
Prosper Ménière, one French botanist, historian, physician/surgeon discovered a disease with vertigo, hearing loss and ringing in the ear in 1861 namely Meniere’s disease (MD). However, our understanding of MD has still been at a very basic stage. Although the basic pathology of MD was identified as endolymphatic hydrops by autopsy in the 1930s [Citation1], the cause and mechanism of the endolymphatic hydrops remain unclear, leading to confusion and uncertainty in the treatment of the disease. Due to the lack of targeted and systematic treatment, a considerable number of patients inevitably develop from early to late stage.
Currently, there are no new treatments added to the MD guidelines issued by various countries. That is, patients with early-stage lesions whose hearing is still in the fluctuating phase are treated with symptom control, and in late-stage cases, chemical labyrinthectomy with gentamicin and/or surgical treatment is widely used to eliminate symptoms by blocking abnormal vestibular afferents [Citation2, Citation3].
In the past decades, the main goal of surgical treatment was aimed at controlling vertigo, and traditional vertigo surgeries included endolymphatic sac surgery, vestibular neurectomy, and labyrinthectomy [Citation4]. With the exception of endolymphatic sac surgery, the latter two surgeries destroy completely vestibular function.
In most patients with late-stage MD, vestibular and auditory functions are severely impaired, however, they do not completely lose, and residual function is still very important, especially in view of the fact that some patients may progress from unilateral to bilateral morbidity, and therefore it is important to preserve as much vestibular function as possible in order to maintain the body’s equilibrium. Moreover, the preservation of the vestibular and cochlear end organs provides the basis and opportunity for better treatment that may occur in the future.
More recently, minimally invasive surgical concepts and techniques have been widely used in various types of surgical fields, and the treatment concepts of vertigo surgery have also undergone significant changes. In addition to focusing on vertigo control, more and more attention has been paid to the preservation of vestibular and cochlear residual function, or even the reconstruction of function. For example, in MD, semicircular canal plugging combined with cochlear implantation can effectively control vertigo while restoring hearing and possibly reducing tinnitus [Citation5]. This type of surgery has changed the treatment concept of traditional vertigo surgery and formed the basis and direction of modern vertigo surgery.
The triple semicircular canal surgery (TSCP) in recent years has been confirmed by a large number of clinical practices to have a high rate of vertigo control (basically the same as vestibular neurotomy and labyrinthectomy), in the meantime, a high rate of hearing preservation, a high rate of preservation of otolithic function, and a fast postoperative compensation of balance [Citation6–11] have been reached after TSCP. The use of semicircular canal plugging combined with vestibular plugging in cases with otolithic crisis has also achieved satisfactory results in controlling vertigo and drop attack while preserving certain hearing. For cases with severe-to-profound bilateral hearing loss, cochlear implantation was performed simultaneously with TSCP, which achieved the dual purpose of vertigo control and hearing restoration, and well embodied the requirements of functional reconstruction by minimally invasive surgery [Citation5, Citation12].
Therefore, TSCP can be considered a functional vertigo surgery, and its emergence represents the direction of modern vertigo surgery, i.e. to effectively control vertigo symptoms while minimizing damage to the inner ear and maximizing the preservation of inner ear function. The TSCP has thus become an effective means of meeting the challenges of late-stage MD treatment, and its advanced treatment concepts and outcomes have made it an alternative to the majority of destructive vertigo surgeries.
Focusing on TSCP itself, however, challenges still remain. In order to better realize the advantages of its functional concept, we need to adopt a series of minimally invasive techniques for the operation. For example, when opening the semicircular canals, we choose a position far away from the ampullae, choose a smaller grinding drill and lower rotational speed to open the canals, try to preserve the endosteum of the bony semicircular canals, and minimize the damage to the membranous labyrinth. Improve the plugging material to increase the convenience of operation and shorten the operation time. In order to reduce the pressure impact during the plugging process, the canals should be plugged one by one after the three canals are opened, so that the pressure generated during the plugging can be released through the windows. One of authors in this article has also adopted underwater endoscopic technique in order to achieve a more delicate operation (unpublished data). Secondly, perioperative management should be strengthened. For example, the use of glucocorticoids during the perioperative period may help to improve the anti-stress capacity of the inner ear to cope with surgical trauma, and also help to alleviate the aseptic inflammation of the inner ear induced by plugging [Citation13].
In order to better perform the minimally invasive and function-preserving concept of semicircular canal surgery. There is also a need to continuously improve surgical techniques and apply new interventional materials such as air bags, degradable materials and other new technologies during semicircular canal plugging to achieve temporary or reversible obstruction of the semicircular canals, with a view to restoring semicircular canal function after the disease has been cured. This would be of great benefit to patients with MD.
The surgery can lead to further hearing loss in about 20% of patients, although this loss occurs on the basis of profound deafness and without substantial impact on the patient’s useful hearing, the indications for the surgery need to be strictly adhered to. The indications for surgery are patients with stage III or IV MD who have been treated conservatively for at least more than six months and still have frequent vertigo episodes that are not effectively controlled, with a hearing loss of more than 60 dB on the affected side or a speech recognition rate of less than 50%. At the same time, the contralateral side should have adequate hearing and vestibular function. TSCP combined with cochlear implantation can be performed simultaneously when available to achieve the best therapeutic outcome.
A completed randomized controlled study of TSCP versus gentamicin chemical labyrinthectomy have been performed by us and we confirmed the clear advantages of TSCP in terms of vertigo control and functional preservation (data unpublished), making it the preferred modality of surgical treatment for late-stage MD.
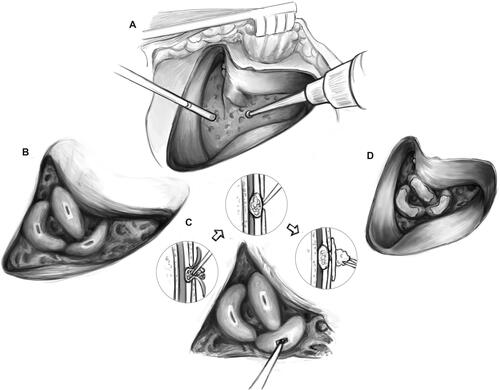
has shown the key point process of the TSCP surgery. Thus, we believe that the TSCP will be clinical routine surgery for controlling vertigo in MD when considering preservation of remaining hearing.
Figure 1. Surgical procedures of TSCP.
Disclosure statement
The authors report no conflicts of interest.
Additional information
Funding
References
- Hallpike CS, Cairns H. Observations on the pathology of Meniere’s syndrome (section of otology). Proc R Soc Med. 1938;31(11):1317–1336.
- Liu Y, Yang J, Duan M. Current status on researches of Meniere’s disease: a review. Acta Otolaryngol. 2020;140(10):808–812.
- Basura GJ, Adams ME, Monfared A, et al. Clinical practice guideline: Meniere’s disease. Otolaryngol Head Neck Surg. 2020;162(2_suppl):S1–S55.
- Luca P, Ralli M, Cassandro C, et al. Surgical management of intractable Meniere’s disease. Int Tinnitus J. 2022;26(1):50–56. doi: 10.5935/0946-5448.20220007.
- Jacob R, Lauer G, Ernst A, et al. Triple semi-circular canal occlusion and cochlear implantation: a treatment option for single-sided Meniere’s disease with functional deafness-a case series. J Clin Med. 2023;12(17):5500.
- Gentine A, Martin E, Schultz P, et al. Lateral semicircular canal plugging: a simple and effective surgical treatment against incapacitating Meniere’s disease. Rev Laryngol Otol Rhinol (Bord). 2008;129(1):11–16.
- Yin S, Chen Z, Yu D, et al. Triple semicircular canal occlusion for the treatment of Meniere’s disease. Acta Otolaryngol. 2008;128(7):739–743.
- Zhang D, Fan Z, Han Y, et al. Triple semicircular canal plugging: a novel modality for the treatment of intractable Meniere’s disease. Acta Otolaryngol. 2016;136(12):1230–1235.
- Zhang D, Lv Y, Han Y, et al. Long-term outcomes of triple semicircular canal plugging for the treatment of intractable Meniere’s disease: a single center experience of 361 cases. J Vestib Res. 2019;29(6):315–322. doi: 10.3233/VES-190682.
- Gill C, Muzaffar J, Kumar R, et al. Triple canal occlusion for the treatment of intractable Meniere’s disease. Otol Neurotol. 2021;42(1):116–120. doi: 10.1097/MAO.0000000000002841.
- Li X, Lyu Y, Li Y, et al. Triple semicircular canal plugging versus labyrinthectomy for Meniere disease: a retrospective study. Laryngoscope. 2023;133(11):3178–3184. doi: 10.1002/lary.30690.
- Zhang DG, Xu L, Han YC, et al. Simultaneous triple semicircular canal plugging and cochlear implantation in advanced Meniere’s disease. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2017;52(1):25–30.
- Lyu Y, Zhang D, Li X, et al. Dexamethasone protects the hearing of Meniere’s disease patients after triple semicircular canal plugging. Acta Otolaryngol. 2020;140(10):803–807.