
Abstract
Background
Recurrent respiratory papillomatosis (RRP) is a wart-like lesion mainly affecting the larynx, caused by human papillomavirus (HPV) genotypes 6 and 11. The disease affects both children and adults, and there is no cure. Surgery is the current symptom-relieving treatment; however, HPV vaccination is used as an adjuvant treatment.
Aims and Objectives
The aims were to study effects of HPV vaccination in RRP cases and to compare juvenile-onset to adult-onset disease and high treatment frequency (TF) to low TF cases.
Material and Methods
Medical records of RRP patients were studied from May 2006 to January 2023. Eighty-five RRP cases, tested for HPV genotypes with PapilloCheck®, were included. Vaccination- onset- and treatment analysis were performed.
Results
Twelve percent of the cases were vaccinated. The number of surgeries decreased from 2.0 to 0.8/year after HPV vaccination. Most cases had an adult-onset and less than one treatment per year. Juvenile-onset cases had a higher vaccination treatment ratio compared to adult-onset.
Conclusions
HPV vaccination was associated with a lower number of treatments per year, supporting the use of vaccination as an adjuvant treatment.
Significance
Vaccination as adjuvant treatment to surgery may lead to increased quality of life for RRP patients and saved healthcare resources.
Chinese Abstract
背景:复发性呼吸道乳头状瘤病(RRP)是一种主要影响喉部的疣样病变, 由人乳头瘤病毒 (HPV) 基因型 6 和 11 引起。该疾病影响儿童和成人, 并且没有治愈方法。 手术是目前缓解症状的治疗方法; 然而, HPV 疫苗接种被用作辅助治疗。
目的:研究 HPV 疫苗接种对 RRP 病例的影响, 并将青少年发病的疾病和成人发病的疾病以及高治疗频率 (TF) 病例和低 治疗频率病例进行比较。
材料和方法:研究了 2006 年 5 月至 2023 年 1 月 RRP 患者的医疗记录。纳入了 85 例 RRP 病例, 并使用 PapilloCheck® 进行了 HPV 基因型检测。 进行了疫苗接种、发病和治疗的分析。
结果:百分之十二的病例接种了疫苗。 手术数量从每年2.0次减少到接种 HPV 疫苗后每年 0.8 次。 大多数病例是成人发病, 每年治疗少于一次。与成人发病相比, 青少年发病病例的疫苗接种治疗率较高。
结论:HPV 疫苗接种与每年治疗次数较少相关, 支持使用疫苗接种作为辅助治疗。
意义:疫苗接种作为手术的辅助治疗可能会提高 RRP 患者的生活质量并节省医疗资源。
Introduction
Recurrent respiratory papillomatosis (RRP) is a wart-like lesion mainly affecting the larynx. It is predominantly caused by human papillomavirus (HPV) genotypes 6 and 11. There is no cure, and the course of the disease is varying. Some patients experience remission, whereas others may develop lesions that require multiple surgical procedures [1]. RRP is characterized by a subtle onset and progressive voice and airway impairment, with a potentially life-threatening outcome [Citation2]. The incidence has been reported to be 0.54 per 100,000 for adult-onset RRP, and 0.17 per 100,000 for juvenile-onset RRP [Citation3]. Once established, the disease is associated with a high burden on patient quality of life [Citation1], as well as large healthcare-related costs. These have been estimated to more than $120 million per year in the US (year 2000) with the annual cost per patient reaching $60,000 [Citation4].
RRP can be classified based on the age of onset, as juvenile-onset (<18 years) or adult-onset (≥ 18 years). Juvenile-onset RRP has been characterized as frequently multi-sited, associated with specific HPV genotypes (HPV 11), and having a higher rate of recurrence than adult-onset RRP [Citation5]. Juvenile-onset RRP is acquired via vertical HPV transmission from mother to child, while adult-onset RRP is typically sexually transmitted [Citation5].
The HPV genotypes can be stratified into low risk (6,11), the most common cause of RRP, or high-risk (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68), based on their carcinogenicity [Citation6]. Studies have shown that HPV 11 is associated with a more treatment-provoking course of RRP [Citation5].
The current symptom-relieving treatment for RRP is surgical removal of the lesion. Several surgical therapies are available, including CO2 laser. The purpose of surgery is complete removal of the lesion and preservation of healthy structures within the larynx. The most common surgical complications after CO2 laser are stenosis in the larynx, vocal fold scarring, and web formation (adhesions) [Citation1].
There are three vaccines available against HPV-related diseases: Cervarix® (GlaxoSmithKline), a bivalent vaccine (HPV 16/18), Gardasil® (Merck Inc.), a quadrivalent vaccine (HPV 16/18 and HPV 6/11), and Gardasil-9® (Merck Inc.), a nine-valent vaccine (HPV 16/18, 6/11, 31/33, 45/52 and 58) [Citation6]. After introducing the vaccinations with Gardasil, HPV-related diseases have decreased [Citation7]. Since 2020, HPV vaccine is offered for free for all children in Sweden [Citation8,Citation9].
It is not known whether HPV vaccination reduces the treatment frequency (TF) in Swedish RRP cases, or if juvenile cases have more severe disease and are infected with specific HPV strains, or finally, if cases with high TF (≥ 1 treatment/year) are associated with specific case factors.
The specific aims were (i) to describe RRP patient characteristics, (ii) to study vaccinated RRP cases with number of treatments per year as an effect outcome, (iii) to compare juvenile-onset to adult-onset RRP and (iv) to compare cases with high treatment frequency (TF) to low TF. If the results show that the use of HPV vaccination as an adjuvant treatment is associated with better outcomes, this can support treatment of cases with high TF in a more accelerated time frame. Possible treatment benefit could reduce the need for surgery, with health-economic gains and increased quality of life for RRP patients.
Material and methods
This cross-sectional and longitudinal study was approved by the Swedish Ethical Review Authority. The approval number and its amendments are 2018-01-29; 2017-543-32 M (2015-323-32 M, 2012-276-32 M, 2010-277-31 M). In connection to diagnostic and therapeutic surgery of the RRP lesion, patients consented to sampling and storage of samples in the BioBankNorr. Reporting here is guided by the STROBE checklist for cross-sectional studies [Citation10].
The RRP participants were referred to the Department of Otorhinolaryngology, University Hospital of Umeå (a tertiary referral hospital) from May 2006 to January 2023. The RRP cases were labelled with the D14.1A diagnosis code using ICD-10, based on histopathology confirming the RRP diagnostic work-up. PapilloCheck® (Greiner BioOneGmbH, Frickenhausen, Germany) was used for HPV detection. PapilloCheck® is a PCR-based microarray system that can detect 24 HPV genotypes. This method requires at least 350 DNA base pairs. The case medical records were checked for inclusion and exclusion criteria, and once included were pseudoanonymized in the analysis database.
Patient characteristics
The study population included 85 cases: 66 men, and 19 women. Most cases had a glottic lesion (online Supplementary Material Table 1). We did not identify any difference regarding age at first disease evaluation or duration of disease when comparing the included cases to the excluded ones (n = 14): mean age 53 years (range: 10–87) for included cases, and 54 years (range: 14–85) for excluded cases. The median duration of disease was 12 years for included cases and 11 years for excluded (flowchart with inclusion and exclusion criteria is presented in online supplementary material Figure 1).
Vaccination analysis
Thirteen cases were vaccinated in addition to surgery. In the selection process for inclusion, only subjects with more than two years since completed vaccination were included as treated (n = 10). Excluded cases (n = 3) were considered not vaccinated in the analysis, due to less than two years since vaccination. The subjects were selected for vaccination based on high treatment frequency (TF ≥ 1/year). A time frame of two years pre- and post-vaccination was compared for the number of treatments per year. A follow-up frame of two years was chosen for two reasons. Firstly, we expect two years to be sufficient to reflect an impact on treatment intervals. Secondly, a two-year time frame allows more cases to be included than a longer time frame, for which there is limited case experience. Thus, the cases became their own controls regarding change in treatment interval pre- compared to post-vaccination. Data is reported at an aggregated level. Some patients received Gardasil® and others Gardasil-9®. We did not stratify for type of HPV vaccine received as long as it was a vaccine that has proven efficacy against the specific HPV genotype. In Sweden, children are offered HPV vaccination in a two-dose procedure and adults in a three-dose procedure.
Onset and treatment frequency analysis
Cases with juvenile-onset were compared to cases with adult-onset with focus on HPV strains and treatment frequency. The treatment ratio was calculated as the number of surgical CO2 laser treatments/number of diseased years. A treatment ratio of ≥1 is labelled as high treatment frequency (TF), and a treatment ratio of <1 is considered as low TF. Cases with high TF were compared to cases with low TF with focus on HPV strains and age. Remission is defined as time (> 1 year) with no surgical treatment.
Statistics
Descriptive statistics were presented regarding patient characteristics. Statistics on HPV genotypes are based on the number of HPV observations and not the number of cases since each case could be infected with more than one genotype.
In the vaccination analysis, due to non-normal distribution of estimates, the results were presented as the median and interquartile range. Wilcoxon signed-rank test was used when comparing differences between treatment ratios pre- and post-vaccination.
In the disease onset and treatment frequency analysis, cross-tabulations presented numbers and percentages for sex, macroscopic web, HPV vaccination, HPV genotype, and disease onset. Associations were analysed using the Chi-square test and Fisher’s exact test. Median and interquartile range values were reported for treatment ratios and duration of disease, and these associations were analysed using the Mann–Whitney U-test. Mean and range values were reported for age and analysed with the t-test. The level for detecting significant differences in group comparisons was p < .05. All statistical analyses were performed using the software package IBM SPSS USA, version 28.
Results
There were 85 total cases of RRP included the analysis cohort: mainly men (78%), with a glottic lesion (78%), infected with HPV 6 (74%) and adult-onset (87%). Most subjects had less than one surgical CO2 laser treatment/year (79%). Four cases were infected with two genotypes each: HPV 73 + 82, HPV 6 + 39, HPV 6 + 11, and HPV 16 + 33 (online Supplementary Material Table 2).
Figure 1. Treatment ratio pre- and post-vaccination.
1Wilcoxons signed rank test
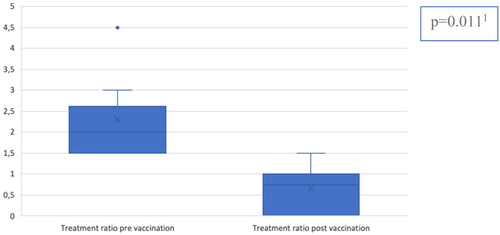
The RRP cases were grouped into those vaccinated or not. Ten cases (12%, 10/85) were vaccinated. We compared the number of treatments per year two years pre-, and post-vaccination. The median treatment ratio in the vaccinated group decreased from two treatments per year pre-vaccination to 0.8 treatments per year post-vaccination (p = .011) ().
We compared juvenile-onset RRP (<18 years) to adult-onset (≥ 18 years), and there were more females with juvenile-onset (p = 0.013) (online Supplementary Material Table 3). Thirty-six percent (4/11) of the juvenile-onset and 8% (6/74) of the adult-onset received the HPV vaccine. The median treatment ratio was higher for juvenile-onset (1.0 treatment/year) than adult-onset (0.4 treatments/year) (p = 0.006). Of the juvenile-onset, 82% (9/11) had HPV 6, 18% (2/11) had HPV 11 and none had a high-risk HPV. Of the adult-onset, 80% (57/71) had HPV 6, 6% (4/71) had HPV 11 and 14% (10/71) had a high-risk HPV. None of the differences are statistically significant.
In the treatment frequency analysis, we compared cases with high TF (≥ 1/year) to those with low TF (<1/year). High TF subjects had a juvenile-onset in 28% (5/18), and an adult-onset in 72% (13/18). Of the low TF cases, fewer (9%, 6/67) had juvenile-onset than adult-onset (91%, 61/67, p = 0.050). Seventeen percent (3/18) of the high TF cases had macroscopic web, in comparison to 3% (2/67) of the low TF cases. Thirty-nine percent (7/18) of those with high TF received the vaccine, as did 5% (3/67) of those with low TF. This shows that vaccination against HPV was predominantly provided to those with high TF. The mean age at entry into the cohort is 45 years for high TF and 55 years for low TF. Seventy percent (14/20) of the high TF cases had HPV 6, 10% (2/20) had HPV 11, and 20% (4/20) had a high-risk HPV. Of the low TF cases, 84% (52/62) had HPV 6, 7% (4/62) had HPV 11 and 10% (6/62) had a high-risk HPV (online Supplementary Material Table 4).
Of the vaccinated cases (n = 10), three experienced remissions for >1 year after the vaccination. Two patients remain in remission at the time of this analysis, at 11 and two years after the vaccination. One patient relapsed after two years and seven months. Seven patients did not experience remission, the median relapse time was nine months after vaccination.
Discussion
Findings from this RRP cohort show that HPV vaccination reduced the ensuing surgical CO2 laser treatment frequency (TF), with new insight that also patients with few treatments gain significant reduction in number of surgeries by HPV vaccination. Patients with juvenile-onset disease are not characterized by a specific HPV type but they have a higher TF than those with adult-onset, findings that support consideration of a more active use of vaccines in subjects with juvenile-onset disease.
In accordance with other reports, this study confirms that most cases had an adult-onset and were infected with HPV 6 [Citation1,Citation3]. However, seven cases lacked virus typing: five cases were not tested for HPV genotype and two cases were tested but HPV genotype could not be detected using PapilloCheck®. This could be due to the subject having an HPV genotype that PapilloCheck® could not detect, due to an insufficient amount of DNA, or fragmentation of DNA to less than 350 base pair products, making it inaccessible to PapilloCheck® analysis.
This study further confirms a previous report on significant decrease in the RRP treatment ratio after HPV vaccination [Citation11]. The novelty of these findings is that the treatment ratio is reduced even at a low treatment index with a median of 2.0/year pre-vaccination to 0.8/year post-vaccination. When calculating the treatment ratio, treatments during ongoing vaccination were excluded from the calculations. Only treatments before and after the completed vaccination were included. It is difficult to isolate the effects of surgical and/or adjuvant treatment from the natural course of the RRP disease since it is associated with spontaneous remission. Still, patients with juvenile-onset disease might benefit more from vaccination since they represent a high treatment frequency group of patients.
The cases in our report with juvenile-onset (<18 years) disease have higher TF than adult-onset cases (≥ 18 years). The mean age at entry into the cohort is ten years younger for high TF-cases compared to low TF-cases. This indicates that high TF is more common in younger cases, as supported by Omland et al. [Citation5].
We identified surgical complications, highlighting the need to reduce the number of surgical treatments. The macroscopic web was more common in cases with high CO2 laser TF (≥ 1/year) than in cases with low TF. Web formation is a complication of CO2 laser surgery. Therefore, it is expected that those with more surgeries have higher risk for web development [Citation1]. The macroscopic web is visible and asymptomatic, while the functional web is symptomatic and affects breathing as well as voice. None of our cases had a functional web.
To achieve as highly radical a resection as possible during surgery, patients are ventilated with high-frequency jet ventilation [Citation12]. This means that air from the patient is dispersed in the room and not enclosed in an endotracheal tube with expired air scavanging. Surgical smoke can be dangerous for operating personnel since HPV DNA can be transferred within airborne droplets [Citation13]. It is unclear whether virus particles dispersed in the plume are infectious.
Latent viruses may remain in the adjacent tissue despite removal of the visible papilloma. RRP is a multigene disease that polarizes immune responses to tolerate HPV 6 and 11 infections, and as such predisposes certain individuals to develop RRP [Citation14]. These aspects might explain the high risk for recurrence and the need for multiple surgeries. According to Rosenberg et al. [Citation15], the successful outcome of adjuvant vaccination in RRP cases can be due to an activation of the immune response. The disease is unpredictable, where some cases may spontaneously recover, and others are afflicted with persistent HPV infections [Citation1]. This is one aspect of current incomplete understanding of RRP.
Methodological considerations and limitations
There are some limitations to the study. It is carried out without previous power calculations on clinical effect measures. We reached 85 included cases. This small cohort means increased risk of type II errors. It can be speculated that there could have been a statistical difference between juvenile- and adult-onset concerning treatment frequency, as the data indicates that there is a difference.
Using other methods for HPV detection, for example the INNO-LiPA® HPV Genotyping Extra assay (Fujirebio, Göteborg, Sweden), we might be able to identify > 30 HPV genotypes and at a lower DNA cost, since it requires less a product size of 150 bp, instead of 350 bp, for successful amplification with PCR.
The definition of remission needs to be highlighted since it might affect the reported outcome measure. It is possible that cases with remission >1 year developed an RRP-lesion within 12 months but did not get a surgical appointment until after 1 year. This dynamic is also reflected in the definition of treatment frequency (TF). A high TF (≥ 1 treatment/year) is reported if cases are diagnosed with RRP within the last year and with one completed surgery, within that year. In a prospective view, these cases might be transferred to low TF if no or few surgeries are needed in the future. However, this is a cross-sectional study, and the data are therefore reported according to the time of cut-off. The term high treatment frequency was used because none of the subjects in northern Sweden had a higher treatment frequency than three/year. Using the definition for aggressive RRP (≥ 4 treatments/year) [Citation5], commonly used in other studies, would therefore result in no included cases.
Another drawback might be a sampling bias effect on statistical balance selection of the population. The use of HPV vaccine as adjuvans in RRP treatment was initiated after 2010, initially with low inclusion rate based on international recommendations of > 4 treatments/year. Out of the 85 cases, 18 was treated with high frequency. Ten cases (12%) were vaccinated, of which two were stratified into a low treatment frequency procedure and as such contributing to a convenience sample effect.
Conclusions
These results confirm earlier findings on HPV vaccine as an adjuvant treatment associated with reduced need for surgery in RRP patients, adding new knowledge that also those with few treatments gain significant reduction in number of surgeries by HPV vaccination. This type of benefit could lead to saved healthcare resources, increased protection for healthcare staff, and increased quality of life for RRP patients.
Supplemental Material
Download MS Word (17.4 KB)Supplemental Material
Download MS Word (17.4 KB)Supplemental Material
Download MS Word (17.2 KB)Supplemental Material
Download MS Word (15.2 KB)Supplemental Material
Download MS Word (76.2 KB)Acknowledgments
We would like to thank PhD Anna Lindam for statistical advice and Professor Michael Haney for text revision.
Disclosure statement
No potential conflict of interest was reported by the author((s).
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request from other investigators adhering to the European Union General Data Protection Regulation (EU) 2016/679 GDPR.
References
- Derkay CS, Bluher AE. Update on recurrent respiratory papillomatosis. Otolaryngol Clin North Am. 2019; Aug52(4):669–679. doi:10.1016/j.otc.2019.03.011.
- Loizou C, Laurell G, Lindquist D, et al. Voice and quality of life in patients with recurrent respiratory papillomatosis in a Northern Sweden cohort. Acta Otolaryngol. 2014;134(4):401–406. Apr doi:10.3109/00016489.2013.867457.
- Omland T, Akre H, Vårdal M, et al. Epidemiological aspects of recurrent respiratory papillomatosis: a population-based study. Laryngoscope. 2012;122(7):1595–1599. Jul doi:10.1002/lary.23327.
- Bishai D, Kashima H, Shah K. The cost of juvenile-onset recurrent respiratory papillomatosis. Arch Otolaryngol Head Neck Surg. 2000; Aug126(8):935–939. doi:10.1001/archotol.126.8.935.
- Omland T, Akre H, Lie KA, et al. Risk factors for aggressive recurrent respiratory papillomatosis in adults and juveniles. pLoS One. 2014;9(11):e113584. doi:10.1371/journal.pone.0113584.
- de Martel C, Plummer M, Vignat J, et al. Worldwide burden of cancer attributable to HPV by site, country and HPV type. Int J Cancer. 2017;141(4):664–670. Aug 15 doi:10.1002/ijc.30716.
- Novakovic D, Cheng ATL, Zurynski Y, et al. A prospective study of the incidence of juvenile-onset recurrent respiratory papillomatosis after implementation of a national HPV vaccination program. J Infect Dis. 2018;217(2):208–212. Jan 4 doi:10.1093/infdis/jix498.
- Wikström A, Elfgren K. [HPV vaccines effective and safe.] Lakartidningen. 2021;118:21061.
- Folkhälsomyndigheten. HPV-vaccinuppföljning Folkhälsomyndigheten 2022 [updated 2022-12-16; cited 2023 01-31]. Available from: https://www.folkhalsomyndigheten.se/smittskydd-beredskap/vaccinationer/nationella-vaccinationsprogram/uppfoljning-av-vaccinationsprogram/hpv-vaccinuppfoljning/.
- von Elm E, Altman DG, Egger M, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495–1499. Dec doi:10.1016/j.ijsu.2014.07.013.
- Young DL, Moore MM, Halstead LA. The use of the quadrivalent human papillomavirus vaccine (gardasil) as adjuvant therapy in the treatment of recurrent respiratory papilloma. J Voice. 2015; Mar29(2):223–229. doi:10.1016/j.jvoice.2014.08.003.
- Helmstaedter V, Tellkamp R, Majdani O, et al. High-frequency jet ventilation for endolaryngotracheal surgery–chart review and procedure analysis from the surgeon’s and the anaesthesiologist’s point of view. Clin Otolaryngol. 2015;40(4):341–348. Aug doi:10.1111/coa.12376.
- Okoshi K, Kobayashi K, Kinoshita K, et al. Health risks associated with exposure to surgical smoke for surgeons and operation room personnel. Surg Today. 2015;45(8):957–965. Aug doi:10.1007/s00595-014-1085-z.
- Holm A, Nagaeva O, Nagaev I, et al. Lymphocyte profile and cytokine mRNA expression in peripheral blood mononuclear cells of patients with recurrent respiratory papillomatosis suggest dysregulated cytokine mRNA response and impaired cytotoxic capacity. Immun Inflamm Dis. 2017;5(4):541–550. Dec doi:10.1002/iid3.188.
- Rosenberg T, Philipsen BB, Mehlum CS, et al. Therapeutic use of the human papillomavirus vaccine on recurrent respiratory papillomatosis: a systematic review and Meta-Analysis. J Infect Dis. 2019;219(7):1016–1025. Mar 15 doi:10.1093/infdis/jiy616.