Abstract
Background The time for femoral lengthening is shortened if external fixation is combined with intramedullary nailing. However, several complications have been reported with this procedure.
Patients and methods We retrospectively reviewed the outcome of femoral lengthening performed over an intramedullary nail using external fixation in 22 patients. These patients were followed for a mean of 3.2 (2-5.2) years. The mean age was 22 (13-35) years at the time of the index procedure. The mean lengthening was 5 (2.7-8.1) cm and the external fixator was removed after median 20 (8-30) weeks. The mean external fixation index was 24 (11-35) days/cm and the mean consolidation index was 43 (26-55) days/cm of lengthening.
Results 3 patients who had a past history of infection or open trauma developed osteomyelitis which required removal of the nail. There were 4 knee joint complications when the lengthening was over 20%, including posterior knee subluxation and patella subluxation. In 1 patient, the lengthened segment collapsed with breakage of locking screws.
Interpretation Although lengthening over a nail can reduce the duration of external fixation, caution is required to prevent major complications.
Femoral lengthening is a complex procedure requiring long treatment. Traditionally, external circular fixators allow complex and extended bone lengthening, but the technique is difficult and is often poorly tolerated by the patient (Aldegheri et al. Citation1989, Aaron and Eilert Citation1996). Femoral lengthening over an intramedullary nail is described as an alternative method. The nail allows the external fixator to be removed after the distraction phase, and stabilization during the longer consolidation period is achieved by the nail alone (Paley et al. Citation1997, Gordon et al. Citation2002). The decreased duration of external fixation improves knee motion, makes rehabilitation easier, and prevents deformity and refracture after removal of the fixator. Nevertheless, there are several important complications associated with this technique, which have not been well described. We report our experience of femoral lengthening over an intramedullary nail for the treatment of limb-length discrepancy in 22 patients.
Patients and methods
We reviewed 22 patients retrospectively, all of whom had been treated with femoral lengthening over an intramedullary nail. This had been done at two institutions between January 1996 and December 2001. Mean age at the index procedure was 22 (13-35) years. Indications for surgery included a limb-length discrepancy greater than 2.5 cm which was located in the femur and which caused gait problems. The diagnoses included an epiphyseal injury of the distal femur in 6 patients, an infected diaphyseal fracture in 4, bone loss with open fracture in 4, sequelae of Perthes′ disease in 3, an osteomyelitis of the distal femur in 2, a treated osteosarcoma of the distal femur in 2 patients, and a chil-dren′s femoral fracture in 1. All patients except for the 3 with Perthe′s disease had undergone previous surgery. All of the femora were lengthened over an unreamed femoral nail (20 cases) or unreamed tibial nail (2 cases) (Synthes, Switzerland) that was inserted in an antegrade fashion. The osteotomy site was distracted with a Dyna extor-lengthener (BK Meditech, Korea). Patients who had other procedures on the ipsilateral femur or tibia were excluded from the study.
All patients were available for a follow-up study of mean 3 (2-5) years postoperatively. Hip and knee motion was measured, and pre- and postoperative radiographs were reviewed to assess limb length at the time of final follow-up. A standing anteroposterior radiograph of both lower extremities was obtained to measure limb alignment, including deviation of the mechanical axis and the lateral distal femoral angle.
Operative technique
Preoperative radiographs were reviewed, and the diameter of the femoral canal at the isthmus and the length of the femur were measured. The diameter of the nail was planned to be 2 mm less than the isthmic femoral diameter. The patient was placed laterally on a radiolucent operating table. Before nailing, the distal aspect of the femur was vented to reduce the risk of fat embolism. The standard approach to the pyriformis fossa was used for ante-grade nailing. The entrance of the femoral canal was reamed to accommodate the proximal flare of the nail, but the medulla of diaphysis was not reamed. The level of the osteotomy was about 1 cm distal to the second proximal locking screw. A percutaneous osteotomy was done with multiple drill holes and osteotome. The nail was then inserted and locked proximally. With the nail in place, an external fixator was applied for lengthening. All external fixation pins were inserted without coming into contact with the intramedullary nail; there should be approximately 2 mm or more of space between the external fixation pin and the nail. 2 or 3 pins were fixed on the proximal and distal sides. Pins were inserted either anterior or posterior to the nail.
Postoperative management
On the second postoperative day, patients were allowed toe-touch weight bearing with 2 crutches. As soon as the patients could tolerate the pain, they were weaned from crutches and full weight bearing was recommended. Distraction began on the seventh to tenth postoperative day, with 0.25 mm of distraction accomplished every 6 hours. Anteroposterior and lateral radiographs were taken weekly throughout the distraction period to evaluate callus formation. At 3-4 weeks after planned lengthening had been achieved, the patient was returned to the operating room, the intramedullary nail was interlocked distally with two interlocking screws placed, and the external fixator was removed. Weight bearing was continued, but now with the use of crutches and without immobilization or bracing. Radiographs were taken every 4 weeks until consolidation and final reconstitution of the cortex were complete.
Chi-square test with SPSS version 10.0 (SPSS Inc., Chicago, IL) was used for analysis of clinical results and complications.
Results (table)
Radiographic results
The femora were lengthened a mean of 5.0 (2.7- 8.1) cm or 15% (9-25) of the preoperative femoral length. The mean duration of external fixation was 20 (8-30) weeks, and the mean external fixation index was 24 (11-35) days/cm of lengthening. The mean consolidation index (number of days until 3 cortices were seen on the radiographs) was 43 (26-55) days/cm. 19 patients reached the desired length. 3 patients underwent early removal of the intramedullary nail because of deep infection: 1 had a vascularized fibular graft on the infected segment (), and 2 needed iliac bone graft for poor bone formation in the distracted area. Except for these 3 failed cases, there was no nonunion or malunion at the osteotomy site, and consolidation and reconstitution of the cortex were complete on the latest radiographs. Angular deformity or fracture did not occur during lengthening and before
Figure 1 (case 17). The patient underwent of femoral lengthening over an intramedullary nail. 2 months after the operation, the quality of the callus was poor. At 3 months, a purulent infection occurred from the pin site and distracted area. Antibiotic cement beads were inserted. A vascularized fibular graft was then inserted and the infection and the bone defect healed.

Details of the 22 patients who underwent femoral lengthening over a nail the most recent follow-up. 1 patient experienced a slight 5 mm collapse of the lengthened segment when the locking screws broke (), probably due to early weight bearing and a weak lengthened segment after the removal of the external fixator. No patient showed evidence of avascular necrosis of the femoral head on the radiographs. 2 patients had delayed consolidation of the lengthened segment, which needed a relatively longer duration of external fixation. On the long-leg axis anterior-pos-terior radiographs, the mean lateral femoral distal femoral angle increased from 84 (72-87) degrees preoperatively to 87 (80-89) degrees at the time of the latest follow-up.
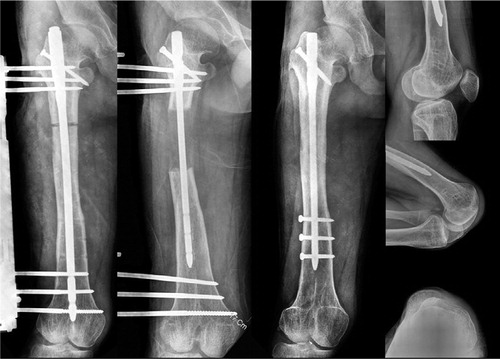
Figure 2 (case 12). Lengthening over a nail was done in an 18-year-old man. After gaining 5 cm, the external fixator was removed. 5 months after the operation, the distracted segment was slightly collapsed, with breakage of locking screws.

Details of the 22 patients who underwent femoral lengthening over a nail
Clinical results
According to the criteria of Paley et al. (Citation1997), there were 10 excellent results, 8 good, 3 fair results, and 1 poor overall result. The range of motion of the hip and knee was evaluated both preoperatively and on a regular basis postoperatively. 7 patients had less than 90° of knee fiexion just after completion of lengthening and the removal of external fixator. 4 patients required quadricepsplasty and 2 patients improved after brisement at the time of external fixator removal. All patients had regained both hip and knee motion to within 5° of the preoperative values, except for 1 patient who had posterior knee subluxation. There was no neurological or vascular complication.
Complications
There were 8 cases of major complications (Aaron and Eilert Citation1996) (3 osteomyelitis, 3 patella subluxation, 1 knee subluxation, and 1 collapse of segment).
Infection. 20 patients experienced superficial pin-track infection which required oral antibiotics. In 7 patients, a deep pin-track infection developed. 4 of them improved after intravenous antibiotics, while 3 patients progressed to osteomyelitis. All of these 3 patients had a previous history of osteomyelitis before the index procedure. 1 patient had deep infection with pus discharge at the time of completion of the lengthening period. After drainage of pus and removal of the intramedullary nail, the distracted callus was almost invisible and a vascularized fibular graft was inserted and union was achieved. The other 2 patients had deep infection in the middle of the lengthening period, and the infection subsided after removal of the intramedullary nail. The planned lengthening was not achieved in these 2 patients, and the distracted callus was poor. An iliac bone graft was used to create stability and union in both patients. The risk group for infection included a shortened femur that was caused by the osteomyelitis (4 cases), a grade-III open fracture that was treated several times with debridement (4 cases), and septic osteomyelitis (2 cases). This risk group showed a higher incidence of deep infection (3 of 10) than the non-risk group (0/12) (p = 0.05).
Knee problems. All patients showed limited knee motion when the external fixator was removed, despite physical therapy. 7 patients had persisting knee motion less than 70°. 2 of them improved after brisement. In the other 4 patients, quadricepsplasty improved motion. 1 patient, who had a deficiency of anterior and posterior ligaments after reinsertion of an irradiated distal femoral segment for treatment of osteosarcoma, showed severe posterior knee subluxation. An arthroplasty was performed in this patient (). 3 patients showed lateral subluxation of the patella, evident in knee fiexion (). At the final follow-up, a complicated knee was defined as the patient having unimproved limitation of motion or residual anatomical deformity of the knee joint. 2 of 3 complicated knees belonged to the longer lengthening group (over 20%, 5 patients), excluding the patient with posterior subluxation. Only 1 complicated knee occurred in the shorter percentile group (under 20%, 16 patients) (p = 0.06, Chi square test). Among 7 cases of stiff knees (under 70 degrees of fiexion) at the time of external fixator removal, 5 were in the group with lengthening of greater than 5 cm and 2 were in the group with lengthening of less than 5 cm, but this was not statistically significant (p = 0.3). Age (≥ 20 years) was not found to be important for the clinical result and complications.
Figure 3 (case 19). The patient experienced femoral shortening after the limb salvage operation, which involved irradiation of the osteosarcoma of the distal femur. Lengthening over a nail was done, and 7.7 cm was gained. Although satisfactory lengthening was achieved, severe knee subluxation occurred with stiffness which was probably due to deficiency of cruciate ligaments. Arthroplasty was performed in this patient.

Figure 4 (case 22). The 16-year-old male patient underwent the procedure of femoral lengthening over an intramedullary nail. A satisfactory lengthening of 6.5 cm was achieved. However, lateral subluxation of the patella occurred in knee fiexion.
Discussion
Traditional femoral lengthening using external fixation has drawbacks because of the long treatment time and frequent complications (Garcia-Cimbrelo et al. Citation1992, Luke et al. Citation1992, Bowen et al. Citation1993, Herzenberg et al. Citation1994, Danziger et al. Citation1995). The technique of femoral lengthening over an intramedullary nail has many advantages because it neutralizes the forces on the femur during lengthening (Lin et al. Citation1996, Paley et al. Citation1997, Simpson et al. Citation1999, Gordon et al. Citation2002). Also, the reduced time needed for external fixation and fracture protection of the distracted bone is remarkable. It also allows most patients to resume normal hip and knee motion. In our study, the external fixation index was less than 1 month, which is much shorter than the conventional Ilizarov method (Aaron and Eilert Citation1996). It was, however, longer than other reports of the same method (Gordon et al. Citation2002, Paley et al. Citation1997), because of 2 patients who experienced delayed consolidation. Another reason for the longer duration of external fixation in our study is that the removal of the external fixator was delayed because we had to wait for the distracted callus to mature, especially after experiencing the collapse of the distracted segment and broken screws in the early part of our study. Kristiansen and Steen (Citation1999) also reported the same complication in tibial lengthening. We believe this complication may be a result of the smaller size of the locking screws in the unreamed nail. We thus recommend that removal of the external fixator be delayed until adequate maturation of callus; it should not be removed immediately after the lengthening.
Pin-track infections are inevitable when using an external fixator (Garcia-Cimbrelo et al. Citation1992), and can be a source of deep infection spreading to the intramedullary nail. Kristiansen and Steen have reported that in tibial lengthening with a similar technique, deep intramedullary infection occurred in 1/9 patients (Kristiansen and Steen Citation1999). Gordon et al. (Citation2002) reported 2 cases of osteomyelitis in 9 patients, 1 of whom had had multifocal osteomyelitis as an infant. We had 3 cases of osteomyelitis, all of which had a previous history of infection or open fracture. However, it is still unknown whether the nailing increases the risk of infection. We believe that previous infection should be an important consideration when choosing the method of lengthening. Osteomyelitis is the most serious potential complication with this technique, whereas it is uncommon with the Ilizarov technique.
A stiff knee, especially fiexion contracture, after femoral lengthening is common and may result from muscle contracture or adhesions during the course of lengthening (Hosalkar et al. Citation2003). Muscle injury by the Ilizarov wire may result in multiple adhesions and excessive stiffness (Bowen et al. Citation1993). In this respect, lengthening over an intramedullary nail has an advantage in maintaining a good knee motion, because of the shorter duration of lengthening and the use of Schanz pins. We had 7 cases of substantial stiffness, however, which needed operative management or had residual deformity.
The modern Ilizarov technique permits extensive lengthening (Murray et al. Citation1993, Stanitski et al. Citation1995). However, lengthening by over 20% has been associated with a high rate of complications such as knee cartilage damage (Stanitski et al. Citation1994). In our study, knee complications increased with lengthening over 20%. Among them, a posterior displacement of the tibia on the femur, which is known to occur as a result of intraarticular bony deficiencies (Jones and Moseley Citation1985), occurred in our case of cruciate ligament deficiency after treatment of osteosarcoma. Although the association is unclear, all 3 cases of patella subluxation in knee fiexion had had distal femoral epiphyseal injury. We consider that hypoplasia or dysplasia of femur may contribute to this complication in addition to the greater degree of lengthening.
In conclusion, lengthening over an intramedullary nail for the treatment of limb-length discrepancy due to femoral shortening is an effective procedure which decreases the duration of treatment with the fixator. However, the technique is at risk from complications, the most important being infection and knee stiffness.
Related Research Data
- Aaron A. D., Eilert R. E. Results of the Wagner and Ilizarov methods of limblengthening. J Bone Joint Surg (Am) 1996; 78: 20–9
- Aldegheri R., Renzi-Brivio L., Agostini S. The callotasis method of limb lengthening. Clin Orthop 1989; (241): 137–45
- Bowen J. R., Levy E. J., Donohue M. Comparison of knee motion and callus formation in femoral lengthening with the Wagner or monolateral-ring device. J Pediatr Orthop 1993; 13: 467–72
- Danziger M. B., Kumar A., DeWeese J. Fractures after femoral lengthening using the Ilizarov method. J Pediatr Orthop 1995; 15: 220–3
- García-Cimbrelo E., Olsen B., Ruiz-Yagüe M., FernandezBaílllo N., Munuera-Martínez L. Ilizarov technique: results and difficulties. Clin Orthop 1992; (283): 116–23
- Gordon J. E., Goldfarb C. A., Luhmann S. J., Lyons D., Schoenecker P. L. Femoral lengthening over a humeral intramedullary nail in preadolescent children. J Bone Joint Surg (Am) 2002; 84: 930–7
- Herzenberg J. E., Scheufele P. T., Paley D., Bechtel R., Tepper S. Knee range of motion in isolated femoral lengthening. Clin Orthop 1994; (301): 49–54
- Hosalkar H. S., Jones S., Chowdhury M., Hartley J., Hill R. A. Quadricepsplasty for knee stiffness after femoral lengthening in congenital short femur. J Bone Joint Surg (Br) 2003; 85: 261–4
- Jones D. C., Moseley C. F. Subluxation of the knee as a complication of femoral lengthening by the Wagner technique. J Bone Joint Surg (Br) 1985; 67: 33–5
- Kristiansen L. P., Steen H. Lengthening of the tibia over an intramedullary nail, using the Ilizarov external fixator. Major complications and slow consolidation in 9 lengthenings. Acta Orthop Scand 1999; 70: 271–4
- Lin C. C., Huang S. C., Liu T. K., Chapman M. W. Limb lengthening over an intramedullary nail: an animal study and clinical report. Clin Orthop 1996; (330): 208–16
- Luke D. L., Schoenecker P. L., Blair V P, 3rd, Capelli A. M. Fractures after Wagner limb lengthening. J Pediatr Orthop 1992; 12: 20–4
- Murray D. W., Kambouroglou G., Kenwright J. One-stage lengthening for femoral shortening with associated deformity. J Bone Joint Surg (Br) 1993; 75: 566–71
- Paley D., Herzenberg J. E., Paremain G., Bhave A. Femoral lengthening over an intramedullary nail. A matched-case comparison with Ilizarov femoral lengthening. J Bone Joint Surg (Am) 1997; 79: 1464–80
- Simpson A. H. R. W., Cole A. S., Kenwright J. Leg lengthening over an intramedullary nail. J Bone Joint Surg (Br) 1999; 81: 1041–5
- Stanitski D. F., Rossman K., Torosian M. The effect of limb lengthening of articular cartilage. An experimental study. Clin Orthop 1994; (301): 68–72
- Stanitski D. F., Bullard M., Armstrong P., Stanitski C. L. Results of femoral lengthening using the Ilizarov technique. J Pediatr Orthop 1995; 15: 224–31