
Abstract
Conclusion: Airtraq® laryngoscope can obviously improve laryngeal visualization and may provide a useful solution to treatment of patients with difficult laryngeal exposure (DLE) under a conventional suspension laryngoscope in phonomicrosurgery.
Objective: In phonomicrosurgery, otolaryngologists may inevitably encounter DLE. Attempts to improve laryngeal exposure have yielded important advances, but the prevalence of DLE yet remains persistent. To overcome this problem, this study applied the Airtraq® laryngoscope to perform phonomicrosurgery combined with a video system. The aim of this study is, thus, to explore the clinical usefulness of the Airtraq® laryngoscope in patients with DLE.
Methods: One hundred and fifty-eight cases who underwent phonomicrosurgery for benign lesions of vocal cord at this hospital were enrolled in this study, of which nine patients were confirmed to be DLE under direct suspension laryngoscope. These nine patients were treated by Airtraq® laryngoscope together with a video system.
Results: In comparison with the traditional suspension laryngoscope, exposure of larynx was remarkably improved by Airtraq® laryngoscope. Under the excellent laryngeal visualization provided by Airtraq®, phonomicrosurgery was successfully accomplished for vocal fold lesions without any severe complications in all cases with DLE.
Introduction
Endolaryngeal microsurgery using a suspension laryngoscope is a routine and well-established procedure to treat vocal cord lesions that cause dysphonia. Optimal laryngeal exposure is essential in phonomicrosurgery. Suspension laryngoscopy relies on the achievement of a direct ‘line-of-sight’ for adequate exposure of the glottis by alignment of the oral, pharyngeal, and laryngeal axes [Citation1]. Laryngeal exposure is not problematic in most cases; however, in some patients difficult laryngeal exposure (DLE) is encountered, which may result in unnecessary trauma, incomplete surgery, and even abortion of the operation [Citation2]. To solve this problem, several methods and alternative techniques, such as head elevation [Citation3], external counter pressure to the larynx, flexible fibre-scope [Citation4,Citation5], curved laryngoscope [Citation6–8], and video-assisted rigid endoscope [Citation9,Citation10] have been developed. These methods and techniques may resolve the problem of DLE to a certain extent. However, DLE is inevitably encountered in phonomicrosurgery, especially in patients with short neck, retrognathia, cervical spine rigidity, and marked obesity [Citation11]. As a consequence, a new solution to DLE in phonomicrosurgery is highly demanded.
The Airtraq® (Prodol Meditec S.A., Vizcaya, Spain) laryngoscope is one of the most popular devices facilitating tracheal intubation [Citation12,Citation13]. This laryngoscope has an anatomically shaped blade, which enables a clear visualization of the glottis without alignment of the oral, pharyngeal, and laryngeal axes [Citation14]. Early studies have shown that Airtraq® could provide an improved and excellent view of the glottis and has been used in the management of difficult airways in anesthesiology [Citation12–15]. Inspired by this, it encourages us to use Airtraq® in phonomicrosurgery for DLE patients. Therefore, the aim of this study is to explore the possibility of using the clinical role of the Airtraq® laryngoscope to resolve DLE in phonomicrosurgery. In this study, using an Airtraq® laryngoscope in combination with a video system, we successfully perform phonomicrosurgery in nine patients with DLE. We here describe the surgical procedures and show its clinical usefulness in patients with DLE.
Materials and methods
Subjects
This study was approved by the ethics committee at Peking University Third Hospital. All patients anticipated to have problems with laryngeal exposure were given detailed information about this technique, and pre-operative informed consent was obtained. One hundred and fifty-eight patients with benign lesions of vocal cord undergoing endolaryngeal microsurgery at the department of otolaryngology, Peking University Third Hospital between February 2015 and July 2016 were enrolled in this study. Among these patients, nine cases (5.7%) was identified as DLE under suspension laryngoscope. There were seven males and two females, ranging in age from 34–65 years. The diagnoses included polyp in five patients, Reinke’s edema in two patients, and cyst nodules in one patient each. The clinical features of all these patients and the possible causes of DLE are shown in .
Table 1. Clinical features of patients, possible causes of difficult laryngeal exposure (DLE), and grade of laryngeal exposure.
Equipment
Airtraq® laryngoscope (Airtraq® AVANT, AC-061, Prodol Meditec S.A., Spain) was used for the phonomicrosurgery (). It has an anatomically shaped blade and contains an optical system with high resolution. To perform the surgery, we designed a series of instruments with curvature similar to the anterior part of the Airtraq® laryngoscope (). In operation, Airtraq® was connected with an endoscopic video system and, thus, the images of the larynx were displayed on a monitor (). The endoscopic video system was made with a color video camera system (Telecam Model 22200020-104, Karl Storz, GmbH & Co., Tuttlingen, Germany) and a LCD monitor (LMD-2140MD, Sony, Tokyo, Japan).
Figure 1. Airtraq® laryngoscope has an anatomically shaped blade and can be connected with a video camera system (A). A set of curved instruments designed by our team (B). In operation, Airtraq® was connected with an endoscopic video system and, thus, the images of the larynx were displayed on a monitor. The surgeon held Airtraq® with the left hand and the instrument with the right hand (C).

Surgical procedure
Patients were administered general anesthesia with endotracheal intubation (5.5–6.0 mm in diameter) and muscle relaxation for endolaryngeal surgery. Then, the direct suspension laryngoscope was placed transorally and an attempt was made to expose the larynx as much as possible. If the larynx, including the lesion, could not be adequately visualized, head elevation, external counter pressure to the larynx, and a video-assisted angled endoscope were applied to improve laryngeal exposure.
If laryngeal exposure was still insufficient by these procedures, Airtraq® laryngoscope combined with an endoscopic video system was used. When connected to an endoscopic video system, the real-time magnified images of the entire glottis and the lesion were obtained. During the procedure, the patients were in a natural supine position with head in a neutral posture. The main surgeon held Airtraq® in the left hand and placed it into the mouth in the midline. The laryngoscope was then glided along the ventral surface of the tongue and advanced down towards the base of the tongue and posterior pharyngeal wall slowly until the epiglottis came into view. After that, the tip of the blade was placed in the vallecula or the laryngeal surface of the epiglottis. Lifting the epiglottis by elevating the blade slightly could optimize the exposure of the glottis. Under optimal exposure and the guidance of the endoscopic video system, the lesion was removed with our specially designed curved instruments, as mentioned above. Usually, the main surgeon performed the surgery with one hand to hold Airtraq® and the other hand to hold the instrument (). If necessary, an assistant held the laryngoscope and, thus, the main surgeon can perform the surgery bimanually.
Evaluation of laryngeal exposure
The laryngeal exposure under suspension laryngoscope and Airtraq® were classified according to a modified Cormack-Lehane score as follows: grade 1, full view of the vocal cords; grade 2A, partial view of the vocal cords; but the anterior commissure was not seen; grade 2B, partial view of the vocal cords (less than half); grade 3, only the arytenoids visible; and grade 4, the entire glottis and arytenoids hidden [Citation7].
Results
shows demographic data of the nine DLE patients. In one patient, the entire larynx was not visualized (grade 4), in six patients, only arytenoid area was exposed (grade 3) and in two patients less than half of the vocal folds was seen (grade 2B) by the direct suspension laryngoscope (). When applying Airtraq® laryngoscope, excellent view of the glottis was easily obtained in all cases (grade 1), as typically shown in . Compared with the direct suspension laryngoscope, the Cormack-Lehane scale exhibited striking improvement, as shown in . The possible causes of DLE included short neck, cervical spinal rigidity, obesity, retrognathia and buckteeth. The vocal cord lesions were successfully removed in all patients for the therapeutic purposes under the Airtraq® laryngoscope and the video system. There were no post-operative complications related to the tongue, teeth, or laceration of the lateral tonsillar pillar. Only one patient complained of post-operative slight throat pain because of abrasion of the mucosa in the soft palate.
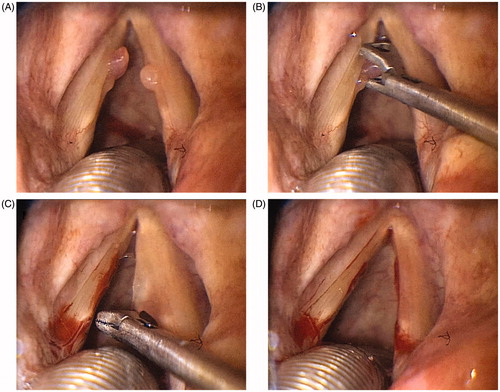
A representative case (case No.5 in ) is described below. A 62-year-old man presented with hoarseness of 7 months was admitted to our department. Fiber-optic laryngoscopy revealed bilateral vocal cords polyps. The exposure of the larynx was impossible through a direct suspension laryngoscope at surgery due to short neck, cervical spinal rigidity, and obesity. In spite of considerable external counter pressure to the larynx, modification of patient posture and an angled rigid endoscope being applied, only the arytenoid area was visible (). When applying the Airtraq® laryngoscope, the whole vocal cord was exposed, including the anterior commissure (). The vocal cord lesions were removed successfully with curved forceps, while the surgeon observed images on the monitor ().
Figure 2. Laryngeal exposure with the conventional suspension laryngoscope (Case No. 5 in ). With the conventional suspension laryngoscope, only the arytenoid area could be viewed microscopically, as grade 3 laryngeal exposure.
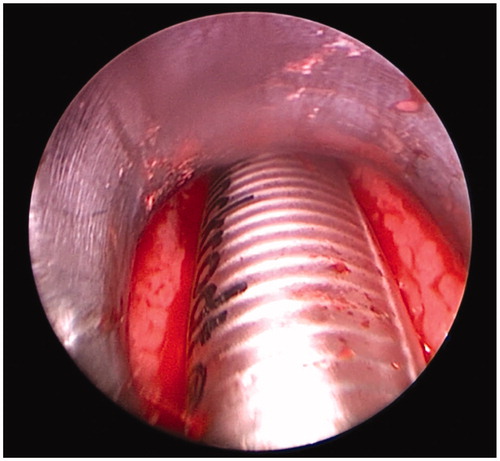
Figure 3. Laryngeal exposure with Airtraq® laryngoscope (Case No. 5 in ). When applying the Airtraq® laryngoscope, the entire glottis was exposed including the anterior commissure, as grade 1 laryngeal exposure. The bilateral polys were also visualized clearly (A). The left vocal cord polyp was grasped with the special curved cutting forceps (B). The right vocal cord polyp was removed successfully by the same method (C). The vocal cord polyps were just removed completely (D).
Discussion
Difficult laryngeal exposure (DLE) is defined as a clinical situation in which a trained otolaryngologist experiences difficulties in exposing the larynx in phonomicrosurgery using a suspension laryngoscope. Although it is successful in most cases, the exposure of the larynx in a certain number of patients yet remains difficult [Citation4–8]. Failure to expose the larynx adequately is the leading cause of operation abortion [Citation2]. Although there is no exact statistical data for the incidence of DLE, the frequency of DLE seems to be increasing recently because of a growing rate of obesity and older patients with rigid cervical spines [Citation5,Citation16].
Attempts to improve the laryngeal exposure in patients with DLE have yielded several important advances, but the prevalence of insufficient views of the glottis is persistent [Citation17]. Since the natural anatomy of the oral cavity and the pharynx is evidently curved, a laryngoscope used in phonomicrosurgery reflecting this anatomy should be accordingly curved. Curved laryngoscopes, including rigid curved laryngoscope or GlideScope® videolaryngoscope, were previously reported to provide good visualization for DLE patients, but they all had some limitations [Citation6–8]. The common limitations included low image resolution and magnification, narrow working space, and difficulty in using the CO2 laser systems. Therefore, effective alternative techniques are essentially needed in such a crucial situation.
Airtraq® is one of the curved laryngoscopes which is designed for tracheal intubation. Early studies have demonstrated that the main impact of Airtraq® is its capability of clearly visualize the laryngeal structures [Citation12–15]. Moreover, Airtraq® has a high-resolution optical system that can be connected with an endoscopic video system [Citation14]. Inspired by these advantages, we believe that Airtraq® may provide an effective solution for DLE in phonomicrosurgery. As described above, among 158 cases who underwent phonomicrosurgery at our hospital during a 17-month period, it was difficult to expose the larynx with a direct suspension laryngoscope in nine cases (∼ 5.7%). For all of our cases with DLE, by using Airtraq®, together with a video system, we achieved optimal laryngeal view including the region of the anterior commissure in neutral or slight flexed position and without external counter pressure to the larynx. Our results demonstrated that, in comparison with the traditional suspension laryngoscope, Airtraq® exhibited improved laryngeal view in all cases with DLE. More important, under the excellent laryngeal exposure, the vocal cord lesions were successfully removed using the described surgical method described above. The Airtraq® laryngoscope also appeared to produce less complications than the traditional suspension laryngoscope. Hypoesthesia and immobility of tongue, loss of taste, injury to the upper teeth and laceration of the lateral tonsillar pillar, which usually occurred in phonomicrosurgery using a suspension laryngoscope [Citation18], were not observed. This could be explained by the fact that an anatomically shaped blade of Airtraq® essentially enables easier and better access to the glottis and laryngeal lesions and allows an atraumatic placement in virtually all anatomical configurations with remarkably reduced forces exerted on the tongue, upper teeth, and oropharyngeal soft tissue [Citation12,Citation19]. Another outstanding advantage is that Airtraq®, in combination with a high-resolution camera and video monitor, can provide very fine and magnified images of the larynx and, thus, enables a precise monitor-guided operation.
Of course, there are still some limitations, such as the requirement of a specially designed set of instruments that have the same curvature as Airtraq®. Another limitation, which is also inherent in other curved laryngoscopes, the curved working pathway of Airtraq® make it difficult for a surgeon to use CO2 laser systems during the surgery. Moreover, techniques requiring fine manipulation, such as the microflap technique which can be performed in a traditional straight laryngoscope, are difficult to perform in such a curved laryngoscope. However, with the development of specifically designed instruments for Airtraq®-guided surgery, it may be possible to perform these precise procedures in the Airtraq® laryngoscope. In the future, more sophisticatedly curved instruments and proper contact type laser systems are necessary for Airtraq®-guided phonomicrosurgery.
Nonetheless, the most important finding of our study is that the Airtraq® laryngoscope improved laryngeal exposure and allowed phonosurgeons to successfully remove laryngeal lesions without severe complications in patients who presented with poor laryngeal view using a conventional suspension laryngoscope. We believe that the use of the Airtraq® laryngoscope might provide a new and effective solution to DLE in phonomicrosurgery.
Conclusions
Difficult laryngeal exposure in phonomicrosurgery is an inevitable clinical problem which is not fully resolved yet. In such patients, we performed endolaryngeal microsurgery successfully with the Airtraq® laryngoscope in combination with a video system. The Airtraq® laryngoscope demonstrated here can obviously improve the exposure of the larynx and may provide a useful option to treat the laryngeal lesions in patients with DLE under a conventional suspension laryngoscope.
Disclosure statement
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Gugatschka M, Gerstenberger C, Friedrich G. Analysis of forces applied during microlaryngoscopy: a descriptive study. Eur Arch Otorhinolaryngol 2008;265:1083–7.
- Fang R, Chen H, Sun J. Analysis of pressure applied during microlaryngoscopy. Eur Arch Otorhinolaryngol 2012;269:1471–6.
- EI-Orbany MI, Getachew YB, Joseph NJ, Salem MR, Friedman M. Head elevation improves laryngeal exposure with direct laryngoscopy. J Clin Anesth 2015;27:153–8.
- Ohno S, Hirano S, Tateya I, Kojima T, Ito J. Management of vocal fold lesions in difficult laryngeal exposure patients in phonomicrosurgery. Auris Nasus Larynx 2011;38:373–80.
- Kikkawa YS, Tsunoda K, Niimi S. Prediction and surgical management of difficult laryngoscopy. Laryngoscope 2004;114:776–8.
- Friedrich G, Kiesier K, Gugatschka M. Curved rigid laryngoscope: missing link between direct suspension laryngoscopy and indirect techniques? Eur Arch Otorhinolaryngol 2009;266:1583–8.
- Kim JK, Jeong HS, Kwon HN. A new curved rigid laryngoscope to overcome the difficult laryngeal exposure (DLE) in endolaryngeal surgery. Eur Arch Otorhinolaryngol 2007;254:901–5.
- Xidong C, Xia Z, Chenjie X, Wenhong Y, Huichang Y, Jiaqi J. Management of difficult suspension laryngoscopy using a GlideScope® Video Laryngoscope. Acta Otolaryngol 2012;132:1318–23.
- Kawaida M, Fukuda H, Kohno N. Video-assisted rigid endoscopic laryngosurgery: application to cases with difficult laryngeal exposure. J Voice 2001;15:305–12.
- Kantor E, Berci G, Haniike M. Operating videoscope for microlaryngeal surgery. Surg Endosc 2006;20:S484–S7.
- Piazza C, Mangili S, Bon FD, Paderno A, Grazioli P, Barbieri D, et al. Preoperative clinical predictors of difficult laryngeal exposure for microlaryngoscopy: the Laryngoscore. Laryngoscope 2014;124:2561–7.
- Maharaj CH, Higgins BD, Harte BH, Laffey JG. Evaluation of intubation using the Airtraq laryngoscope by anaesthetists in easy and simulated difficult laryngoscopy-a manikin study. Anaesthesia 2006;6:469–77.
- Giquello J-A, Humbert S, Duc F, Monrigal J-P, Granry J-C. Use of the Airtraq by inexperienced physicians supervised during a series of tracheal intubation in adult patient with anticipated difficult airway. Ann Fr Anesth Reanim 2011;30:804–8.
- Niforopoulou P, Pantazopoulos I, Demestiha T, Koudouna E, Xanthos T. Video-laryngoscopes in the adult airway management: a topical review of the literature. Acta Anaesthesiol Scand 2010;54:1050–61.
- Paolini JB, Donati F, Drolet P. Review article: video-laryngoscopy: another tool for difficult intubation or a new paradigm in airway management? Can J Anaesth 2013;60:184–91.
- Pinar E, Calli C, Oncel S, Selek B, Tatar B. Preoperative clinical prediction of difficult laryngeal exposure in suspension laryngoscopy. Eur Arch Otorhinolaryngol 2009;266:699–703.
- Cheng J, Woo P. Rescue microlaryngoscopy: a protocol for utilization of four techniques in overcoming challenging exposures in microlaryngeal surgery. J Voice 2012;26:590–5.
- Klussmann JP, Knoedgen R, Damm M, Wittekindt C, Eckel HE. Complications of suspension laryngoscopy. Ann Otol Rhinol Laryngol 2002;111:972–6.
- Liu L, Tanigawa K, Kusunoki S, Tamura T, Ota K, Yamaga S. Tracheal intubation of a difficult airway using Airway Scope, Airtraq, and Macintosh laryngoscope: a comparative manikin study of inexperienced personnel. Anesth Analg 2010;110:1049–55.