37]. In recent years, Norwegian authorities have focussed on reducing the consumption of sugary drinks. For example, during the period 2007–2011, the goal was to reduce the proportion of people consuming sugary drinks on a daily basis by 20% [Citation38], and in the period from 2017 to 2021 the goal is to reduce the proportion of adolescents drinking sugary drinks five times per week or more by 50% [Citation39]. Furthermore, one of the 12 official Norwegian dietary advices has an explicit focus on the consumption of sugary foods and beverages: ‘Avoid foods and beverages with lots of sugar on an everyday basis’ [Citation40]. These goals and dietary advices are important in terms of preventing excess weight, obesity and other lifestyle diseases associated with the consumption of sugary drinks [Citation41,Citation42]. However, with the increasing prevalence of dental erosive wear observed among adolescents, there may also be a need for health policy objectives and official dietary advices related to matters of significance for dental health. For example, it seems relevant to include information about the potential detrimental effects that both sugar-sweetened and artificially sweetened beverages can have on dental health in official dietary guidelines.
Knowledge and concern about dental erosion
The high proportion of participants scoring above the neutral point (i.e. somewhat/totally agree) for items measuring subjective knowledge suggests that the adolescents in our sample had relatively strong beliefs about their own knowledge about dental erosive wear. The proportion with high scores for items measuring deficient objective knowledge about erosive wear was lower, but still disturbingly high for some of the statements. For example, almost 60% of the students somewhat or totally agreed that erosive tooth wear can be prevented by brushing the teeth after consuming acidic beverages. However, an equally large proportion (close to 60% of the students in the sample) somewhat or totally agreed that they are concerned about preventing erosive tooth wear. Thus, there seem to be a discrepancy between wanting to prevent dental erosion and the knowledge about how to do it. These findings support previous reports of insufficient knowledge about dental erosive wear among adolescents [Citation23,Citation24].
Associations between acidic beverage consumption, knowledge and concern about dental erosive wear
Significant positive associations were found between deficient objective knowledge and acidic beverage consumption frequency in the three multiple linear regression models tested. Additionally, in model 3, a significant negative association was found between concern about preventing dental erosive wear and the consumption frequency of ‘unhealthy acidic beverages’. This finding supports our initial assumption that people who are concerned about preventing erosive wear will tend to have a lower consumption of acidic beverages. Interestingly, similar associations were not found when we looked at the consumption of ‘all acidic beverages’ (model 1) and the consumption of ‘healthy acidic beverages’ (model 2). One possible explanation may be that ‘unhealthy acidic beverages’ are perceived as more damaging to the teeth than ‘healthy acidic beverages’. It may also be that the positive attributes of ‘healthy acidic beverages’ (vitamins in juices and smoothies, lower sugar content in flavoured water) to some extent outweigh the negative attributes (that they are acidic) of these products. Hence, ‘healthy acidic beverages’ may be considered better alternatives among the students in our sample. However, all the models had low explanatory power, implying that there are other factors than knowledge and concern about preventing dental erosive wear offering a better explanation for the consumption of different types of acidic beverages among adolescents. For example, in a recent Norwegian study by Gebremariam et al. [Citation43], a positive association was found between availability and consumption of sugary beverages, while a negative association was found between parental rules (i.e. parents setting limitations on consumption) and consumption of sugary beverages among 13–15-year-olds. In two other Norwegian studies focussing on adolescent consumption of sugary soft drinks, associations were found between high consumption and factors such as impulsiveness [Citation44], self-control, social pressure and intentions [Citation45]. Moreover, in a study focussing on the consumption of various types of beverages such as fruit juice, nectar, smoothies, iced tea, energy drinks and chocolate milk, associations were found between dietary advice from parents and adolescent consumption of some of these beverages [Citation33]. The latter study also confirms well-known relationships between the consumption of ‘healthy’ and ‘unhealthy’ products and sociodemographic variables such as gender and parental educational level. For example, girls had a higher consumption of smoothies, while boys drank more iced tea, energy drinks and chocolate milk. Moreover, adolescents with highly educated parents drank more juice, while adolescents having parents with a lower level of education drank more energy drinks and chocolate milk [Citation33]. The objective of our study, however, was not to adapt models with the largest possible explanatory power, but to explore potential associations between the consumption of various types of acidic beverages, knowledge and concern about preventing dental erosive wear among high school students. Our results support the assumption that young people have insufficient objective knowledge about erosive tooth wear and that this lack of knowledge is associated with increased consumption of acidic beverages.
Strengths, limitations and conclusive remarks
One strength of the present study is its large sample size, which allows the application of parametric techniques, thereby increasing the statistical power of the results. An obvious limitation is that all data are based on self-reports. It is widely recognized that self-reports are often more optimistic than objective measurements (i.e. participants respond in line with what is considered desirable behaviour in a specific context). Another limitation is the cross-sectional design of the study, which does not allow for causal inferences. Nevertheless, the results of the present study suggest that, despite of an increased focus on erosive tooth wear in dental research and practice, there seems to be a need for raising the awareness and factual knowledge about dental erosive wear in youth – not only about the consequences of such damage, but also about how to prevent it. Being aware that knowledge is a prerequisite, but by itself not sufficient to induce behaviour change, the authors of this paper hope that results from the present study may be of use as a starting point for future research on factors and mechanisms that may help explain dental health-related behaviours among adolescents. Understanding the factors and mechanisms at play is essential for the development and implementation of effective preventive programmes in this particular group of the population.
Correction Statement
This article has been republished with minor changes. These changes do not impact the academic content of the article.
Acknowledgements
The authors thank dental hygienists, dentists and community nurses who contributed to data collection, and students who answered the questionnaire.
Disclosure statement
The authors report no conflict of interest.
Additional information
Funding
Notes
1 Orange juice, apple nectar, etc.
2 YT, Powerade, Maxim, etc.
3 Soda, cordials, iced tea, etc. with sugar.
4 Soda, cordials, iced tea, etc. without sugar.
5 Red Bull, Battery, etc.
References
- Haugejorden O, Birkeland JM. Karies i Norge i fortid og fremtid: analyse av endringer og årsaker. Den Norske Tannlegeforenings Tidende. 2008;2(118):84–90.
- Søvik JB, Tveit AB, Storesund T, et al. Dental erosion: a widespread condition nowadays? A cross-sectional study among a group of adolescents in Norway. Acta Odontol Scand. 2014;72(7):523–529.
- Mulic A, Fredriksen O, Jacobsen ID, et al. Dental erosion: prevalence and severity among 16-year-old adolescents in Troms, Norway. Eur Arch Paediatr Dent. 2016;17(3):197–201.
- Jarkander MS, Grindefjord M, Carlstedt K. Dental erosion, prevalence and risk factors among a group of adolescents in Stockholm County. Eur Arch Paediatr Dent. 2018;19(1):23–31.
- Salas MMS, Nascimento GG, Huysmans MC, et al. Estimated prevalence of erosive tooth wear in permanent teeth of children and adolescents: an epidemiological systematic review and meta-regression analysis. J Dent. 2015;43(1):42–50.
- Alaraudanjoki V, Laitala ML, Tjaderhane L, et al. Association of erosive tooth wear and dental caries in Northern Finland Birth Cohort 1966 – an epidemiological cross-sectional study. BMC Oral Health. 2017;17(1):6.
- Arnadottir IB, Holbrook WP, Eggertsson H, et al. Prevalence of dental erosion in children: a national survey. Community Dent Oral Epidemiol. 2010;38(6):521–526.
- Jaeggi T, Lussi A. Prevalence, incidence and distribution of erosion. Monogr Oral Sci. 2014;25:55–73.
- Mulic A, Tveit AB, Skaare AB. Prevalence and severity of dental erosive wear among a group of Norwegian 18-year-olds. Acta Odontol Scand. 2013;71(3–4):475–481.
- Bardsley PF. The evolution of tooth wear indices. Clin Oral Invest. 2008;12(S1):15–19.
- Johansson AK, Lingstrom P, Birkhed D. Comparison of factors potentially related to the occurrence of dental erosion in high- and low-erosion groups. Eur J Oral Sci. 2002;110(3):204–211.
- Huysmans MC, Chew HP, Ellwood RP. Clinical studies of dental erosion and erosive wear. Caries Res. 2011;45(s1):60–68.
- Gulati P, Mittal MA. Frequent consumption of soft drinks and dental erosion: a literature review. BAOJ Dentistry. 2016;2(3):1–5
- Søvik JB, Skudutyte-Rysstad R, Tveit AB, et al. Sour sweets and acidic beverage consumption are risk indicators for dental erosion. Caries Res. 2015;49(3):243–250.
- Isaksson H, Birkhed D, Wendt L-K, et al. Prevalence of dental erosion and association with lifestyle factors in Swedish 20-year olds. Acta Odontol Scand. 2014;72(6):448–457.
- Hasselkvist A, Johansson A, Johansson AK. Association between soft drink consumption, oral health and some lifestyle factors in Swedish adolescents. Acta Odontol Scand. 2014;72(8):1039–1046.
- Milosevic A, Bardsley PF, Taylor S. Epidemiological studies of tooth wear and dental erosion in 14-year old children in North West England. Part 2: the association of diet and habits. Br Dent J. 2004;197(8):479–483.
- Skudutyte-Rysstad R, Mulic A, Skeie MS, et al. Awareness and attitudes related to dental erosive wear among 18-yr-old adolescents in Oslo, Norway. Eur J Oral Sci. 2013;121(5):471–476.
- Singh AS, Chinapaw MJ, Brug J, et al. Ethnic differences in BMI among Dutch adolescents: what is the role of screen-viewing, active commuting to school, and consumption of soft drinks and high-caloric snacks? Int J Behav Nutr Phys Act. 2009;6(1):23.
- Liang T, Kuhle S, Veugelers PJ. Nutrition and body weights of Canadian children watching television and eating while watching television. Public Health Nutr. 2009;12(12):2457–2463.
- Giammattei J, Blix G, Marshak HH, et al. Television watching and soft drink consumption: associations with obesity in 11- to 13-year-old schoolchildren. Arch Pediatr Adolesc Med. 2003;157(9):882–886.
- May J, Waterhouse PJ. Dental erosion and soft drinks: a qualitative assessment of knowledge, attitude and behaviour using focus groups of schoolchildren. A preliminary study. Int J Paediatr Dent. 2003;13(6):425–433.
- Verploegen VJN, Schuller AA. Erosive tooth wear: knowledge among young adults and their preferred information sources. Int J Dent Hyg. 2019;17(1):85–92.
- Andersen EH, Isaksen MB. Dentale erosjoner [Master's thesis]. Tromsø: UiT Norges Arktiske Universitet; 2017.
- Park CW, Lessig VP. Familiarity and its impact on consumer decision biases and heuristics. J Consum Res. 1981;8(2):223–230.
- Bettman JR, Park CW. Effects of prior knowledge and experience and phase of the choice process on consumer decision processes: a protocol analysis. J Consum Res. 1980;7(3):234–248.
- Hansen H, Mehmetoglu M. Optimum stimulation level and consumer attitudes toward time share second homes. J Vacat Market. 2009;15(4):335–347.
- Hair JF, Black WC, Babin BJ, et al. Multivariate data analysis. A global perspective. 7th ed. Upper Saddle River (NJ): Pearson Education, Inc.; 2010.
- Field A. Discovering statistics using IBM SPSS statistics. 4th ed. London: SAGE Publications Ltd.; 2013.
- Kline RB. Methodology in the social sciences. Principles and practice of structural equation modeling. 2nd ed. New York (US): Guilford Press; 2005.
- Haerens L, Craeynest M, Deforche B, et al. The contribution of psychosocial and home environmental factors in explaining eating behaviours in adolescents. Eur J Clin Nutr. 2008;62(1):51–59.
- Bjelland M, Lien N, Grydeland M, et al. Intakes and perceived home availability of sugar-sweetened beverages, fruit and vegetables as reported by mothers, fathers and adolescents in the HEIA (HEalth In Adolescents) study. Public Health Nutr. 2011;14(12):2156–2165.
- Nordnes ET, Melbye EL, Pedersen I, et al. Hva betyr kjønn, foreldres utdanningsnivå og foreldrepraksis for ungdommers inntak av ulike typer drikke? Norsk Tidsskrift Ernaering. 2016;4:6–12.
- Nowak D, Jasionowski A. Analysis of the consumption of caffeinated energy drinks among Polish adolescents. Int J Environ Res Public Health. 2015;12(7):7910–7921.
- West DS, Bursac Z, Quimby D, et al. Self-reported sugar sweetened beverage intake among college students. Obesity. 2006;14(10):1825–1831.
- Helsedirektoratet. Utviklingen i norsk kosthold 2018. Matforsyningsstatistikk og forbruksundersøkelser. Oslo: Helsedirektoratet; 2019.
- Sylvetsky AC, Rother KI. Trends in the consumption of low-calorie sweeteners. Physiol Behav. 2016;164:446–450.
- Departementene. Handlingsplan for bedre kosthold i befolkningen (2007–2011). Oppskrift for et sunnere kosthold. Oslo: Helse- og omsorgsdepartementet; 2007.
- Departementene. Nasjonal handlingsplan for bedre kosthold (2017–2021). Sunt kosthold, måltidsglede og god helse for alle! Oslo: Helse- og omsorgsdepartementet; 2017.
- Helsedirektoratet. Kostrådene; 2016. Available from: https://www.helsedirektoratet.no/faglige-rad/kostradene-og-naeringsstoffer
- Basu S, McKee M, Galea G, et al. Relationship of soft drink consumption to global overweight, obesity, and diabetes: a cross-national analysis of 75 countries. Am J Public Health. 2013;103(11):2071–2077.
- Grimes CA, Riddell LJ, Campbell KJ, et al. Dietary salt intake, sugar-sweetened beverage consumption, and obesity risk. Pediatrics. 2013;131(1):14–21.
- Gebremariam MK, Lien N, Torheim LE, et al. Perceived rules and accessibility: measurement and mediating role in the association between parental education and vegetable and soft drink intake. Nutr J. 2015;15(1):76.
- Melbye EL, Bergh IH, Hausken SES, et al. Adolescent impulsivity and soft drink consumption: the role of parental regulation. Appetite. 2016;96:432–442.
- Melbye EL, Helland MH. Soft drinks for lunch? Self-control, intentions and social influences. Br Food J. 2018;120(8):1735–1748.