Abstract
Background The annual number of total hip arthroplasties (THA) has increased in Denmark over the past 15 years. There is, however, limited detailed data available on the incidence of THAs.
Methods We calculated the incidence rates (IR) of primary THA and revision in Denmark between 1996 and 2002 and estimated the demands for primary THA in Denmark until 2020. We used data from the Danish Hip Arthroplasty Registry, a nationwide and popula-tion-based clinical database, to identify patients who had undergone primary THA (n = 37 144) or revision arthroplasties (n = 6 446). Age and sex-specific data on the Danish population were obtained from the StatBank Denmark. All IRs were standardized according to two standards, i.e. the Danish population in 1996 and the European standard population (18 age groups). The future demands for primary THA were estimated using the age and sex-specific incidence of primary THA for 2002 as a reference, and taking into account the expected changes in the age distribution of the population and the trend in IRs seen in Denmark between 1996 and 2002.
Results The annual overall standardized IRs of primary THAs and revisions increased from 101 (95% confidence interval (CI): 97.6–104) to 134 (CI: 131–138) and from 19.2 (CI: 17.9–20.5) to 21.1 (CI: 19.8–22.4) per 100 000 inhabitants from 1996 to 2002, respectively (IRs adjusted to the Danish population in 1996). The IRs of primary THAs and revisions increased by 30% and 10% during this period. The relative increase in IRs of primary THAs was found to be similar in both women and men. The increase was higher among patients aged 50–59 years, however. Furthermore, a decrease in IRs was seen in patients who underwent primary THA due to rheumatoid arthritis. IRs of primary THAs have been estimated to increase by 22% in 2020 compared with 2002, based only on the expected changes in the age distribution of the population. However, assuming that the annual age and sex-independent increase in the IRs seen in the period 1996–2002 will continue, the IR of primary THA is estimated to increase by as much as 210% in 2020.
Interpretation The overall annual standardized IRs of primary THAs and revisions in Denmark increased during the period from 1996 to 2002. Moreover, the demands for THA procedures in the coming decades may exceed the current capacity due to the ageing population and a continued age and sex-independent increase in surgical activity.
The annual number of THA procedures has been rising steadily worldwide during the past decades, due to the improvements in surgical technique and the increasing number of elderly people in most Western populations (Havelin et al. Citation2000, Ingvarsson Citation2000, Puolakka et al. Citation2001, Söderman et al. Citation2001, Malchau et al. Citation2002, Ostendorf et al. Citation2002, Mahomed et al. Citation2003). However, there are substantial differences between the reported THA incidence rates (IR) in Europe, the United States, Canada, and Australia (Merx et al. Citation2003).
It has been suggested that the future demands for THA may exceed the current capacity for THA procedures (Birrell et al. Citation1999, Ingvarsson Citation2000). There is a limited amount of data on the incidence of THAs in Denmark (Lucht Citation2000) and, in general, there have been few studies dealing with estimated future demands (Overgaard et al. Citation1992). In order to predict the need for THA procedures in the coming years, it is necessary to estimate the incidence of THA in the context of changing population demographics. The objective of this study was therefore to estimate the IRs of primary THAs and revisions in Denmark in the period 1996–2002 using data from the Danish Hip Arthroplasty Registry, and also to estimate the demands of primary THA to be expected in Denmark in the coming decades.
Methods
Study population
The Danish Hip Arthroplasty Registry (DHR).The DHR is a population-based clinical database, which was started in 1995. The goals of the database are to define the epidemiology of THA procedures in Denmark, to provide timely information on risk factors for revision, and to provide data that may improve and maintain the quality of outcome in hip replacement surgery at both local and national levels. The registry contains pre-, per- and postoperative data about primary THAs and revisions, collected using a standardized form. Registration of primary THAs and revisions is obligatory, whereas registration of follow-up examinations is voluntary (Lucht Citation2000).
The quality of data in the DHR has recently been examined and found to be high, i.e., the registration completeness for THA procedures is 94% and the positive predictive values of the registered diagnoses in patients undergoing primary THAs have been shown to be between 81% and 100%, except for fresh fracture of the proximal femur (Pedersen et al. Citation2004). A total of 50 113 procedures, both primary THAs (n = 42 624) and revisions (n = 7 489), have been registered in the DHR since 1995. However, in the present study, we excluded the year 1995 from the analysis because of its relatively low registration completeness (88%). Also, due to a strike among Danish nurses in 1995, the numbers of primary THAs and revisions in Denmark during that year were unusually low. Thus, we studied the period from January 1, 1996 through December 31, 2002.
We excluded procedures which occurred before and after the study period (n = 5 472) and patients who were erroneously registered with a third primary THA (n = 8), from the analysis of primary THAs. This left 37 144 primary THA procedures (87.1% of the initial 42 624) for further analysis. We also excluded procedures that occurred outside of the study period (n = 1 043) from the analysis of revisions, leaving 6 446 revisions (86.1% of the initial 7 489).
The StatBank Denmark.The StatBank Denmark is a database which contains detailed statistical information on the Danish population (http://statis-tikbanken.dk/). At the middle of each calendar year, we obtained data on the population size-including estimates for the coming years-by age and sex.
Analyses
Incidence rates.We estimated annual overall IRs of primary THAs or revisions as the number of patients undergoing primary THA or revision by calendar year, divided by the total number of individuals at risk in Denmark. Age and gender-specific annual IRs were also estimated. Age was divided into five groups: 10–49, 50–59, 60–69, 70–79, and more than 80 years. Annual IRs of primary THAs were also estimated separately and according to diagnosis (primary arthrosis; rheumatoid arthritis; late sequelae from fracture of the proximal femur; atraumatic necrosis of femoral head and hip disorders in childhood, including congenital hip dislocation, morbus Calvé-Legg-Perthes, epiphysiolysis, and acetabular dysplasia).
All IRs were standardized to the age distribution of the Danish population in 1996 and expressed per 100 000 inhabitants, with 95% confidence intervals (CI). Poisson regression was used to estimate incidence rate ratios (IRR), using the year 1996 as the reference. Here, IRR expresses the relative change in IRs of primary THAs or revisions in 1997–2002 compared with IRs in the reference category. To examine possible differences in IRs according to different ways of standardization and in order to increase the comparability of our study with studies based on other populations, we also calculated annual overall IRs of primary THAs and revisions using the European Standard Population (divided into 18 age groups) within SEER*Stat (http:// www-dep.iarc.fr/dattaava/ewstdpop.htm).
Predictions for the years 2010, 2015, and 2020.We estimated the future demands for primary THA in Denmark using the age-specific IRs of primary THAs for year 2002 as a reference, based on two different scenarios: A) with the expected changes in the age distribution of the population, and B) with the combined effect of the expected changes in the age distribution of the population and a continued relative annual age and sex-specific increase in the age-standardized IRs (based on the development in the period 1996–2002).
In scenario A, the predicted number of primary THAs in 2010 (A2010 (total)) was estimated using the following equation:
where IR2002 (i) represents the age-specific IRs of primary THAs in 2002, and POP2010 (i) is the predicted age-specific population in 2010 (i = 1 to 5 relates to five age-groups, separately for males and females).
In scenario B, the predicted number of primary THAs in 2010 (B2010 (total)) was estimated using the following equation:
where the trend is the continued relative annual age and sex-specific increase in the age-standard-ized IRs. The trend was estimated with the Poisson regression model.
The predicted numbers of primary THAs and corresponding IRs for years 2015 and 2020 were estimated in the same way, except that specific age distributions and trends in IRs for years 2015 and 2020 (respectively) were used.
Statistics
All analyses were performed using Stata statistical software (Release 8.0; Stata Corp., TX).
Results
shows the baseline characteristics of the THA patients registered in the DHR from 1996 to 2002.
Table 1. Characteristics of the total hip arthroplasty (THA) patients registered in the DHR, 1996–2002
Overall IRS standardized to the Danish population in 1996
Annual standardized IRs of primary THAs and revisions increased steadily during the period 1996–2002 in Denmark. For primary THAs, the overall annual IR increased from 101 (95% CI: 98–104) in 1996 to 131 (CI: 128–135) in 2002 per 100 000 inhabitants. For revisions, the annual standardized IRs increased from 19.2 (CI: 17.9–20.5) to 20.7 (CI: 19.4–22.1) per 100 000 inhabitants in the same period. The corresponding IRRs for primary THAs and revisions were 1.3 (CI: 1.3–1.4) and 1.1 (CI: 0.9–1.4), respectively, when comparing 2002 with 1996.
IRS standardized to the European standard population
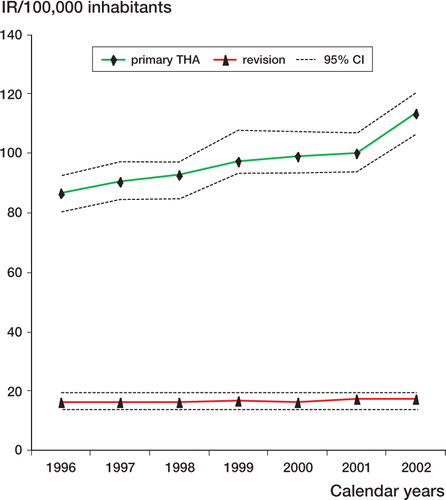
IRs of primary THAs and revisions were lower when we used the age distribution of the European Standard Population (18 age groups). Thus, IRs of primary THAs increased from 86.7 (CI: 80.7–92.8) in 1996 to 113 (CI: 107–121) in 2002 per 100 000 inhabitants, and IRs of revisions increased from 16.4 (CI: 14–19.7) in 1996 to 17.3 (CI: 14.2–19.5) in 2002 per 100 000 inhabitants (). The corresponding IRRs for primary THAs and revisions were the same as those found after standardization to the Danish population in 1996.
Figure 1. Incidence rates (IR) of primary THAs and revisions standardized to the European Standard Population (18 age groups).
IRS according to gender and age
The relative increase in IRs of primary THAs was found to be similar in both females and males. The IRs of primary THAs increased from 114 (CI: 109–118) to 153 (CI: 148–158) among women and from 87 (CI: 83–90) to 114 (CI: 110–119) among men per 100 000, from 1996 through 2002, respectively. In terms of sex differences, IRs of revisions followed the same pattern.
Age-specific IRs of primary THAs increased according to age, being highest among individuals aged 70–79 (IRR = 45.6, CI: 43.6–47.7) in comparison to individuals aged 10–49 (). IRs of revisions according to age followed the same pattern. The increase in IRs of primary THAs was found in all five age groups during the period 1996–2002, being highest among people aged 50–59 (43%) and lowest among people aged 10–49 (17%).
Table 2. Annual age and sex-specific incidence rates (IRs) of primary THA per 100 000 inhabitants in Denmark, 1996–2002
IRS according to diagnosis
shows the development in IRs of primary THA according to selected diagnoses. The IRR due to primary arthrosis was 1.4 (CI: 1.3–1.4) in 2002 compared with 1996, and an increase was also seen for most other diagnoses (IRRs were between 1.1 and 1.3). In contrast, IRs of primary THAs due to rheumatoid arthritis decreased in the same period, with an IRR of 0.7 (CI: 0.6–0.9) when comparing 2002 with 1996.
Table 3. Estimates of incidence rates and incidence rate ratios of THA between 1996 and 2002 according to diagnosis in patients undergoing primary operation (Poisson regression)
Predictions for the years 2010, 2015, and 2020
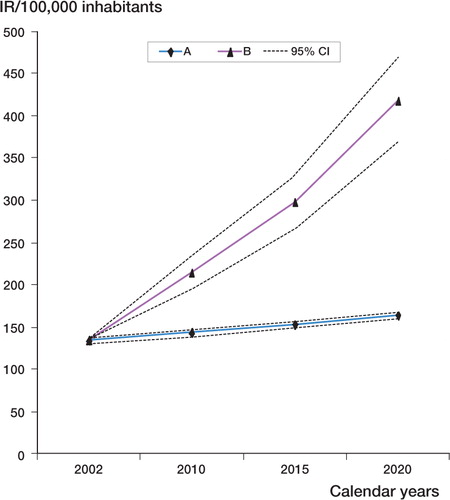
shows expected IRs of primary THAs according to two scenarios in the coming decades. The lower line, A, shows IRs based on the expected changes in the age distribution of the population. IRs in this scenario will increase continuously from 2002, and would be expected to be 143 (CI: 140–147), 154 (CI: 150–157), and 164 (CI: 161–168) per 100 000 in years 2010, 2015, and 2020, respectively (that is, an increase of 22% in 2020 compared with 2002). The upper line, B, shows the increase in IRs that is expected if changes in the age distribution are combined with a continued annual age and sex-specific increase in the age-standardized IRs of primary THA observed in the period 1996–2002. With this scenario, we would expect an IR of 417 (CI: 370–470) per 100 000 in 2020. This corresponds to an increase of 210% in 2020 compared with 2002. The 95% CI includes uncertainties related to both the population prediction and the estimation of trend.
Figure 2. Expected incidence rates (IRs) of primary THAs in Denmark in the years 2010, 2015, and 2020, based on constant age-specific IRs of primary THAs (2002). A: with expected changes in age distribution. B: with expected changes in age distribution combined with the continued annual age and sex-specific increase in the standardized IRs of primary THA based on figures from 1996–2002.
Discussion
The strengths of our study include access to information on THA procedures from a nationwide pop-ulation-based clinical database with documented high data-validity (Pedersen et al. Citation2004). Furthermore, detailed demographic data on the Danish population were available, including predictions of its future development. Age-standardization of the estimated IRs was performed according to both a Danish and a European standard population, to permit comparisons over time and with other populations.
The limitations of the study include a moderate completeness of registration of revisions in the DHR (81%). The accuracy of the expected IRs of primary THAs in the future is highly dependent on the accuracy of the assumptions made by Statistics Denmark when estimating the size and age distribution of the Danish population in the coming decades. However, the predictions are very sensitive to even minor changes in the age-independent IRs, resulting in substantial uncertainty about the future IRs, as indicated by the large difference between scenarios A and B.
Some difficulties arise when making comparisons of our results with other countries, due to differences in the age distribution of the populations, methods of collecting and reporting the data, and study periods. Most of the published studies on the incidence of THA have only reported crude data, making direct comparisons with data from other studies difficult. Ingvarsson (Citation2000) has demonstrated the importance of using age-standardized IRs; for example, crude overall IRs in Iceland and Sweden were almost identical, but after age standardization the incidence of THA was at least 50% higher in Iceland than in Sweden. Although some of the existing studies have performed age standardization, it is often difficult to know from the papers which standard populations were used (Hoaglund et al. Citation1995, Ingvarsson Citation2000, Wells et al. Citation2002, Mahomed et al. Citation2003).
Including age-standardized results-preferably to a generally accepted international standard pop-ulation-in future reports on IRs of THA would be a relatively simple way of enabling valid and useful worldwide comparisons of IRs.
Overall IRS of primary thas and revisions
Despite the problems with lack of age standardization, the steady increase in IRs of primary THAs and revisions found in our study appears to be consistent with the reports from a number of other countries. Increases in IRs were reported in Finland during 1988 through 1999 (Puolakka et al. Citation2001), Norway during 1995 through 1999 (Havelin et al. Citation2000), Sweden during 1995 through 2000 (Malchau et al. Citation2002), Canada during 1994 through 2000 (Bourne et al. 2004), and Australia during 1999 through 2002 (Graves et al. Citation2004). These IRs were based on data from the national registries and included primary THA due to all diagnoses.
Increase in IRs of primary THAs varies from 20% to 60% between different countries (Mahomed et al. Citation2003, Ostendorf et al. Citation2002, Söderman et al. Citation2001). The increase in IRs of THA procedures may be due to a number of factors, including changes in the clinical criteria for performing THA, e.g. increased acceptance among clinicians and patients of performing THA on younger and older patients, or patients with severe comorbidity. Other factors which might affect the increase in IRs of THA are increased demand from patients, implementation of financial incitements for increasing the surgical throughput, and changes in the organization of the health care system-with the formation of fewer but more specialised and efficient units with a high operating volume.
The crude IRs of primary THA found in Iceland in age groups 49–59 and < 59 years, were two to three times higher than corresponding IRs in Denmark (Ingvarsson Citation2000). The differences may be related to a higher prevalence of primary hip osteoarthrosis in Iceland compared with other Nordic countries (Ingvarsson et al. Citation1999), or onset of osteoarthrosis at an earlier age. Mahomed et al. (Citation2003) reported IRs of revision in 1995–1996 to be 3 to 6 times lower than IRs of primary
THA, which agrees with our findings. Because most of the studies have reported the annual number of revisions but not IRs of revision, it is difficult to make comparisons. The overall ratio between revisions and THA procedures found in our study was higher than in Sweden, but comparable to that of Norway (Havelin et al. Citation2000).
IRS according to sex and age
The higher IRs of THA procedures in women found in our study and the results of others generally agree (Overgaard et al. Citation1992, Peterson et al. 1992, Ingvarsson Citation2000, Malchau et al. Citation2002, Mahomed et al. Citation2003). This may be explained by higher risk of osteoarthrosis in women. Osteoarthrosis has been described as the most frequent and disabling chronic disease among women (Callahan et al. 1996, Creamer and Hochberg Citation1997). Hawker et al. (2001) reported that the potential need for arthroplasty among women would be even higher than indicated by the IRs of THA, if the lower willingness to undergo surgery is taken into account. However, an increased risk of osteoarthrosis is probably not the only explanation, since the proportion of women within most of the diagnostic groups (except for atraumatic necrosis of the femoral head) was more than 70% in our study.
The IRs peaked for persons aged 70–79 years, which also agrees with the findings from other studies (Ingvarsson Citation2000, Söderman et al. 2000, Wells et al. Citation2002, Mahomed et al. Citation2003). Overgaard et al. (1992) reported the same pattern in Denmark from 1981 to 1990. However, the highest increase in IRs in the period 1996–2002 was seen among people aged 50–59. This may indicate that today, patients and surgeons prefer treatment at an earlier stage of their disease.
IRS according to diagnosis
The decrease in IRs of primary THAs due to rheumatoid arthritis, found in our study, has also been seen in Sweden (Malchau et al. Citation2002). This can be explained by the progressive decline in the incidence of rheumatoid arthritis seen in a number of populations over the last few decades (Kaipiainen-Seppanen et al. 2001, Doran et al. 2002, Symmons et al. 2002). There is further evidence that rheumatoid arthritis is less severe now than it was about 30 years ago (Silman Citation2002). It has been suggested that the improved outcome of rheumatoid arthritis reflects the introduction of modern drug treatment, although there is no evidence that mortality of rheumatoid arthritis has decreased during this time (Doran et al. 2002).
Predictions for the years 2010, 2015, and 2020
Very few studies have reported the expected future demands of THAs (Overgaard et al. Citation1992, Birrell et al. Citation1999, Ostendorf et al. Citation2002). The existing predictions have, however, been based on demographic projections only and 2 of the reports did not include estimates of the IRs. The increase in IRs of primary THAs from 2002 to 2020 in Denmark found in our study, based only on the expected changes in the age distribution of the population, was lower than corresponding estimates projected in the Netherlands, Sweden, and England. This may reflect true differences; however, it may also be related to inaccuracies in the demographic projections or to the fact that the studies were not conducted at exactly the same time. At the moment, it seems unlikely that the annual age-independent increase in IRs of primary THA will continue to be 5% in the coming decades. Such a development would represent a serious economic challenge for the health care system, and allocation of sufficient economic resources and staff would be problematic.
The waiting time for THA did not become shorter in Denmark between 1996 and 2002 (http://www. venteinfo.dk/ventelister/visventetider.asp), despite the substantial increase in surgical activity, and reports indicate that current demands for THA procedures do not appear to have been met yet (Bourne et al. Citation2004). In conclusion, the overall annual IRs of primary THAs and revisions in Denmark have increased substantially during the period from 1996 to 2002. Also, the demands for THA procedures in the coming decades may increase dramatically due to the ageing population and to a continued age-independent increase in surgical activity.
This study was supported by the Danish Rheumatism Association, the Oldermand Slagtermester Peter Ryholts Grant, the Orthopedic Research Foundation in Aarhus, Aarhus University Hospitals Research Initiative from Aarhus County, Lægekredsforeningen for Aarhus County Research Foundation and Aarhus University.
The authors thank Prof. Otto Sneppen of the Department of Orthopedic Surgery, Aarhus University Hospital, and Anne Hjelm, secretary of the Danish Hip Arthroplasty Register. We are also grateful to all orthopedics departments in Denmark for their assistance.
No competing interests declared.
Related Research Data
- Birrell F, Johnell O, Silman A. Projecting the need for hip replacement over the next three decades: influence of changing demography and threshold for surgery. Ann Rheum Dis 1999; 58(9)569–72
- Bourne R B, Maloney W J, Wright J G. An AOA critical issue the outcome of the outcomes movement. J Bone Joint Surg (Am) 2004; 86(3)633–40
- Callahan L F, Rao J, Boutaugh M. Arthritis and women′s health: prevalence, impact, and prevention. Am J Prev Med 1996; 12(5)401–9
- Creamer P, Hochberg M C. Osteoarthritis. Lancet 1997; 350(9076)503–8
- Doran M F, Pond G R, Crowson C S, O′Fallon W M, Gabriel S E. Trends in incidence and mortality in rheumatoid arthritis in Rochester, Minnesota, over a forty-year period. Arthritis Rheum 2002; 46(3)625–31
- Graves S E, Davidson D, Ingerson L, Ryan P, Griffith E C, McDermott B F, McElroy H J, Pratt N L. The Australian orthopaedic association national joint replacement registry. Med J Aust 2004; 180: S31–S34, (5 Suppl)
- Havelin L I, Engesaeter L B, Espehaug B, Furnes O, Lie S A, Vollset S E. The Norwegian Arthroplasty Register:. Acta Orthop Scand 2000; 71(4)337–53
- Hawker G A, Wright J G, Coyte P C, Williams J I, Harvey B, Glazier R, Wilkins A, Badley E M. Determining the need for hip and knee arthroplasty: the role of clinical severity and patients′ preferences. Med Care 2001; 39(3)206–16
- Hoaglund F T, Oishi C S, Gialamas G G. Extreme variations in racial rates of total hip-arthroplasty for primary coxarthrosis – A population-based study in San-Francisco. Ann Rheum Dis 1995; 54(2)107–10
- Ingvarsson T. Prevalence and inheritance of hip osteoarthritis in Iceland. Acta Orthop Scand 2000; 1–46, (Suppl 298)
- Ingvarsson T, Hagglund G, Lohmander L S. Prevalence of hip osteoarthritis in Iceland. Ann Rheum Dis 1999; 58(4)201–7
- Kaipiainen-Seppanen O, Aho K, Nikkarinen M. Regional differences in the incidence of rheumatoid arthritis in Finland in 1995. Ann Rheum Dis 2001; 60(2)128–32
- Lucht U. The Danish Hip Arthroplasty Register. Acta Orthop Scand 2000; 71(5)433–9
- Mahomed N N, Barrett J A, Katz J N, Phillips C B, Losina E, Lew R A, Guadagnoli E, Harris W H, Poss R, Baron J A. Rates and outcomes of primary and revision total hip replacement in the United States medicare population. J Bone Joint Surg (Am) 2003; 85(1)27–32
- Malchau H, Herberts P, Eisler T, Garellick G, Soderman P. The Swedish Total Hip Replacement Register. J Bone Joint Surg (Am) 2002; 84: 2–20, (Suppl 2)
- Merx H, Dreinhofer K, Schrader P, Sturmer T, Puhl W, Gunther K P, Brenner H. International variation in hip replacement rates. Ann Rheum Dis 2003; 62(3)222–6
- Ostendorf M, Johnell O, Malchau H, Dhert W J, Schrijvers A J, Verbout A J. The epidemiology of total hip replacement in The Netherlands and Sweden: present status and future needs. Acta Orthop Scand 2002; 73(3)282–6
- Overgaard S, Knudsen H M, Hansen L N, Mossing N. Hip arthroplasty in Jutland, Denmark. Age and sex-specific incidences of primary operations. Acta Orthop Scand 1992; 63(5)536–8
- Pedersen A B, Johnsen S P, Overgaard S, Søballe K, Sørensen H T, Lucht U. Registration in the Danish Hip Arthroplasty Registry. Completeness of total hip arthroplasties and positive predictive value of registered diagnosis and postoperative complications. Acta Orthop Scand 2004; 75: 434–41
- Peterson M G, Hollenberg J P, Szatrowski T P, Johanson N A, Mancuso C A, Charlson M E. Geographic variations in the rates of elective total hip and knee arthroplasties among Medicare beneficiaries in the United States. J Bone Joint Surg (Am) 1992; 74(10)1530–9
- Puolakka T J, Pajamaki K J, Halonen P J, Pulkkinen P O, Paavolainen P, Nevalainen J K. The Finnish Arthroplasty Register: report of the hip register. Acta Orthop Scand 2001; 72(5)433–41
- Silman A J. The changing face of rheumatoid arthritis. Arthritis Rheumatism 2002; 46(3)579–81
- Söderman P. On the validity of the results from the Swedish National Total Hip Arthroplasty register. Acta Orthop Scand 2000; 71: 1–33, (Suppl 296)
- Söderman P, Malchau H, Herberts P, Zugner R, Regner H, Garellick G. Outcome after total hip arthroplasty: Part II. Disease-specific follow- up and the Swedish National Total Hip Arthroplasty Register. Acta Orthop Scand 2001; 72(2)113–9
- Symmons D, Turner G, Webb R, Asten P, Barrett E, Luntet M, et al. The prevalence of rheumatoid arthritis in the United Kingdom: new estimates for a new century. Rheumatology 2002; 41(7)793–800, (All authors!)
- The European (18 age groups) Standard Population within SEER*Stat. Available from: URL: (http://www-dep.iarc.fr/dattaava/ewstdpop.htm). Retrieved September 10, 2003
- The StatBank Denmark. Available from: URL: (http://statis-tikbanken.dk/). Retrieved July 24, 2003
- The waiting time for THA. Available from: URL: ( www.venteinfo.dk/ventelister/visventetider.asp)Retrieved September 15, 2003
- Wells V M, Hearn T C, McCaul K A, Anderton S M, Wigg A E, Graves S E. Changing incidence of primary total hip arthroplasty and total knee arthroplasty for primary osteoarthritis. J Arthroplasty 2002; 17(3)267–73