Abstract
Introduction Hip dysplasia (HD) is assumed to be an etiological factor in the development of premature hip osteoarthrosis (OA). We established the prevalences of HD and OA in adults according to qualified radiographic discriminators, and investigated the relationship between HD and OA.
Methods Wiberg′s CE angle (CE), Sharp′s angle, the femoral head extrusion index, the acetabular depth ratio (ADR), the radiographic OA discriminators of Croft, and of Kellgren and Lawrence, and also minimum joint space width (JSW) ≤ 2 mm were applied to the standing, standardized pelvic radiographs of 1 429 men (22-93 years), and 2 430 women (22-92 years).
Results The 4 HD discriminators were interrelated. A negligible sex-related difference in acetabular morphology was found, male acetabulae being slightly more dysplastic than female acetabulae. However, differences between the sexes for right and left CE angles were within 1.0°, and within 1.4° for right and left Sharp′s angles. There were no cases of hip subluxation (breakage of Shenton′s line ≥ 5 mm). Average CE angle was 34° in men (SD 7.3°), and 35° in women (SD 7.6°). Applying a CE cut-off value of 20° for designation of definite hip dysplasia, we found a prevalence of hip dysplasia of 3.4%. Approximately 2% of cases were unilateral and 1.4% of cases were bilateral. We found significant relationships between radiographic OA discriminators and the CE angle, femoral head extrusion index and ADR. Odds ratios ranged from 1.0 to 6.2. Compared to subjects with OA in morphologically normal hips, a trend towards younger age in subjects with HD and OA was noted, but this was not strictly significant.
Interpretation We found that HD is not uncommon in the general population. The assumption that HD is an etiological factor in the development of hip OA was confirmed.
Hip dysplasia (HD) has been assumed to be a significant etiological factor in the development of premature hip osteoarthrosis (OA) in adults (Wiberg Citation1939, Severin Citation1941, Pauwels Citation1951, Stulberg and Harris Citation1974, Stulberg et al. Citation1975, Cooperman et al. Citation1983, Salter et al. Citation1984, Ganz Citation1988, Murphy et al. Citation1990, Croft et al. Citation1991, Hansson et al. Citation1993). To evaluate the magnitude of this predisposition, information on the prevalence of HD in the general population is required. To our knowledge, no such information exists in the literature. The prevalence of radiographic hip OA according to qualified discriminators is also required. We established the prevalence of HD in the adult cohort of 4 151 subjects from the Osteoarthrosis Substudy of the third Copenhagen City Heart Study, and investigated the relationship of HD to hip OA according to specified radiographic discriminators.
Material and methods
The osteoarthrosis substudy of the Copenhagen city heart study (CCHS III)
The CCHS is a longitudinal health survey of an adult cohort randomly selected from the residents of the county of Österbro in Copenhagen. The survey has been registering health and social factors pertaining to the participants since the beginning of 1976 (Schnohr et al. Citation2001).
From 1991 to 1994, antero-posterior (AP) pelvic and lumbar spine radiographs were recorded in 4 151 participants. There were 1 533 men with an average age of 62 (23-93) years, and 2 618 women with an average age of 65 (22-92) years. Radiographs were obtained in the standing position. The feet pointed straight forward, and the lower extremities were positioned in neutral abduction-adduction along the functional axis of the lower extremity. In AP pelvic radiographs, the X-ray beam was centered two finger-breadths over the symphysis pubis in the vertical midline. In lateral lumbar spine radiographs, the X-ray beam was centered at the apical midpoint of the iliac crista. Tube to film distance was 120 cm in all cases. All radiographs were taken by the same two radiography technicians.
Radiographic parameters of hip dysplasia
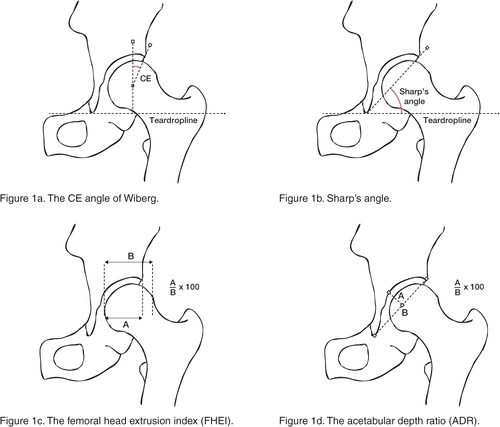
Acetabular morphology was assessed by the acetabular depth ratio (ADR) of Murray and Stulberg (cut-off value for definite dysplasia set at ≤ 250), and Sharp′s angle (cut-off value set at ≤ 45°). Containment of the femoral head by the acetabulum was assessed by Wiberg′s center-edge (CE) angle (cut-off value set at 20°), and the femoral head extrusion index of Heyman and Herndon (cut-off value set at ≥ 25%) (Wiberg Citation1939, Heyman and Herndon Citation1950, Sharp Citation1961, Murray Citation1965, Stulberg and Harris Citation1974) (). The center of the femoral head was localized using Mose′s template: a transparent plastic sheet with concentric, high-definition circles 1 mm apart. Sphericity of the femoral head was characterized using the following categories: 1) spherical, 2) coxae plana, and 3) irregular. Shenton′s line was evaluated. Pelvic rotation was assessed using Tönnis′ foramen obturator index (FOI), in which maximum horizontal width of the right obturator foramen was divided by left obturator foramen width (Tönnis Citation1976). Pelvic inclination was measured in lateral lumbar spine radiographs as the angle between the horizontal plane and a line parallel to the cranial articulating surface of the sacrum.
Radiographic parameters of hip OA
Minimum joint space width (JSW) was measured at three locations: 1) at the lateral margin of the subchondral sclerotic line ('the sourcil′), 2) at the apical transection of the weight-bearing surface by a vertical line through the center of the femoral head, and 3) at the medial margin of the weight-bearing surface bordering on the fovea. Minimum JSW was selected as the smallest of these 3 measurements. One observer (SJ) performed all measurements using a 0.1-mm graded magnifying glass.
Absence or presence of radiological OA was determined according to 1) the OA classification of Croft (grades 3-5), 2) Kellgren and Lawrence (KL) (grades 2-4) using a radiographic atlas (Kellgren and Lawrence Citation1957, Kellgren Citation1963, Croft et al. Citation1990) (), and 3) Minimum JSW ≤ 2 mm regardless of other features of OA, according to Lanyon et al. (Citation2003).
Table 1 Croft′s and Kellgren-Lawrence′s osteoarthritis scores for the hip joint
Exclusion criteria regarding radiographs
In a cadaver study, we have found that extreme pelvic rotation can have a significant influence on the radiological pelvic morphometry (Jacobsen et al. Citation2004). Keeping within ± 3° of error in measurements of the CE angle and Sharp′s angle, FOI inclusion limits of 0.7–1.8 were applied to radiographs.
We have found that extreme pelvic inclination during standing pelvic X-ray recordings constitutes a possible source of error for the precise measurement of JSW. Consequently, radiographs with pelvic inclinations outside 2 SD of the mean were omitted from the study. Median pelvic inclination was 38° (0–82), and 1 SD was 9.4°. Inclusion limits for pelvic inclination thus ranged from 19° to 56°. Radiographs in which measurements were inaccurate due to obesity of the subject were omitted.
Exclusion criteria regarding subjects
The following exclusion criteria were applied: 1) previous hip surgery of any hip except total hip arthroplasty, 2) previous fractures of any hip, 3) former treatment of childhood hip disorders, and 4) a history of rheumatoid arthritis or other inflammatory arthritis of any joint.
Reproducibility
Intraobserver reproducibility of measurements of JSW and index angles was assessed by blinded rereading (also by SJ) of a subset of 50 CCHS III radiographs 1 month after the first reading, using intraclass coefficients (ICC). Intraobserver reproducibility of Croft, and Kellgren and Lawrence OA grade assignments were performed in another subset of 100 radiographs after 1 month. Reproducibility of OA grading was assessed by kappa statistics.
Statistics
Interrelationships of radiographic HD discriminators were assessed by Spearman′s correlation coefficient. Sex-related differences of HD or minimum JSW were assessed by paired samples t-test. Age differences between subjects with hip OA and HD, and subjects with OA in morphologically normal hips were assessed by independent samples t-test. The relationship of HD to OA was investigated by chi-square tests and odds ratios.
A significance level of p < 0.05 was assumed. SPSS statistical software version 11.5 was used for all calculations (SPSS, Chicago, IL).
Results
Inclusion
Applying FOI limits of 0.7–1.8 meant that 188 of 4 151 (4.5%) of the CCHS-III pelvic radiographs had to be excluded from further analysis. Applying limits of pelvic inclination within 2 SD of the mean meant that an additional 34 cases (0.8%) had to be excluded. Applying individual exclusion criteria resulted in the final inclusion of 1 429 men with an average age of 61 (23–93) years, and of 2 430 women with an average age of 61 (22–92) years.
Reproducibility
ICC of JSW measurements ranged from 0.81 to 0.87. ICC of index angles ranged from 0.85 to 0.91. Repeatability of Croft′s OA grading was moderate; κ = 0.56 for the right hips, and κ = 0.46 for the left hips. If dichotomized into grades, 0°-3° denoting absent or slight OA, and grades 4°-5° denoting definite OA, kappa values increased to 0.65 for right hips, and 0.65 for left hips. Repeatability of K-L OA grading was κ = 0.55 for right hips, and κ = 0.51 for left hips. If dichotomised into grades, 0°-1° denoting absent or doubtful OA, and grades 2°-4° denoting definite OA, kappa values increased to 0.82 for right hips, and 0.85 for left hips.
Hip morphology
There were no cases of hip subluxation (breakage of Shenton′s line ≥ 5 mm). Interrelationships of the radiographic discriminators, basic values and sex-related differences in measured acetabular morphometry are summarized in . Sex-related distributions of right and left hip CE angles are presented in -. We found significant interrelationships between the radiographic discriminators of acetabular morphology (all p < 0.001). The correlation coefficient of Sharp′s angle to the 3 other HD discriminators was weakest. We found sex-related differences in acetabular morphology, male acetabulae being marginally more dysplastic than female acetabulae. However, mean differences between sexes for CE angles were within 1.0°, and for Sharp′s angles they were within 1.4°. For ADR, the mean difference between sexes was within 7%. For all practical clinical purposes, we find these differences negligible. In 3 770 hips (97.7%) the femoral head was spherical (mean CE angle 34.5°), and in 54 hips (1.4%) we found coxae plana (mean CE angle 34.2°). In 34 hips (0.9%), the femoral head was irregular in shape (mean CE angle 33.8°). There were no statistically significant differences between CE angles in normal, spherical femoral heads and the CE angles in flattened or irregular femoral heads.
Figure 2a Distribution of right hip CE angles.
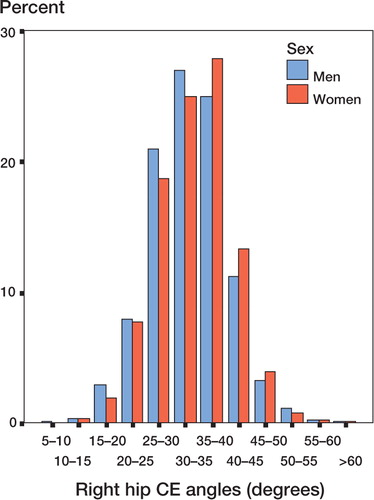
Figure 2b Distribution of left hip CE angles.
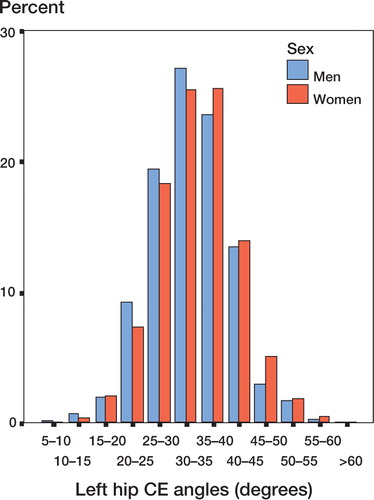
Table 2 Basic values, interrelationships and sex-related differences of Wiberg′s CE-angle, Sharp′s angle, the migration index of Heyman and Herndon and the acetabular depth ratio (ADR)
Prevalences of OA and HD
Mean minimum JSW was 3.6 (0.0–7.0) mm (SD 0.8 mm) for men, and 3.7 (0.0–8.0) mm (SD 0.8) for women. On average, minimum JSW for females was significantly larger than minimum JSW for males (p = 0.004). Applying the radiographic OA discriminators of Croft and of Lawrence and Kellgren, male hip OA ranged from 3.9% to 4.9%, and female hip OA ranged from 2.0% to 2.3%. The prevalences of radiographic hip OA became equalized if the discriminator of minimum JSW ≤ 2 mm (regardless of other features of OA) was applied ().
HD prevalences are summarized in . Although not strictly significant, we found a trend of subjects with OA and HD being younger than subjects with hip OA in normal hips ().
Table 3 Prevalences of hip OA and hip dysplasia
Table 4 Age differences between subjects with hip dysplasia and hip OA and subjects with hip OA in morphologically normal hips. OA discriminator: minimum JSW ≤ 2.0 mm
The relationship between HD and OA
We found statistically significant relationships between OA discriminators and the CE angle, the migration index, and ADR (). Odds ratios ranged from 1.0 to 6.2. The relationship between minimum JSW and the CE angle is presented graphically in .
Figure 3 The relationship between CE angle and minimum JSW.
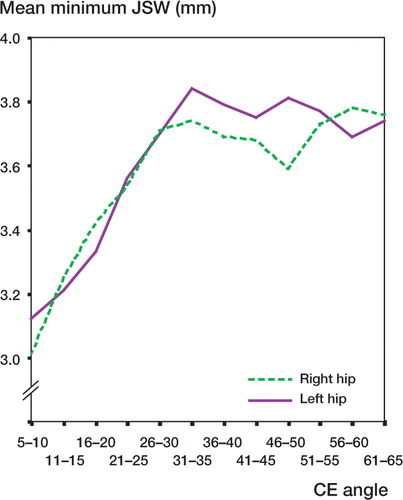
Table 5 The relationship between coxarthrosis and hip dysplasia for both sexes according to predefinitions (n = 3 859)
THA and HD
There were 43 right hip THAs and 34 left hip THAs at the time of the index radiographs. 12 subjects had bilateral THAs. We have no information on indication status for the THAs; nor have we access to preoperative radiographs. For unilateral THAs, we found no statistically significant differences in HD between the contralateral "healthy" hips and other hips that were included (with p ranging from 0.2 to 0.5 in right hips, and 0.2 to 0.6 in left hips).
Discussion
The etiology of hip OA is multifactorial. Mechanical and genetic factors seem to be most important (Cicuttini and Spector Citation1996, Spector et al. Citation1996, Jordan et al. Citation2000). Altered biomechanics of the hip caused by dysplasia and subluxation has been assumed to predispose it to osteoarthrosis (Wiberg Citation1939). In vivo and in vitro studies, as well as biomechanical computations, have shown that reduced areas of load transfer in dysplastic hips may lead to premature degeneration of cartilage (Afoke et al. Citation1987, Legal Citation1987, Hadley et al. Citation1990, Bergmann et al. Citation1993, Michaeli et al. Citation1997). However, while hip subluxation invariably seems to lead to early hip OA, the relationship between mild or moderate dysplasia and OA has not been clearly demonstrated. There have only been a few longitudinal studies, which included relatively few patients. Wiberg′s own longitudinal study (with a follow-up of 28 years) only included 44 patients, and 7 of the 17 hips illustrated in his original study were subluxated (Wiberg Citation1939, Cooperman et al. Citation1983). A significant relationship between dysplasia and degeneration has been confirmed lately by MRI and arthroscopy studies (Leunig et al. Citation1997, Citation2001, McCarthy et al. Citation2001, McCarthy and Lee Citation2002).
We have investigated the prevalence of acetabular dysplasia in the general population by applying commonly used radiographic discriminators of dysplasia to the pelvic radiographs of 3 859 subjects of the CCHS III cohort. A multitude of geometric radiographic indices for the description of hip morphology have been developed. We have chosen Wiberg′s CE angle, Sharp′s angle, the femoral head extrusion index and the acetabular depth ratio. These complement each other and are easy to use in clinical and epidemiological studies.
The CE angle decreases in acetabular dysplasia and coxa magna, which increases the head radius. The center of the head becomes displaced laterally and inferiorly. If subluxation occurs, it may move further laterally and superiorly. The angle increases in coxa plana, where the center of the femoral head moves cranially, and in OA where the center of the head migrates cranially due to reduced cartilage height. In adults, Stulberg found average angles of 37° (26–48) in men, and 35° (24–46) in women. Murphy found angles averaging 37°. Cut-off value for definite dysplasia varies considerably. Wiberg found a physiological range of 20–40° in normal adults. Tönnis estimated normal values between 26° and 30° at 17–20 years of age. The same range was found by Fredensborg in adults. A CE angle of less than 20° is considered by most investigators to be diagnostic of definitive acetabular dysplasia, while a CE angle of 25–20° is considered to be borderline normal (Stulberg and Harris Citation1974, Fredensborg Citation1976, Tönnis Citation1976, Murphy et al. Citation1990, Delaunay et al. Citation1997). This parameter has some limitations. The CE angle relates acetabular coverage to the position of the femoral head and is dynamic in nature, but does not indicate the shape or depth of the acetabulum. It does not assess vertical migration of the femoral head: in cases with borderline subluxation and broken Shenton′s line, the CE angle may be the same as in the purely dysplastic joint. The true lateral acetabular margin is difficult to identify in many AP radiographs. The lateral margin may be obscured by the supero-pos-terior curvature, osteophytes, or the most lateral portion of the acetabular surface may be so oblique that it does not participate in the actual articulation. We have chosen to designate the readily identifiable lateral margin of the subcondral sclerotic 'sourcil′ (Fr: eyebrow) as our lateral point of reference (Katz Citation1979).
Qualified radiographic case definitions of both OA and HD and proper size of the background material are essential in the study of childhood hip diseases and secondary development of OA. We have found that most studies investigating this relationship have been based on urograms and colon radiographs, with little or no information on tube-to-film distance, pelvic orientation, magnification, or centering of the X-ray beam (Croft et al. Citation1991, Lau et al. Citation1995, Smith et al. Citation1995, Lavy et al. Citation2003). Furthermore, most OA case definitions used have either been Croft′s classification based solely on male urograms, or the classification of Lawrence and Kellgren, which is notoriously problematic regarding reproducibility (Sun et al. Citation1997).
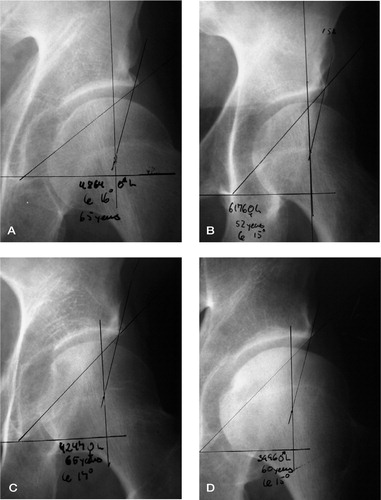
The assumption of HD being prearthrotic was confirmed in this study, with odds ratios ranging from 1.0 to 6.2. Mild to moderate HD is not an unusual condition in the population; prevalences range from 3.5% to 10.7% depending on the index used. Also, we established a trend for subjects with OA and HD being somewhat younger than subjects with hip OA in normal hips. Using the Croft or Kellgren and Lawrence OA classifications emphasizing the formation of subcondral sclerosis and osteophytes, there is a tendency to overestimate male OA prevalence, while underestimating female OA prevalence. If minimum JSW ≤ 2.0 mm was used exclusively as the OA discriminator, female hip OA prevalence superseded male prevalences in older age groups. HD is only one of several factors influencing the development of hip OA. Age and genetic factors are also important. During the reading of radiographs, we have encountered several cases of HD in elderly subjects with no radiological signs of OA ().
Figure 4 Moderate hip dysplasia without radiological signs of osteoarthrosis. A: male, 65 years, left hip; CE = 16°. B: female, 52 years, left hip; CE = 15°. C: female, 65 years, left hip; CE = 17°. D: male, 60 years, left hip; CE = 15°.
During the past decade, pelvic realignment osteotomies in younger adults with HD have become increasingly popular to prevent secondary OA (Ganz et al. Citation1988, Søballe Citation2003). This development has precipitated the need for further research in this field. Longitudinal studies of larger cohorts, to establish the range and rate at which secondary OA develops in response to incongruency of the hip joint, are especially relevant.
This study was financially supported by the Research Board of the National University Hospital of Rigshospitalet, the Danish Medical Research Council, the Danish Rheumatism Association, the SAHVA Foundation, Sygekassernes Helsefond, and Biomet-Merck Ltd., Denmark.
No competing interests declared.
Related Research Data
- Afoke N Y P, Byers P D, Hutton W C. Contact pressures in the human hip joint. J Bone Joint Surg (Br) 1987; 69: 536–41
- Bergmann G, Graichen F, Rohlmann A. Hip joint loading during walking and running, measured in two patients. J Biomechanics 1993; 26: 969–90
- Cicuttini F M, Spector T D. Genetics of osteoarthritis. Ann Rheum Dis 1996; 55: 665–7
- Cooperman D R, Wallensten R, Stulberg S D. Acetabular dysplasia in the adult. Clin Orthop 1983, 175: 79–85
- Croft P, Cooper C, Coggon D. Case definition of hip osteoarthritis in epidemiologic studies. Am J Epidemiol 1990; 132: 514–22
- Croft P, Cooper C, Wickham C, Coggon D. Osteoarthritis of the hip and acetabular dysplasia. Ann Rheum Dis 1991; 50: 308–10
- Delaunay S, Dussault R G, Kaplan P A, Alford B A. Radiographic measurements of dysplastic adult hips. Skeletal Radiol 1997; 26: 75–81
- Fredensborg N. The CE angle of normal hips. Acta Orthop Scand 1976; 47: 403–5
- Ganz R, Klaue K, Vinh T S, Mast J W. A new periacetabular osteotomy for the treatment of hip dysplasias. Technique and preliminary results. Clin Orthop 1988, 232: 26–36
- Hadley N A, Brown T D, Weinstein S L. The effects of contact pressure elevations and aseptic necrosis on the long-term outcome of congenital hip dislocation. J Orthop Res 1990; 8: 504–13
- Hansson G, Jerre R, Sanders S M, Wallin J. Radiographic assessment of coxarthrosis following slipped capital femoral epiphysis. Acta Radiol 1993; 34: 117–23
- Heyman C H, Herndon C H. Legg-Perthes disease. A method for the measurement of the roentgenographic result. J Bone Joint Surg (Am) 1950; 32: 767–78
- Jacobsen S, Sonne-Holm S, Lund B, Søballe K, Kiær T, Rovsing H, Monrad H. Pelvic orientation and assessment of hip dysplasia in adults. Acta Orthop Scand 2004; 75: 721–9
- Jordan J M, Kington R S, Lane N E, Nevitt M C, Zhang Y, Sowers M. Systemic risk factors for osteoarthritis. Ann Intern Med 2000; 133: 637–9
- Katz J F. Precise identification of radiographic acetabular landmarks. Clin Orthop 1979, 141: 166–8
- Kellgren J H. The epidemiology of chronic rheumatism. Volume II: Atlas of standard radiographs of arthritis. Blackwell Scientific Publications, Oxford 1963; 1–44
- Kellgren J H, Lawrence J S. Radiological assessment of osteo-arthritis. Ann Rheum Dis 1957; 16: 494–502
- Lanyon P, Muir K, Doherty S, Doherty M. Age and sex differences in hip joint space among asymptomatic subjects without structural change: implications for epidemiologic studies. Arthritis Rheum 2003; 48: 1041–6
- Lau E M, Lin F, Lam D, Silman A, Croft P. Hip osteoarthritis and dysplasia in Chinese men. Ann Rheum Dis 1995; 54: 965–9
- Lavy C, Msamati B, Igbigbi P. Racial and gender variations in adult hip morphology. Int Orthop 2003; 27: 331–3
- Legal H. Introduction to the biomechanics of the hip. Congenital dysplasia and dislocation of the hip, D Tönnis. Springer-Verlag, Berlin-Heidelberg-New York 1987; 26–56
- Leunig M, Werlen S, Ungersbock A, Ito K, Ganz R. Evaluation of the acetabular labrum by MR arthrography. J Bone Joint Surg (Br) 1997; 79: 230–4
- Leunig M, Siebenrock K A, Ganz R. Rationale of periacetabular osteotomy and background work. Instr Course Lect 2001; 50: 229–38
- McCarthy J C, Lee J A. Acetabular dysplasia: a paradigm of arthroscopic examination of chondral injuries. Clin Orthop 2002, 405: 122–8
- McCarthy J C, Noble P C, Schuck M R, Wright J, Lee J. The Otto E. Aufranc Award: The role of labral lesions to development of early degenerative hip disease. Clin Orthop 2001, 353: 25–37
- Michaeli D A, Murphy S B, Hipp J A. Comparison of predicted and measured contact pressures in normal and dysplastic hips. Med Eng Phys 1997; 19: 180–6
- Murphy S B, Kijewski P K, Millis M B, Harless A. Acetabular dysplasia in the adolescent and young adult. Clin Orthop 1990, 261: 214–23
- Murray R O. The aetiology of primary osteoarthritis of the hip. Brit J Radiol 1965; 38: 810–24
- Pauwels F. Des affections de la hanche d′origine mechanique et de leur traitment par l′osteotomie d′adduction. Rev Chir Orthop 1951; 37: 221–8
- Salter R B, Hansson G, Thompson G H. Innominate osteotomy in the management of residual congenital subluxation of the hip in young adults. Clin Orthop 1984, 182: 53–68
- Schnohr P, Jensen G, Lange P, Scharling H, Appleyard M. The Copenhagen city heart study -Österbroundersøgelsen - tables with data from the third examination 19911994. Eur Heart J 2001, Suppl 3: 1–83, H
- Severin E. Contribution to the knowledge of congenital dislocation of the hip joint. Acta Orthop Scand 1941, Suppl 63: 45–54
- Sharp I. Acetabular dysplasia. J Bone Joint Surg (Br) 1961; 43: 268–72
- Smith R W, Egger P, Coggon D, Cawley M I, Cooper C. Osteoarthritis of the hip joint and acetabular dysplasia in women. Ann Rheum Dis 1995; 54: 179–81
- Spector T D, Cicuttini F, Baker J, Loughlin J, Hart D. Genetic influences on osteoarthritis in women: a twin study. BMJ 1996; 312: 940–3
- Stulberg S D, Harris W H (1974) Acetabular dysplasia and development of osteoarthritis of hip. The hip. Proceedings of the second open scientific meeting of the hip society. 1974. C.V.Mosby, St. Louis, 82–93
- Stulberg S D, Cordell L D, Harris W H, Ramsey P L, MacEwen G D (1975) Unrecognized childhood hip disease: a major cause of idiopathic osteoarthritis of the hip. Proceedings of the third open scientific meeting of the hip society. 1975. C.V.Mosby, St. Louis, 212–28
- Sun Y, Günther K P, Brenner H. Reliability of radiographic grading of osteoarthritis of the hip and knee. Scand J Rheumatol 1997; 26: 155–65
- Søballe K. Pelvic osteotomy for acetabular dysplasia. Acta Orthop Scand 2003; 74: 117–8
- Tönnis D. Normal values of the hip joint for the evaluation of X-rays in children and adults. Clin Orthop 1976, 119: 39–47
- Wiberg G. Studies on dysplastic acetabula and congenital subluxation of the hip joint. Acta Orthop Scand 1939, Suppl 58: 1–132