
Abstract
Objective
The aim of this study was to evaluate if delayed dental development is a cause of postponed care for patients with impacted maxillary canine (IMC).
Materials and methods
This case-control study was based on 403,355 children and adolescents in Region Västra Götaland, Sweden. The subjects, who were in the age range of 9–16 years during the period of 2011–2013, underwent surgical exposure or removal of a maxillary canine. Demirjian’s dental age assessment was carried out on panoramic radiographs.
Results
In total, 1028 patients, 514 with IMC and 514 age- and gender-matched controls, were enrolled. The patients with IMC exhibited a dental development delay of 0.2 years compared to the control group. In the impaction sub-groups, the female patients, patients in the chronological age group of 12–13 years, and patients with palatally positioned IMC had a significantly lower dental age than their paired-control subjects.
Conclusions
Overall, the difference in dental age between patients with or without IMC is significant but small, and as such is likely of minor clinical relevance. Therefore, the timing of preventive care and treatment for patients with IMC should be the same as that for patients with normally erupting canines.
Introduction
Monitoring of dental development in growing individuals is important for the early diagnosis of malocclusions and for improving the prognosis of an effective intervention. This applies in particular to the permanent maxillary canine, which with a prevalence of 1–2% is the second-most-prone tooth to become impacted [Citation1–5]. Dental impaction is a condition when a tooth remains embedded in the alveolar bone and fails to erupt into the oral cavity at the expected time [Citation6]. An impacted tooth may be located in a correct or displaced position, whereas an ectopic tooth is always displaced. Severely ectopic teeth can be predicted to become impacted, even though the expected developmental window has not yet passed. [Citation5] With correctly performed interceptive treatment in a timely manner, permanent maxillary canines that exhibit an ectopic position are able to spontaneously erupt [Citation7]. If preventive care is insufficient, surgical exposure or surgical removal of the impacted maxillary canine (IMC) is necessary.
On occasion, the age of the patient may be considered high at the time of surgical exposure or surgical removal. The question then is if the interceptive care has been neglected or if the postponed treatment is due to late dental development. The consequences of postponed diagnosis and preventive care involve costly and time-consuming treatments and also potential severe root resorptions with loss of the front teeth as a result [Citation8]. Analyses of possible causes of postponed care are therefore crucial.
Delayed dental development has been suggested to be associated with impacted maxillary canines [Citation9]. Evaluation if delayed dental development is a cause of postponed treatment, is possible by comparing dental age (DA) in patients with IMC and DA in patients with normally erupting canines. Previous studies, based on relatively small sample sizes and different populations, have analyzed the relationship between DA and patients with IMC, and have reported discrepant outcomes [Citation10–13] (). Only one previous study has considered gender as an influencing factor to the difference in DA between patients with or without IMC, whereas no study to date has considered chronological age groups. While the aetiology of IMC is still unknown, previous studies have investigated whether buccally or palatally positioned IMC to have different aetiologies, with no clear consensus being reached [Citation10–13]. Therefore, the aim of this study was to evaluate if delayed dental development is a cause of postponed care for patients with IMC by determining whether DA differs between patients with IMC and patients with normally erupting maxillary canines. The factors gender, chronological age group and position of the IMC were also considered. Our hypothesis is that there are no differences in DA between the impaction group (IG) and the control group (CG).
Table 1. Previous studies analysing the relationship between DA and patients with IMC.
Materials and methods
Study design
This case control study was approved by the Regional Ethics Board at the University of Gothenburg, Sweden (Dnr. 898-13).
Data collection
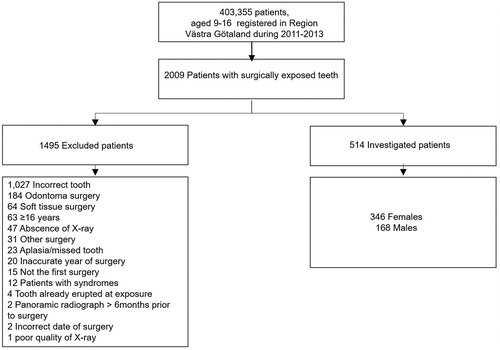
The study is based on 403,355 children and adolescents in Region Västra Götaland who during the period 2011–2013 were in the age range of 9–16 years. Patients that had undergone surgical exposure or removal of an impacted maxillary canine were included. The maxillary canines were either diagnosed as impacted (for older age groups) or as having a severely ectopic position, which strongly suggested that they would become impacted (for younger age groups). The dental records of the identified patients in the IG were screened for gender, chronological age (CA) at the time of panoramic radiography, and position of the IMC. The position was determined based on the recorded notes of the surgeon or the radiographical examinations performed prior to the surgery. Excluded from the study were those patients who had panoramic images of unsatisfactory quality, chronological age >16.0 years, and craniofacial syndromes, as well as those who had previously undergone surgical exposure of an IMC ().
Figure 1. Patient distribution.
Control group
The CG consisted of patients with normally erupting maxillary canines who were age-matched (±0.1 year) and gender-matched with the patients in the IG. Patients in the CG were consecutively selected from the same orthodontic clinics as the patients in the IG. Only patients with existing panoramic radiographs were included in the CG. For control patients who had un-erupted maxillary canines, their clinical records were checked to assure that the permanent canines subsequently erupted without surgical intervention.
Dental age assessment
DA was estimated using the method described in 1973 by Demirjian et al. [Citation14]. The system is based on analysis using panoramic radiographs of root development in the seven lower-left teeth [Citation14]. In brief, a development stage is determined for each tooth, generating a score. The scores are then summed to give the final value, which is translated into a DA estimate. The lower age limit of the system is 3 years, and the upper age limit is 16 years. In the present study, if a tooth was missing or the apex was unclear on the left-hand side, the contralateral tooth was used. The examiner was blinded to the patients’ age and gender until the developmental stages were determined and the DAs of all the patients were finalized.
Intra-examiner reliability
The intra-class correlation coefficient (ICC) was applied to assess the intra-examiner reliability. The ICC estimates and their 95% confidence intervals were calculated using the SPSS statistical package ver. 24 (SPSS Inc., Chicago, IL) based on a single measurement/rater, absolute-agreement, 2-way mixed-effects model. The initial measurements were performed on 30 patients (MLL), who were re-measured one month later.
Statistical analysis
All the data were analyzed using the Excel MS ver. 2018 software (Microsoft Corp., Redmond, WA). A QQ-plot was constructed and demonstrated that the residuals were not normally distributed, so a non-parametric test was chosen. Since DA has a maximum possible value of 16.0, the sign test, rather than the signed-rank test, was utilized for comparing DA with CA within the IG and CG, and also for comparisons of the DA values between the two groups. All tests were two-sided and p-values <0.05 were considered statistically significant.
Results
In total, 514 patients with IMC, 346 (67%) females and 168 (33% males), were enrolled and examined for DA, as were 514 age- and gender-matched controls. The median chronological age of the IG was 13.7 [95% CI 12.8–15.0], with a range of 9.1–16.0 years. The intra-examiner reliability ICC for the examiners was 0.92.
The overall IG had a significantly (p < 0.001) lower DA (median of differences of 0.2 years) than the CG (). Of the gender subgroups, the difference in DA between the IG and CG was only significant for females (p < 0.001) ( and ).
Table 2. DA and CA for all patients with respect to chronological age groups.
Table 3. DA and CA for male patients with respect to chronological age groups.
Table 4. DA and CA for female patients with respect to chronological age groups.
Of the seven chronological age sub-groups, DA was significantly higher in the CG than in the IG for age groups 12 and 13 in the total group (). A separate analysis of the chronological age groups for females and males, respectively, showed no significant differences in DA for the males and a significant difference only in the chronological age group of 12 years (median of differences, 0.5 years) for the females ( and ).
Regarding the position of the IMC, only those patients who had a palatal position of the IMC had a significantly lower DA than their paired controls. The median differences was 0.0 years, whereas the mean difference was 0.3 years ().
Table 5. DA and CA for all patients with respect to the position of the IMC.
Discussion
In this study, the overall impaction group had a significantly lower DA than the control group. This indicates that patients with IMC have delayed dental development compared to patients who have normally erupting canines. However, the difference in DA between the groups was only 2.4 months, which is of minor clinical relevance.
A comparison of DA in patients with IMC and patients with normally erupting canines has been performed in only one previous study [Citation11]. Rozylo-Kalinowska et al. included fewer patients than in the present study, and the patients with IMC showed delayed dental development compared with those with normally erupting canines, which is in accordance with the results of the present study. However, in the previous study, the absolute age difference was slightly larger than in the present study, which might be explained by the different sizes and geographical origins of the patient groups studied.
When analyzing dental development in patients with IMC, it is important to consider not only the patients at a group level but also other factors that may be important in identifying any other aberrant dental development in individuals within the group. Examples of these factors are gender, chronological age groups, and the position of the IMC. All these factors may require special attention when supervising dental development, especially the eruption timing of the permanent canines. In the present study, the differences in DA between the IG and CG were systematically investigated in terms of gender, chronological age group, and position of the IMC, which have not been studied previously in this context. In the present study, only females and patients in the chronological age groups of 12 and 13 years in the IG exhibit significantly delayed dental development compared with the patients in the CG. In general, only those groups with the most patients show significant age differences in the present study, however, the small differences in DA observed in this study lack clinical relevance.
In the present study, the relationship between DA in the IG and the CG was studied in terms of several factors. The comparison of DA is possible due to the large cohort surveyed, and because the CG was matched with respect to gender and CA (with a precision of 1.2 months) against the experimental group. The results of the present study are, therefore, independent of any methodological error, that is, the absolute value of the age difference between the groups is valid.
Previous studies have instead of presenting results for the differences in DA between patients with IMC and patients without IMC, presented results for DA in relation to CA. Methods for DA assessment correlate with CA to a varying degree, and if DA is compared to CA the absolute age difference will be biased due to errors of the method [Citation15]. For example, Demirjian’s DA assessment, which is based on a French-Canadian population, resulted in a higher DA than CA of a different magnitude not only in the present study but also in other studied populations and the difference between DA and CA varied between the populations [Citation15–19]. In a Swedish population, a higher DA than CA with about one year has earlier been reported [Citation17]. A higher DA than CA using Demirjian’s index might also be explained by the fact that the index was elaborated in 1973, and more precocious maturation of children has been reported in subsequent generations [Citation20,Citation21]. Age estimation based on Demirjian’s index is, therefore, not an accurate method to evaluate DA, since a higher DA than CA has been demonstrated in most populations. Thus, the index needs to be updated in line with the characteristics of present-day children and adolescents.
Other limitations associated with Demirjian’s DA method are the upper age limit of 16 years and the large age difference between some of the tooth stages, which may result in a difference of 1.4 years at most. An alternative method for DA estimation is the Haavikko’s index, which is based on a study sample similar to the one considered in the current study [Citation22]. However, the Haavikko system has an upper age limit of 13 years and includes in the age assessment the root development of the maxillary right canine, which is difficult to evaluate in the panoramic radiographs taken for patients with IMC. Despite the limitations of Demirjian’s assessment, it is the most widely used method for DA estimation in children. Also, a comparison of different methods has concluded that Demirjian’s assessment is the most straight-forward and most-detailed method [Citation15].
Four other different studies have compared DA with CA, either for the group as a whole or for a single variable [Citation10–13] (). Two studies have presented results on group level, in which the DA is higher than the CA [Citation11,Citation13]. One of these studies lacks a control group, so no conclusions can be drawn regarding dental development [Citation13]. In the present study, the CG consisted of patients from orthodontic clinics who had a normal eruption of the maxillary canine. For ethical reasons, only patients with existing panoramic radiographs could be included in the CG.
Only one previous study has analyzed the impact of gender on DA among patients with IMC [Citation12]. Results similar to those of the present study were obtained, that is, the difference between DA and CA was statistically significant for both genders.
Regarding the relationship between the position of the IMC and the DA, previous studies have only compared DA with CA for patients with IMC. As mentioned earlier, comparisons of DA and CA may lead to biased absolute age differences owing to different errors of the method. Therefore, comparisons of DA involving a control group is more valid, as performed in the present study. In the present study, only patients with palatal IMC show delayed dental development. Although, the mean difference in DA between the IG and CG for palatal IMC was only 0.3 years. Therefore, this outcome would not support the theory regarding different aetiologies for buccal and palatal IMC, as proposed in several studies [Citation10,Citation12].
From the present study, it is evident from the DA assessment that patients with IMC display delayed dental development compared with patients with normally erupting canines. Although the absolute DA difference between the groups is of a magnitude that is of minor clinical relevance, this is essential knowledge for the crucial period of clinical monitoring of eruption of permanent canines. Early diagnosis and interceptive care for patients with ectopic canines are, therefore, possible in these patients as well.
Conclusion
Overall, the difference in dental development between patients with and without IMC is significant but small, and therefore, of minor clinical relevance. Female patients, patients in the chronological age groups of 12 and 13 years, and patients with palatally positioned IMC exhibit a minor but significant delay in their dental development assessment as DA. Thus, the timing of preventive care and treatment for patients with IMC should be the same as that for patients with normally erupting canines.
Author contributions
The responsibility of the conception and design of the study: all authors.
The responsibility of the acquisition of data: all authors.
The responsibility of data analysis: Mai Lin Lövgren and Anna Westerlund.
The responsibility of drafting the manuscript: Mai Lin Lövgren and Anna Westerlund.
The responsibility of revising the manuscript critically for important intellectual content: all authors.
The final version is approved to be published by all authors.
Acknowledgement
The authors thank the Public Dental Service, Region Västra Götaland for assistance with data extraction.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Chu FCS, Li TKL, Lui VKB, et al. Prevalence of impacted teeth and associated pathologies - a radiographic study of the Hong Kong Chinese population. Hong Kong Med J. 2003;9(3):158–163.
- Pedro FL, Bandeca MC, Volpato LE, et al. Prevalence of impacted teeth in a Brazilian subpopulation. J Contemp Dent Pract. 2014;15(2):209–213.
- Thilander B, Jakobsson SO. Local factors in impaction of maxillary canines. Acta Odontol Scand. 1968;26(2):145–168.
- Aktan AM, Kara S, Akgunlu F, et al. The incidence of canine transmigration and tooth impaction in a Turkish subpopulation. Eur J Orthod. 2010;32(5):575–581.
- Lovgren ML, Dahl O, Uribe P, et al. Prevalence of impacted maxillary canines-an epidemiological study in a region with systematically implemented interceptive treatment. Eur J Orthod. 2019;41(5):454–459.
- Litsas G, Acar A. A review of early displaced maxillary canines: etiology, diagnosis and interceptive treatment. Open Dent J. 2011;5:39–47.
- Naoumova J, Kurol J, Kjellberg H. Extraction of the deciduous canine as an interceptive treatment in children with palatal displaced canines - part I: shall we extract the deciduous canine or not? Eur J Orthod. 2015;37(2):209–218.
- Yan B, Sun Z, Fields H, et al. Maxillary canine impaction increases root resorption risk of adjacent teeth: a problem of physical proximity. Am J Orthod Dentofacial Orthop. 2012;142(6):750–757.
- Newcomb MR. Recognition and interception of aberrant canine eruption. The Angle Orthodontist. 1959;29(3):161–168.
- Becker A, Chaushu S. Dental age in maxillary canine ectopia. Am J Orthod Dentofacial Orthop. 2000;117(6):657–662.
- Rozylo-Kalinowska I, Kolasa-Raczka A, Kalinowski P. Dental age in patients with impacted maxillary canines related to the position of the impacted teeth. Eur J Orthod. 2011;33(5):492–497.
- Naser DH, Abu Alhaija ES, Al-Khateeb SN. Dental age assessment in patients with maxillary canine displacement. Am J Orthod Dentofacial Orthop. 2011;140(6):848–855.
- Sajnani AK, King NM. The sequential hypothesis of impaction of maxillary canine - a hypothesis based on clinical and radiographic findings. J Craniomaxillofac Surg. 2012;40(8):e375.
- Demirjian A, Goldstein H, Tanner JM. A new system of dental age assessment. Hum Biol. 1973;45(2):211–227.
- Maber M, Liversidge HM, Hector MP. Accuracy of age estimation of radiographic methods using developing teeth. Forensic Sci Int. 2006;159(1):S68–S73.
- Mani SA, Naing L, John J, et al. Comparison of two methods of dental age estimation in 7-15-year-old Malays. Int J Paediatr Dent. 2008;18(5):380–388.
- Mornstad H, Reventlid M, Teivens A. The validity of four methods for age determination by teeth in Swedish children: a multicentre study. Swed Dent J. 1995;19(4):121–130.
- Tunc ES, Koyuturk AE. Dental age assessment using Demirjian’s method on northern Turkish children. Forensic Sci Int. 2008;175(1):23–26.
- Koshy S, Tandon S. Dental age assessment: the applicability of Demirjian’s method in South Indian children. Forensic Sci Int. 1998;94(1–2):73–85.
- Aksglaede L, Sorensen K, Petersen JH, et al. Recent decline in age at breast development: the Copenhagen Puberty Study. Pediatrics. 2009;123(5):e932.
- Karpati AM, Rubin CH, Kieszak SM, et al. Stature and pubertal stage assessment in American boys: the 1988-1994 Third National Health and Nutrition Examination Survey. J Adolesc Health. 2002;30(3):205–212.
- Haavikko K. Tooth formation age estimated on a few selected teeth. A simple method for clinical use. Proc Finn Dent Soc. 1974;70(1):15–19.