
Abstract
The objective of this study was to evaluate three passive upper-extremity exoskeletons relative to a control condition. Twelve subjects performed an hour-long, simulated occupational task in a laboratory setting. Independent measures of exoskeleton, exertion height (overhead, head height), time, and their interactions were assessed. Dependent measures included changes in tissue oxygenation (ΔTSI) in the anterior deltoid and middle trapezius, peak resultant lumbar spine loading, and subjective discomfort in various body regions. A statistically significant reduction in ΔTSI between exoskeleton and control was only observed in one instance. Additionally, neither increases in spinal loading nor increases in subjective discomfort ratings were observed for any of the exoskeletons. Ultimately, the exoskeletons offered little to no physiological benefit for the conditions tested. However, the experimental task was not highly fatiguing to the subjects, denoted by low ΔTSI values across conditions. Results may vary for tasks requiring constant arm elevation or higher force demands.
Practitioner summary This study quantified the benefits of upper-extremity exoskeletons using NIRS, complementary to prior studies using EMG. The exoskeletons offered little to no physiological benefit for the conditions tested. However, the experimental task was not highly fatiguing, and results may vary for an experimental task with greater demand on the shoulders.
Abbreviations: WMSD: work-related musculoskeletal disorder; EMG: electromyography; NIRS: near-infrared spectroscopy; NIR: near-infrared; Hb: haemoglobin; Mb: myoglobin; TSI: tissue saturation index; ATT: adipose tissue thickness
1. Introduction
Work-related musculoskeletal disorders (WMSDs) represent a major problem in modern occupational environments, in which 53.4% of cases involve the back or shoulders (U.S. Bureau of Labor Statistics Citation2018). In response to these prevalent WMSDs, industrial exoskeletons have been introduced into occupational environments in private industry. ASTM International defines the term exoskeleton as a “wearable device that augments, enables, or assists, and/or enhances physical activity, through mechanical interaction with the body” (ASTM Citation2020). This rather broad definition includes both “active” exoskeletons that are powered by actuators such as electric motors or hydraulics and “passive” exoskeletons that counterbalance human movement with springs or other materials capable of storing energy (Howard et al. Citation2020). Different types of exoskeletons also exist depending on which body region the device is designed to assist. Upper-extremity exoskeletons, for example, have been designed to combat shoulder-related WMSDs. These exoskeletons assist individuals working in jobs that require arm elevation, such as supporting the weight of the arms or a tool during overhead work.
Yin et al., Citation2020; Bock et al. Citation2021). However, there are some limitations of this type of approach that are worth noting. First, studies relying on EMG to detect differences in muscle activity with and without an exoskeleton relied on the assumption that reduced muscle activation yields decreases in muscle fatigue and ultimately, a reduction in injury risk. Though this is a valid assumption, using the time-domain EMG signal to measure muscle activation represents a proxy (rather than direct) measure for muscle fatigue. While spectral EMG variables including the mean frequency and median frequency can be used to assess muscle fatigue, especially for isometric muscle contractions (Phinyomark et al. Citation2012; Scano et al. Citation2020), few of the aforementioned exoskeleton studies actually performed this type of analysis. Additionally, while the concept of using mean or median frequency shifts to quantify muscle fatigue has been considered the “gold standard” in the literature for decades, no published standards exist regarding the amount of median frequency shift that actually defines fatigue (Szucs, Navalgund, and Borstad Citation2009), and the sensitivity of this method has previously been questioned relative to the shoulder muscles during simulated occupational work (Ferguson et al. Citation2013). Regarding biomechanical modelling approaches, most existing shoulder models rely on an optimization-based inverse dynamics approach when estimating shoulder loading. However, this type of modelling approach often ignores antagonist muscle co-contraction and may subsequently underestimate actual tissue loads (Xu, Lin, and McGorry Citation2017).
Thus, while evidence provided from prior exoskeleton studies using biomechanical methods provide some useful data, further study of the effects of upper-extremity exoskeletons on shoulder muscle fatigue using an alternate method is also warranted. Instead of using EMG to measure the effects of upper-extremity exoskeletons in the shoulders, physiological measures related to oxidative metabolism could provide a more appropriate picture of the potential of industrial exoskeletons to reduce occupational injury. A multitude of studies have explored the metabolic effects of both low back and upper-extremity exoskeletons, and a recent systematic review reports that the majority of these studies recorded significant reductions in the mean values of metabolic or cardiorespiratory parameters considered (Del Ferraro et al. Citation2020). However, these studies measured global changes rather than localised metabolic changes occurring in the individual muscles of target body areas. Localised muscle fatigue is an important factor to consider, as there is evidence that localised muscle fatigue may cause increased muscle coactivity, altered joint kinematics, and reduced tissue tolerance (Psek and Cafarelli Citation1993; Potvin and O’Brien Citation1998; Boushel et al. Citation2001; Marras et al. Citation2006), thereby increasing musculoskeletal injury risk.
Fortunately, advances in non-invasive and portable Near-Infrared Spectroscopy (NIRS) technology streamlines the understanding of localised muscle fatigue and offers the ability to understand how upper-extremity exoskeletons change the capacity of the shoulder muscles to do work and the subsequent likelihood of muscle fatigue or injury. NIRS technology involves measuring the absorbance of light at two or more wavelengths in the near-infrared (NIR) range (650–1000 nm) in a region of interest between a light source and detector(s) (Jones et al. Citation2016). As the absorbance of haemoglobin (Hb) and myoglobin (Mb) in the blood depends on whether they are in the oxygenated or deoxygenated state (Jones et al. Citation2016; Barstow Citation2019), relative oxy-/deoxy- Hb + Mb concentrations can be estimated using the modified Beer-Lambert law (Ferrari and Quaresima Citation2012; Scholkmann et al. Citation2014). NIRS has previously been shown to be a sensitive tool to detect changes in shoulder muscle fatigue for simulated occupational work (Ferguson et al. Citation2013). It has also been applied to evaluate a “muscle suit” low-back exoskeleton previously (Muramatsu and Kobayashi Citation2014), though to the authors’ knowledge, no study to date has utilised NIRS to measure muscle fatigue when evaluating upper-extremity exoskeletons.
Additional barriers exist before industrial exoskeletons are at advanced enough level of readiness for most workplaces (Howard et al. Citation2020). For example, prior studies have tested exoskeletal devices on only a small number of (mostly male) subjects, have tested the devices over short time durations, and have failed to fully assess the trade-offs associated with the use of the devices (particularly biomechanical and physiological changes in non-target body areas). Relative to the last point (trade-offs), the scientific literature relative to the effects of upper-extremity exoskeletons also remains contradictory. For example, Theurel et al. (Citation2018) noted that upper-extremity exoskeletons may increase antagonist muscle activity, postural strains, and cardiovascular demand. Similarly, Weston et al. (Citation2018) noted an increase in compressive spinal loads of up to 56.8% with the use of an exoskeletal vest and tool support arm, suggesting that the upper-extremity exoskeleton tested may reduce shoulder injury risk at the cost of an increased risk for a low back injury. In contrast, the same exoskeletal vest was tested by Kim, Nussbaum, Mokhlespour Esfahani, Alemi, Jia, and Rashedi (Citation2018), who noted reductions in spinal loading of up to 30% when at higher vertical exertion heights and a smaller moment arm from the spine. This discrepancy points towards the fact that the context with which an upper-extremity exoskeleton is used (and tested) can drastically influence the results.
The present study hopes to address some of these stated limitations. When designing the study, special considerations were made regarding (1) the measurement of muscle fatigue using NIRS rather than EMG, (2) the duration of time for which the exoskeletons are tested, and (3) the measurement of not only the potential physiological benefits of upper-extremity exoskeletons but also potential side effects (changes to spinal loading or user-rated discomfort). The primary objective of this laboratory study was to understand the impact of three commercially available upper-extremity exoskeletons on tissue oxygenation in two shoulder muscles (the anterior deltoid and middle trapezius) during simulated overhead work tasks performed over a one-hour duration. A secondary objective of this study was to document potential trade-offs, including changes to spinal loading and subjective discomfort ratings.
2. Methods
2.1. Approach
This laboratory study compared three upper-extremity exoskeletons (Ekso Bionics Ekso Vest, Levitate AIRFRAME, suitX ShoulderX) against a no exoskeleton condition (control) to understand the impact of upper-extremity exoskeletons on tissue oxygen saturation in the shoulder muscles (right and left middle trapezius and anterior deltoid), peak resultant lumbar spinal loading, and subjective discomfort in various body regions during a simulated occupational task performed at two heights (head height and overhead).
2.2. Subjects
Six male subjects (age 21.2 ± 2.9 (SD) years, mass 79.8 ± 10.1 kg, and height 179.5 ± 4.2 cm) and six female subjects (age 22.5 ± 3.3 years, mass 57.6 ± 6.8 kg, and height 165.5 ± 7.1 cm) were recruited from the local university population. This sample size was determined a priori via a power analysis and was deemed appropriate to detect a small (10%) effect size at a power level of 0.90. As pilot data were not available, this power analysis relied on data collected from Yang et al. (Citation2007), who used NIRS to assess changes to the tissue saturation index (TSI) and subsequent muscle fatigue from repetitive lifting exertions. Change in TSI also represents the primary outcome of interest herein (see below), so it is expected that use of data from this former study provided an adequate comparison point, even though NIRS data was collected on low back muscles in the former study and collected on shoulder muscles in this study. None of the subjects recruited for this study reported any low back or shoulder pain within the past 3 years. Additionally, none of the subjects had any prior experience in manual materials handling or using an occupational exoskeleton. Subjects gave informed consent per the study protocol, which was approved by the University’s Institutional Review Board.
2.3. Experimental design
2.3.1. Independent variables
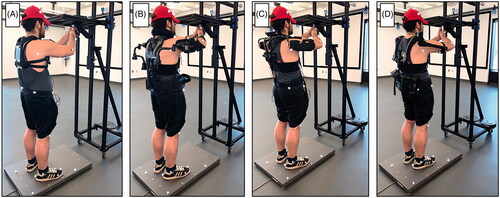
A balanced 4 × 2 design was implemented in this study, representing eight total combinations of four exoskeleton conditions (control, EksoVest, AIRFRAME, ShoulderX, as shown in ) and two exertion heights (head height and overhead). Each exoskeleton condition was collected for subjects in different sessions, one per week for four weeks. The first session was always the control condition, and the order of the remaining exoskeleton sessions was counterbalanced across subjects. Each individual session consisted of the two 1-h exertion height conditions with a 1-h break between these conditions for recovery. The order of the exertion height conditions was randomised. The effect of time (0–15 min, 15–30 min, 30–45 min, 45–60 min) within each experimental condition was also evaluated for physiological and biomechanical measures described herein.
Figure 1. Exoskeleton conditions tested including (A) the control condition (no exoskeleton), (B) the Ekso Vest, (C) the AIRFRAME, and (D) the ShoulderX. All exoskeletons tested were designed to support the upper extremities during occupational work and are commercially available.
2.3.2. Dependent variables
Dependent measures consisted of: (1) changes in the tissue saturation index (TSI) in the aforementioned shoulder muscles at various time points throughout the hour-long condition, (2) the peak resultant load on the lumbar spine at various time points throughout the hour-long condition, and (3) subjective discomfort in multiple body regions after each experimental condition.
NIRS was used to monitor mean changes in the TSI (ΔTSI) in the right and left anterior deltoid and middle trapezius muscles across two-minute windows spaced five minutes apart throughout each one-hour condition. TSI is defined as the ratio of oxygenated haemoglobin (and myoglobin) to total haemoglobin (and myoglobin) under the optode surface (Ferrari, Muthalib, and Quaresima Citation2011).
Peak resultant lumbar spinal loads were quantified using an EMG-assisted spine model for one-minute windows spaced five minutes apart throughout each condition. The biomechanical model estimates spinal loads extending from T12/L1 to L5/S1 and has been described extensively in the literature (Hwang, Knapik, Dufour, Aurand, et al. Citation2016; Hwang, Knapik, Dufour, Aurand, Best, et al. Citation2016).
Generalised subjective discomfort was quantified via a questionnaire administered at the end of each condition. Subjects were asked to rate their level of discomfort (either musculoskeletal discomfort or discomfort from contact with exoskeleton parts, etc.) on a numerical scale ranging from 0 to 10, wherein 0 corresponded to no discomfort at all, 0.5–2 corresponded to light discomfort, 3–5 corresponded to moderate discomfort, and 6–10 corresponded to high discomfort. Subjects rated their discomfort for the right and left shoulders, chest, upper back, upper arms, forearms, wrists and hands, hips, thighs, knees, lower legs, and ankles and feet. Discomfort ratings were also assessed for the abdomen and lower back.
2.3.3. Experimental task
The experimental task for this study involved repetitively exerting 10 lbs. of vertical force against a hand transducer (a type of load cell) and sustaining that force for two seconds. Subjects repeated this task at a frequency of 6 exertions per minute for 1 h. Subjects were instructed to stand directly behind the hand transducer and use both hands. Thus, the task was assumed to be symmetric in the sagittal plane and place equal demand on the left and right sides of the body. Subjects were free to perform the experimental task at a self-selected distance from the hand transducer based on what felt most comfortable. Audible tones signalled to the subject when to begin each repetition, when their vertical force reached to 10 lbs., when they had successfully sustained the force for 2 s, and if/when the subject had failed to sustain the force for the required duration of time. If subjects failed the task within the first second of sustaining the force (i.e. dropped below the necessary sustained force level), they were instructed to try again. If subjects failed the task after sustaining the force for longer than one second, investigators made note of this, and subjects rested until the next repetition. Subjects were not explicitly instructed on what to do with their arms between exertions (i.e. hold the arms in constant elevation vs. elevate and lower the arms for each exertion), though all subjects chose the latter strategy, especially as time progressed.
2.4. Apparatus and instrumentation
The three exoskeletons tested included the Ekso Vest (Ekso Bionics, Richmond, CA, USA), AIRFRAME (Levitate Industries Inc., San Diego, CA, USA), and ShoulderX (suitX, US Bionics, Inc., Emeryville, CA, USA). These three exoskeletons are commercially available and (from personal observation) appear to be the most widely used in the United States in private industry at this time. The level of support by the exoskeletons was held constant across subjects and sessions and corresponded to “medium” levels of support in all three devices. The hand transducer was mounted to a custom T-slotted aluminium frame (80/20 Inc., Columbia City, IN, USA). The tool that was used to exert the force was light weight (approximately 1 kg), pestle-shaped, and fabricated in the laboratory.
A wireless continuous dual-wave near-infrared spectrophotometer (PortaLite, Artinis Medical Systems, Arnhem, The Netherlands) was used to quantify TSI in aforementioned shoulder muscles. Each optode emits wavelengths of 748 and 840 nm from diodes spaced 30, 35, and 40 mm from a single photodiode receiver. This configuration allows TSI to be calculated using a spatially-resolved approach (Suzuki et al. Citation1999; Ferrari, Muthalib, and Quaresima Citation2011). A differential path-length factor of 4.0 was incorporated to correct for scattering of light in the tissue, and NIRS measurements were acquired at a frequency of 10 Hz.
Electromyographic activity was collected using a wireless TrignoTM system (Delsys, Natick, MA, USA) and bipolar surface electrodes placed bilaterally onto the lumbar erector spinae, internal oblique, latissimus dorsi, external oblique, and rectus abdominis. EMG data were sampled at 1925.93 Hz (standard for the Trigno system), and signals were notch filtered at 60 Hz and its aliases, bandpass filtered between 30 and 450 Hz, rectified and smoothed, and low-pass filtered using a second-order Butterworth filter with a cut-off frequency of 1.59 Hz, consistent with standards for reporting EMG data (Merletti Citation1999). Kinematic data were collected via a 42-camera optical motion capture system (Optitrack Prime 41, NaturalPoint, Corvallis, OR, USA) with a 120 Hz sampling rate and were low-pass filtered using a fourth-order Butterworth filter with a cut-off frequency of 10 Hz. Finally, kinetic data were captured at a 1000 Hz sampling rate from both the six-axis load cell at the subjects’ feet (6090-15, Bertec, Worthington, OH, USA) and the custom-built six-axis hand transducer (HT0825, Bertec, Worthington, OH, USA) mounted to the aluminium frame. Signals were gathered with customised laboratory software and synchronised via a data acquisition board (USB-6225, National Instruments, Austin, TX, USA).
2.5. Procedure
During the first session, subjects provided informed consent. Anthropometric measures were collected, including stature, weight, waist circumference, and the breadth and width of the torso at the level of the sternum and umbilicus. Subjects then stood on the load cell in order to record appropriate exertion heights (head height and overhead) for the subject. These heights were recorded and used during all other experimental sessions. Head height corresponded to approximately 90 degrees of shoulder flexion and was close to eye level. The overhead exertion height corresponded to approximately 110 degrees of shoulder flexion. During the first (control) session, the experimental task was also described to the subjects at this time (see section 2.3.3), and the subjects were provided with 10–15 min to familiarise themselves with the task. Alternatively, if an exoskeleton was to be used in the session, the subject next donned the exoskeleton, and it was fit to the subject according to manufacturer recommendations. Subjects were allowed 15–20 min to get comfortable with the exoskeleton and practice the experimental task while wearing it before doffing the device to prepare the subject with the necessary sensors for the data collection.
Subjects were prepared with surface electrodes on the aforementioned 10 torso muscles in accordance with standard placement guidelines (Mirka and Marras Citation1993) and 41 reflective motion capture markers placed in accordance with a custom full-body marker set prescribed by OptiTrack’s motion capture software. Finally, NIRS optodes were placed into secure holders and secured to the skin on top of the muscle bellies of each subject’s right and left trapezius and anterior deltoid muscles using double-sided adhesive tape. For the trapezius, optodes were placed halfway along the line extending between the vertebra prominens and the acromion process of the scapula. For the anterior deltoid, a point two thirds the distance between the clavicular notch and acromion process was first located, and optodes were placed one third the distance between this point and the olecranon process of the ulna. After sensor placement was complete, the biomechanical model was calibrated using data derived from a series of dynamic concentric and eccentric lumbar motions while holding a 9.07 kg medicine ball. This calibration technique has been described previously (Dufour, Marras, and Knapik Citation2013).
After model calibration, subjects once again donned the exoskeleton device if applicable, and the first experimental condition was subsequently collected. At the start of the experimental condition, subjects were instructed to stand for one minute in a relaxed upright position with their arms relaxed by their sides, during which time baseline tissue saturation data was collected for each of the four shoulder muscles. Then, subjects began the experimental task. At the end of the hour, subjects doffed the exoskeleton (if applicable) and were given an hour of rest, during which time they were first asked to complete the discomfort questionnaire and then permitted to sit and relax. After the break, the same process as described above was conducted for the second exertion height. Subjects filled out another discomfort survey before leaving for the day.
2.6. Analysis
TSI data were collected continuously from one minute prior to the experimental task through the end of the experimental task. The mean of the TSI signal was first calculated across the minute of data prior to the experimental task and utilised as baseline data, from which ΔTSI could eventually be calculated. Two-minute windows of TSI data spaced 5-min apart throughout the hour (t = 2–4, 7–9, …, 57–59 min) were then extracted for each of the four muscles. The twelve local minima in the TSI signal across each two-minute window (resulting from repetitions of the experimental task during that time) were extracted using a custom script written in MATLAB (The MathWorks, Natick, MA, USA). The mean of these local minima was calculated, and ΔTSI was calculated by subtracting the baseline TSI value from this mean. In order to assess the effect of time, ΔTSI values for each muscle were also grouped based on the fifteen-minute chunk of time from which the data were collected.
Lumbar spinal loads were derived via simulations in a multibody dynamics solver, Adams (MSC Software, Santa Ana, CA, USA) by combining dynamic inputs of lumbar muscle EMG-activations, full-body kinematics, and kinetics into the aforementioned EMG-driven lumbar spine model. As was the case for the NIRS data, spinal loads were assessed at 5-min time intervals throughout each hour-long experimental condition. However, because infrared light from the optical motion capture system interfered with the infrared light required to collect the NIRS data, spinal loads were assessed at different time points than the NIRS data (t = 0, 5, 10, …, 55, 59 min). The peak resultant spinal load across all lumbar levels extending from T12/L1 to L5/S1 was calculated for each time point, though only the lumbar level with the highest magnitude of loading was used in the statistical analysis. As was done with the NIRS data, peak spinal loads for the rest of the time points were also stratified based on fifteen-minutes chunks of time, though peak spinal loads recorded for the first minute of the task (t = 0 min) were ultimately discarded because subjects were noted to need the first few minutes of each hour to (re)acclimate to the task.
Statistical analyses were performed using JMP 14.0 Pro software (SAS Institute Inc., Cary, NC, USA), and statistical significance was interpreted relative to a significance level α = 0.05. The effects of the independent variables and their interactions on the physiological (ΔTSI) and biomechanical (resultant spinal loading) measures were assessed using a generalised linear mixed model. In each model, exoskeleton, exertion height, time, and their two-way interactions were introduced as fixed effects, while subject and interactions involving subject were introduced as random effects. Higher order (three-, four-way) interaction effects were included in the model’s residual/error term. For instances in which a significant p value was observed in a fixed effect test, effect details were assessed using either a least squares means differences Student’s t test or a least squares means Tukey HSD test where appropriate. Regarding the subjective discomfort data, descriptive statistics were used to ascertain the body regions resulting in the highest levels of discomfort and whether any differences in the ratings existed between the right and left sides of the body. Due to the ordinal nature of the subjective discomfort data, the effects of the exoskeleton condition were assessed using a Kruskal-Wallis non-parametric test and a nonparametric post-hoc test (Wilcoxon’s multiple comparisons test).
3. Results
Statistically significant main and interaction effects are shown in . Regarding the physiological and biomechanical variables, main effects of exoskeleton or exertion height were rare, but an exoskeleton * height interaction effect was observed in all instances. However, exoskeleton * time and height * time interaction effects were never significant.
Table 1. Statistically significant main and interaction effects for each of the dependent variables.
3.1. Physiological data (ΔTSI)
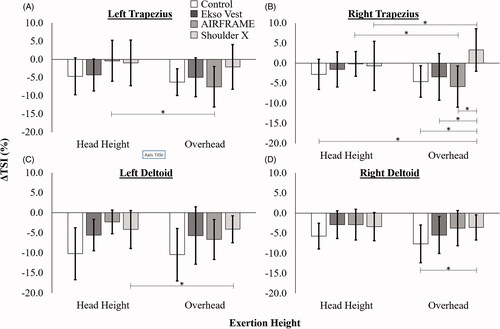
There were no instances in which a significant main effect of exoskeleton was noted for ΔTSI, and exertion height was only noted to influence ΔTSI in the left trapezius (p = 0.012). However, a statistically significant exoskeleton * exertion height interaction effect was noted in all four of the shoulder muscles (left trapezius p < 0.001, right trapezius p < 0.001, left anterior deltoid p < 0.001, right anterior deltoid p = 0.004). As shown in , a significant increase in the magnitude of ΔTSI between head height and overhead exertion heights was noted for the AIRFRAME in both the left and right trapezius muscles. In the right trapezius, ΔTSI for the ShoulderX at the overhead exertion also differed significantly from all other groups except the Esko Vest at head height; this was also the only combination of exoskeleton/height conditions that saw an increase in TSI from baseline rather than a decrease. In the left anterior deltoid, the only statistically significant difference among groups was between exertion heights for the ShoulderX, wherein the magnitude of ΔTSI was greater in the head height condition than overhead. Likewise, in the right anterior deltoid, the only statistically significant difference among groups was between the control and ShoulderX exoskeleton conditions at the overhead exertion height, wherein the magnitude of ΔTSI was greater in the control condition.
Figure 2. ΔTSI in the (A) left trapezius, (B) right trapezius, (C) left anterior deltoid, and (D) right anterior deltoid muscles stratified by exoskeleton condition and exertion height. Error bars denote standard deviation. *Denotes a statistically significant difference between groups at a significance level of 0.05.
As shown in , time was also noted to affect ΔTSI in all muscles except the right trapezius. Post-hoc results generally suggested that ΔTSI was greatest in magnitude during the first fifteen minutes of the exertion and decreased in magnitude throughout the hour-long task.
Table 2. Mean (SD) ΔTSI in each of the four should muscles evaluated with respect to time (0–15 min, 15–30 min, 30–45 min, and 45–60 min).
3.2. Biomechanical data (resultant spinal load)
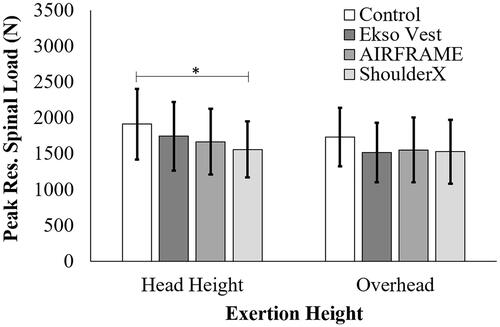
The biomechanical model predicted peak resultant spinal loading values (a combination of compression and shear loading) to occur at the L4/L5 vertebral level. In terms of main effects, the control condition was noted to have significantly higher resultant spinal loads than the ShoulderX exoskeleton condition, while the Ekso Vest and AIRFRAME did not differ significantly from either the control condition or the ShoulderX (p = 0.028). However, a significant exoskeleton * exertion height interaction effect (p < 0.001) suggested that this result only held true for the exertions performed at head height, not overhead (). A statistically significant main effect of exertion height was also noted, for which resultant spinal loads were significantly higher at head height than overhead across all four exoskeleton conditions (p = 0.006). Time did not affect spinal loading (p = 0.101), nor did time interact with either the exoskeleton or height variables.
Figure 3. Peak L4/L5 Resultant Spinal Loads stratified by exoskeleton condition and exertion height. Error bars denote standard deviation. *Denotes a statistically significant difference between exoskeleton conditions at a significance level of 0.05.
3.3. Subjective discomfort
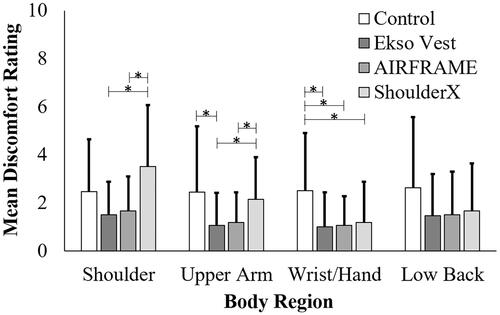
Discomfort ratings were similar between the right and left sides of the body, so only values for the right side of the body will be discussed herein. The experimental task led to light discomfort in most body regions across all the exoskeleton and exertion height conditions. The body regions that were consistently rated to have the highest discomfort scores were the shoulders (mean rating of 2.3 across all exoskeleton and height conditions), upper arms (mean rating 1.7), the hands and wrists (mean rating 1.4), and the lower back (mean rating 1.9) (). In these four body regions, discomfort ratings were noted to differ significantly according to the exoskeleton condition in the shoulders (p = 0.002), upper arms (p = 0.028), and hands and wrists (p = 0.049), but not the lower back (p = 0.352). In the shoulder, discomfort was significantly higher for the ShoulderX than the Ekvo Vest (p < 0.001) and AIRFRAME (p = 0.002), though the control condition did not vary significantly from any of the exoskeletons tested. The same effect was observed for the upper arms (ShoulderX > Ekso Vest, p = 0.012 and ShoulderX > AIRFRAME, p = 0.025), though discomfort was also noted to be reduced for the Ekso Vest relative to the control condition (p = 0.047). In the hands/wrists, discomfort was higher for the control condition than all three of the exoskeletons (compared to Ekso Vest, p = 0.015; compared to AIRFRAME, p = 0.041; compared to ShoulderX, p = 0.048).
Figure 4. Mean subjective discomfort rating in the most affected body regions after performing the 1-hour experimental task (across both exertion heights). Error bars denote standard deviation. *Denotes a statistically significant difference between exoskeleton conditions at a significance level of 0.05, as noted by a pairwise Wilcoxon’s multiple comparisons test.
4. Discussion
This laboratory study leveraged continuous-wave NIRS and an advanced biomechanical model to assess physiological and biomechanical variables for three upper-extremity exoskeletons compared to a control condition. While physiological (NIRS) data assessed the potential benefits of these exoskeletons relative to the control condition, the biomechanical and subjective discomfort data measured potential trade-offs associated their use, especially in non-target body regions. ΔTSI values trended closer to zero across the four muscles tested with the use of the exoskeletons compared to the control condition, but differences between the exoskeleton and control conditions were not statistically significant, except for one instance (ShoulderX relative to control at the overhead height). In terms of the potential trade-offs, none of the three exoskeletons led to increased loading on the lumbar spine, and one exoskeleton (the ShoulderX) even led to a statistically significant reduction in resultant spinal loading relative to control at head height. No significant differences in subjective discomfort results were observed for any of the exoskeletons relative to the control condition.
Upper-extremity exoskeletons are designed to assist individuals working in postures that require shoulder elevation, such as supporting the weight of the arms or tool during drilling, countersinking, bucking, and riveting. To date, a multitude of studies have noted positive biomechanical and physiological results for this class of exoskeleton. These results include reductions in muscle activity during static and dynamic movements (Rashedi et al. Citation2014, Kim, Nussbaum, Mokhlespour Esfahani, Alemi, Alabdulkarim, and Rashedi 2018; Theurel et al. Citation2018; Alabdulkarim and Nussbaum Citation2019; Gillette and Stephenson Citation2019; Schmalz et al. Citation2019; Grazi et al. Citation2020; Iranzo et al. Citation2020; Yin et al. 2020), decreases in the sum of joint torque in the upper arm (Sylla et al. Citation2014), decreases in the effective load on the shoulder joint (Naito et al. Citation2007), and decreases in heart rate (Schmalz et al. Citation2019; Grazi et al. Citation2020). That being said, physiological measures related to oxygen utilisation in the surrounding musculature can provide a complementary picture of how upper-extremity exoskeletons alter the capacity for muscles to do work and the subsequent likelihood of muscle fatigue. To the authors’ knowledge, this study represents the first attempt to evaluate upper-extremity exoskeleton effectiveness using NIRS on individual shoulder muscles.
In a former study with a similar experimental task, the tissue oxygenation/saturation index measure was shown to be less sensitive than directly assessing changes to oxygenated haemoglobin (Ferguson et al. Citation2013). However, ΔTSI was chosen for this study given the multi-day experimental protocol because this measure accounts for the influence of the superficial tissue layer, and its values can be compared directly across subjects (Jones et al. Citation2016). If effective, the exoskeleton conditions should have yielded ΔTSI values closer to zero (i.e. baseline) than the control conditions. This is because larger decreases in ΔTSI suggest that more oxygen is being used up by the mitochondria in the muscles during each contraction. Our results showed that ΔTSI values were closer to zero across the four muscles tested with the use of the exoskeletons, as indicated by 15–134% reductions in ΔTSI in the right and left trapezius muscles and 36–56% reductions in ΔTSI in the right and left anterior deltoid muscles for the exoskeleton conditions relative to the control condition across both exertion heights. However, the only statistically significant changes for any of the exoskeleton conditions relative to the control condition were in the right trapezius and right anterior deltoid muscles (both with the ShoulderX at head height).
The magnitude of ΔTSI values herein only ranged between 1.9% and 7.3%. In contrast, Baláš et al. (Citation2018) noted ΔTSI values of approximately 8% in the forearm muscles of climbers for 8 second contractions performed at 60% MVC, while Jones and Cooper (Citation2018) noted ΔTSI of approximately 10% in the vastus lateralis muscles during synchronised swimming. Larger changes in TSI of approximately 15% have been recorded in the vastus lateralis muscle during light intensity cycling (40% peak aerobic power) (Leung et al. Citation2010), and even larger changes of up to 40–50% have been noted for maximal concentric and eccentric bicep contractions (Muthalib et al. Citation2010). When placed in context with results from these prior studies, it becomes clear that the experimental task may not have been as fatiguing to subjects as originally anticipated. At the force level chosen, there was in general a lack of statistically significant findings in the the physiological shoulder data attributable to the exoskeleton condition, even at the high (0.90) power level calculated a priori for the number of subjects tested. In particular, the ability of the subjects to lower their arms between exertions could have allowed for additional muscle recovery and increased blood flow to the shoulder muscles throughout the hour-long task (relative to the arms being constantly elevated), contributing to the lack of statistically significant results observed. However, the simulated occupational task performed by the subjects in this study is still believed to accurately represent overhead work tasks that might be performed in the field. There are, of course, some occupational tasks where the arms are constantly elevated. However, tasks in which the arms are elevated and lowered at a high frequency (as tested here) are also prevalent. Additionally, it remains unclear how the results would differ at either higher or lower force levels, as force demands vary significantly among the many jobs that might implement an upper-extremity exoskeleton in the field.
Exoskeletons are designed to potentiate joint movement or transfer load elsewhere in the body, thus leading to potential side-effects. For this reason, we considered not only the physiological benefits of the upper-extremity exoskeletons but also its effects on lumbar spine loading and subjective discomfort. Mean peak resultant spinal loads for all the exoskeleton conditions were 10–15% lower than the control condition in this study, though there was only one instance in which any statistically significant differences attributable to the exoskeleton condition was noted (the ShoulderX relative to the control condition at the overhead height). Kim, Nussbaum, Mokhlespour Esfahani, Alemi, Jia, and Rashedi (Citation2018) reported up to a 30% reduction in spinal loading as an “unexpected” benefit of using an exoskeletal vest, which was not observed presently. However, at the very least, these results suggest that there was not a cost of using any of the three exoskeletons to the lumbar spine. These results are contrary to a prior upper-extremity exoskeleton study (of a very different design) that used the same biomechanical model and noted rather large increases in spinal loading with exoskeleton use (Weston et al. Citation2018). However, it should be noted that external moments acting on the lumbar spine in this referenced study were increased considerably from a mechanical arm supporting the hand tool at a far distance from the body, whereas the moment arm between the spine and the tool was much shorter presently.
Finally, it should be noted that whereas the ShoulderX performed the best in terms of the physiological and biomechanical measures, the ShoulderX consistently received the worst discomfort ratings via questionnaire. This could be because contact forces on this device were likely higher than the other two exoskeletons, leading to increased discomfort. Though contact forces were not measured directly, 8 of the 12 subjects reported discomfort arising from the ShoulderX exoskeleton in the shoulders and neck resulting from the device contacting their skin in the “notes” section next to their discomfort rating in their discomfort questionnaire. These results reinforce the recommendation that contact forces and other related considerations (i.e. hygiene, distraction/vigilance changes) should also be fully considered prior to exoskeleton adoption in the field (Howard et al. Citation2020). These results also suggest that individuals are less perceptive to changes in internal factors such as fatigue or tissue loading than they are to external factors like contact stress.
Of course, the results of this study should also be placed in context with its limitations. First, this study was performed in a laboratory setting with young subjects inexperienced in manual materials handling. The subjects’ inexperience led to the decision to collect the control condition first in all subjects, rather than adding the control condition to the counterbalance structure (the study team wanted the subjects to be familiar with the experimental task before introducing any additional intervention/changes). This may have introduced the potential that an order effect could have confounded the results. However, this potential order effect was more likely to affect the dependent measures favourably (as the subjects learned how to better perform the experimental task with time), rather than unfavourably and was not likely to be a large issue given our lack of statistically significant findings herein. Additionally, only one subjective discomfort scale was used. Therefore, it is not possible to separate out the contribution of musculoskeletal discomfort versus discomfort arising from the exoskeleton interventions (i.e. contact pressures) from the overall discomfort scores, unless the subjects noted which type of discomfort they were feeling in the “notes” section that was provided next to each rating on the questionnaire.
Because of the large time commitment per subject to collect all the experimental conditions, subjects were provided limited training/familiarization with the exoskeleton devices before collecting any data. Similarly, due to time constraints, just one experimental task was performed by the subjects at one force level. Thus, it remains unclear how the results may have differed at other force levels, exertion heights, or exertion frequencies. However, based upon industrial observations our task was indicative of common industrial overhead work. Moreover, the restorative force provided by each of the three exoskeletons was held constant to “medium” levels of support. Thus, the exact force provided by each of the exoskeletons at this level was likely to vary within a few pounds.
Finally, the reliability of the NIRS signal has been noted to be influenced by factors including adipose tissue thickness (ATT) and tissue movement during muscle contraction (Barstow Citation2019). While ATT was not assessed for any of the subjects, they were generally of a healthy weight for their stature (average body mass index of 22.9), and the multiple source-detector approach used by the PortaLite system allows for signals to be recorded in skeletal muscle independent of superficial tissue (Ferreira et al. Citation2005; Yu et al. Citation2005; Jones et al. Citation2016). Likewise, in regard to tissue movement, the sensors and subsequently the region of interest could have shifted over each one-hour experimental task, particularly between baseline and the experimental task. Collecting baseline data prior to each experimental condition with the arms elevated rather than down in a neutral position would have better mitigated the effects of tissue movement. However, each repetition throughout the hour-long experimental task was also largely isometric, which suggests that the underlying tissue was not moving during the actual exertions when changes in TSI were most important.
5. Conclusion
This study evaluated three different commercially available upper-extremity exoskeletons (Ekso Vest, AIRFRAME, ShoulderX) against a control condition for a simulated, repetitive occupational task. The benefits of the exoskeletons to the shoulders were assessed using physiological (i.e. NIRS) rather than biomechanical methods (i.e. EMG). The physiological measure associated with oxygen utilisation in the right and left middle trapezius and anterior deltoid muscles (ΔTSI) were reduced for the exoskeleton conditions by 15–134% in the right and left trapezius muscles and by 36–56% in the right and left anterior deltoid muscles relative to the control condition. However, these reductions were not statistically significant, except for in one instance (the ShoulderX exoskeleton at overhead height), in part because low magnitudes of the ΔTSI measure were recorded for the experimental task (ΔTSI values ranged between 1.9% and 7.3%). Together, these results suggest that the upper-extremity exoskeletons offered little to no physiological benefit for the conditions tested, but also that the experimental task was not as fatiguing as initially anticipated. Thus, results may differ for a more demanding task, such as a task requiring constant arm elevation or a higher force level. In addition to measuring the benefits of the exoskeletons on the shoulder, potential trade-offs (changes to lumbar spinal loading and subjective discomfort) were also assessed. Biomechanically, the exoskeletons yielded similar (or even reduced) spinal loads relative to the control condition. Likewise, subjective discomfort in multiple body regions did not differ significantly between exoskeleton and control conditions. These subjective discomfort ratings seemed to be based most on contact forces, and subjects appeared to be less perceptive to changes in internal factors such as fatigue or tissue loading.
Disclosure statement
The authors report no financial interest or benefit derived from this work.
Additional information
Funding
References
- Alabdulkarim, S., and M. A. Nussbaum. 2019. “Influences of Different Exoskeleton Designs and Tool Mass on Physical Demands and Performance in a Simulated Overhead Drilling Task.” Applied Ergonomics 74: 55–66. doi:https://doi.org/10.1016/j.apergo.2018.08.004.
- ASTM. 2020. F3323-20 Standard Terminology for Exoskeletons and Exosuits. West Conshohocken, PA: ASTM International.
- Baláš, J., J. Kodejška, D. Krupková, J. Hannsmann, and S. Fryer. 2018. “Reliability of near-Infrared Spectroscopy for Measuring Intermittent Handgrip Contractions in Sport Climbers.” The Journal of Strength & Conditioning Research 32 (2): 494–501. https://journals.lww.com/nsca-jscr/Fulltext/2018/02000/Reliability_of_Near_Infrared_Spectroscopy_for.24.aspx.
- Barstow, T. J. 2019. “Understanding Near Infrared Spectroscopy and Its Application to Skeletal Muscle Research.” Journal of Applied Physiology (Bethesda, Md. : 1985) 126 (5): 1360–1376. doi:https://doi.org/10.1152/japplphysiol.00166.2018.
- Bock, S. D., J. Ghillebert, R. Govaerts, S. A. Elprama, U. Marusic, B. Serrien, A. Jacobs, J. Geeroms, R. Meeusen, and K. D. Pauw. 2021. “Passive Shoulder Exoskeletons: More Effective in the Lab than in the Field?” IEEE Transactions on Neural Systems and Rehabilitation Engineering : a Publication of the IEEE Engineering in Medicine and Biology Society 29: 173–183. doi:https://doi.org/10.1109/TNSRE.2020.3041906.
- Boushel, R., H. Langberg, J. Olesen, J. Gonzales-Alonzo, J. Bülow, and M. Kjaer. 2001. “Monitoring Tissue Oxygen Availability with near Infrared Spectroscopy (Nirs) in Health and Disease.” Scandinavian Journal of Medicine & Science in Sports 11 (4): 213–222. doi:https://doi.org/10.1034/j.1600-0838.2001.110404.x.
- Del Ferraro, S., T. Falcone, A. Ranavolo, and V. Molinaro. 2020. “The Effects of Upper-Body Exoskeletons on Human Metabolic Cost and Thermal Response during Work Tasks—a Systematic Review.” International Journal of Environmental Research and Public Health 17 (20): 7374. doi:https://doi.org/10.3390/ijerph17207374.
- Dufour, J.S., W.S. Marras, and G.G. Knapik. 2013. “An Emg-Assisted Model Calibration Technique That Does Not Require Mvcs.” Journal of Electromyography and Kinesiology : official Journal of the International Society of Electrophysiological Kinesiology 23 (3): 608–613. doi:https://doi.org/10.1016/j.jelekin.2013.01.013.
- Ferguson, S.A., W.G. Allread, P. Le, J. Rose, and W.S. Marras. 2013. “Shoulder Muscle Fatigue during Repetitive Tasks as Measured by Electromyography and near-Infrared Spectroscopy.” Human Factors 55 (6): 1077–1087. doi:https://doi.org/10.1177/0018720813482328.
- Ferrari, M., M. Muthalib, and V. Quaresima. 2011. “The Use of Near-Infrared Spectroscopy in Understanding Skeletal Muscle Physiology: Recent Developments.” Philosophical Transactions. Series A, Mathematical, Physical, and Engineering Sciences 369 (1955): 4577–4590. doi:https://doi.org/10.1098/rsta.2011.0230.
- Ferrari, M., and V. Quaresima. 2012. “A Brief Review on the History of Human Functional near-Infrared Spectroscopy (fNIRS) Development and Fields of Application.” NeuroImage 63 (2): 921–935. doi:https://doi.org/10.1016/j.neuroimage.2012.03.049.
- Ferreira, L. F., D. K. Townsend, B. J. Lutjemeier, and T. J. Barstow. 2005. “Muscle Capillary Blood Flow Kinetics Estimated from Pulmonary O2 Uptake and near-Infrared Spectroscopy.” Journal of Applied Physiology 98 (5): 1820–1828. doi:https://doi.org/10.1152/japplphysiol.00907.2004.
- Gillette, J.C., and M.L. Stephenson. 2019. “Electromyographic Assessment of a Shoulder Support Exoskeleton during on-Site Job Tasks.” IISE Transactions on Occupational Ergonomics and Human Factors 7 (3-4): 302–310. doi:https://doi.org/10.1080/24725838.2019.1665596.
- Grazi, L., E. Trigili, G. Proface, F. Giovacchini, S. Crea, and N. Vitiello. 2020. “Design and Experimental Evaluation of a Semi-Passive Upper-Limb Exoskeleton for Workers with Motorized Tuning of Assistance.” IEEE Transactions on Neural Systems and Rehabilitation Engineering : A Publication of the IEEE Engineering in Medicine and Biology Society 28 (10): 2276–2285. doi:https://doi.org/10.1109/TNSRE.2020.3014408.
- Howard, J., V. V. Murashov, B. D. Lowe, and M.-L. Lu. 2020. “Industrial Exoskeletons: Need for Intervention Effectiveness Research.” American Journal of Industrial Medicine 63 (3): 201–208. doi:https://doi.org/10.1002/ajim.23080.
- Hwang, J., G. G. Knapik, J. S. Dufour, A. Aurand, T. M. Best, S. N. Khan, E. Mendel, and W. S. Marras. 2016a. “A Biologically-Assisted Curved Muscle Model of the Lumbar Spine: Model Structure.” Clinical Biomechanics (Bristol, Avon) 37: 53–59. doi:https://doi.org/10.1016/j.clinbiomech.2016.06.002.
- Hwang, J., G. G. Knapik, J. S. Dufour, T. M. Best, S. N. Khan, E. Mendel, and W. S. Marras. 2016b. “A Biologically-Assisted Curved Muscle Model of the Lumbar Spine: Model Validation.” Clinical Biomechanics (Bristol, Avon) 37: 153–159. doi:https://doi.org/10.1016/j.clinbiomech.2016.07.009.
- Iranzo, S., A. Piedrabuena, D. Iordanov, U. Martinez-Iranzo, and J. -M. Belda-Lois. 2020. “Ergonomics Assessment of Passive Upper-Limb Exoskeletons in an Automotive Assembly Plant.” Applied Ergonomics 87: 103120. doi:https://doi.org/10.1016/j.apergo.2020.103120.
- Jones, B., and C.E. Cooper. 2018. “Near Infrared Spectroscopy (nirs) Observation of Vastus Lateralis (Muscle) and Prefrontal Cortex (Brain) Tissue Oxygenation during Synchronised Swimming Routines in Elite Athletes.” In Oxygen Transport to Tissue xl, edited by O. Thews, J. C. Lamanna, and D. K. Harrison, 111–117. Cham: Springer International Publishing.
- Jones, S., S.T. Chiesa, N. Chaturvedi, and A.D. Hughes. 2016. “Recent Developments in Near-Infrared Spectroscopy (NIRS) for the Assessment of Local Skeletal Muscle Microvascular Function and Capacity to Utilise Oxygen .” Artery Research 16: 25–33. doi:https://doi.org/10.1016/j.artres.2016.09.001.
- Kim, S., M. A. Nussbaum, M. I. Mokhlespour Esfahani, M. M. Alemi, S. Alabdulkarim, and E. Rashedi. 2018a. “Assessing the Influence of a Passive, Upper Extremity Exoskeletal Vest for Tasks Requiring Arm Elevation: Part I – “Expected” Effects on Discomfort, Shoulder Muscle Activity, and Work Task Performance.” Applied Ergonomics 70: 315–322. doi:https://doi.org/10.1016/j.apergo.2018.02.025.
- Kim, S., M. A. Nussbaum, M. I. Mokhlespour Esfahani, M. M. Alemi, B. Jia, and E. Rashedi. 2018b. “Assessing the Influence of a Passive, Upper Extremity Exoskeletal Vest for Tasks Requiring Arm Elevation: Part II – “Unexpected” Effects on Shoulder Motion, Balance, and Spine Loading.” Applied Ergonomics 70: 323–330. doi:https://doi.org/10.1016/j.apergo.2018.02.024.
- Leung, T. S., A. Wittekind, T. Binzoni, R. Beneke, C. E. Cooper, and C. E. Elwell. 2010. “Muscle Oxygen Saturation Measured Using “Cyclic Nir Signals” During Exercise.” In Oxygen Transport to Tissue XXXI, edited by E. Takahashi and D. F. Bruley, 183–189. Boston, MA: Springer US.
- Marras, W. S., J. Parakkat, A. M. Chany, G. Yang, D. Burr, and S. A. Lavender. 2006. “Spine Loading as a Function of Lift Frequency, Exposure Duration, and Work Experience.” Clinical Biomechanics (Bristol, Avon) 21 (4): 345–352. doi:https://doi.org/10.1016/j.clinbiomech.2005.10.004.
- Merletti, R. 1999. “Standards for Reporting Emg Data.” Journal of Electromyography and Kinesiology 9 (1): 3–4.
- Mirka, G. A., and W. S. Marras. 1993. “A Stochastic Model of Trunk Muscle Coactivation during Trunk Bending.” Spine (Phila Pa 1976) 18 (11): 1396–1409. https://www.ncbi.nlm.nih.gov/pubmed/8235810.
- Muramatsu, Y., and H. Kobayashi. 2014. “Assessment of Local Muscle Fatigue by Nirs - Development and Evaluation of Muscle Suit.” ROBOMECH Journal 1 (1): 19. doi:https://doi.org/10.1186/s40648-014-0019-2.
- Muthalib, M., H. Lee, G. Y. Millet, M. Ferrari, and K. Nosaka. 2010. “Comparison Between Maximal Lengthening and Shortening Contractions for Biceps Brachii Muscle Oxygenation and Hemodynamics.” Journal of Applied Physiology 109 (3): 710–720. doi:https://doi.org/10.1152/japplphysiol.01297.2009.
- Naito, J., G. Obinata, A. Nakayama, and K. Hase. 2007. “Development of a Wearable Robot for Assisting Carpentry Workers.” International Journal of Advanced Robotic Systems 4 (4): 48. [Accessed 2020/05/13]. doi:https://doi.org/10.5772/5667.
- Phinyomark, A., S. Thongpanja, H. Hu, P. Phukpattaranont, and C. Limsakul. 2012. “The Usefulness of Mean and Median Frequencies in Electromyography Analysis.” In Computational Intelligence in Electromyography Analysis: A Perspective on Current Applications and Future Challenges, 195–220. Rijeka, Croatia: InTech.
- Potvin, J. R., and P. R. O’brien. 1998. “Trunk Muscle co-Contraction Increases During Fatiguing, Isometric, Lateral Bend Exertions. Possible Implications for Spine Stability. Spine (Phila Pa).” Spine 23 (7): 774–780; discussion 781. doi:https://doi.org/10.1097/00007632-199804010-00006.
- Psek, J. A., and E. Cafarelli. 1993. “Behavior of Coactive Muscles During Fatigue.” Journal of Applied Physiology 74 (1): 170–175. doi:https://doi.org/10.1152/jappl.1993.74.1.170.
- Rashedi, E., S. Kim, M. A. Nussbaum, and M. J. Agnew. 2014. “Ergonomic Evaluation of a Wearable Assistive Device for Overhead Work.” Ergonomics 57 (12): 1864–1874. doi:https://doi.org/10.1080/00140139.2014.952682.
- Scano, A., I. Pirovano, M. E. Manunza, L. Spinelli, D. Contini, A. Torricelli, and R. Re. 2020. “Sustained Fatigue Assessment During Isometric Exercises with Time-Domain near Infrared Spectroscopy and Surface Electromyography Signals.” Biomedical Optics Express 11 (12): 7357–7375. doi:https://doi.org/10.1364/BOE.403976.
- Schmalz, T., J. Schändlinger, M. Schuler, J. Bornmann, B. Schirrmeister, A. Kannenberg, and M. Ernst. 2019. “Biomechanical and Metabolic Effectiveness of an Industrial Exoskeleton for Overhead Work.” International Journal of Environmental Research and Public Health 16 (23): 4792. doi:https://doi.org/10.3390/ijerph16234792.
- Scholkmann, F., S. Kleiser, A. J. Metz, R. Zimmermann, J. Mata Pavia, U. Wolf, and M. Wolf. 2014. “A Review on Continuous Wave Functional Near-Infrared Spectroscopy and Imaging Instrumentation and Methodology.” NeuroImage 85 Pt 1: 6–27. doi:https://doi.org/10.1016/j.neuroimage.2013.05.004.
- Suzuki, S., S. Takasaki, T. Ozaki, and Y. Kobayashi. 1999. “Tissue Oxygenation Monitor Using NIR Spatially Resolved Spectroscopy." Proc. SPIE 3597, Optical Tomography and Spectroscopy of Tissue III, (15 July 1999). doi:https://doi.org/10.1117/12.356862.
- Sylla, N., V. Bonnet, F. Colledani, and P. Fraisse. 2014. “Ergonomic Contribution of Able Exoskeleton in Automotive Industry.” International Journal of Industrial Ergonomics 44 (4): 475–481. doi:https://doi.org/10.1016/j.ergon.2014.03.008.
- Szucs, K., A. Navalgund, and J.D. Borstad. 2009. “Scapular Muscle Activation and co-Activation following a Fatigue Task.” Medical & Biological Engineering & Computing 47 (5): 487–495. doi:https://doi.org/10.1007/s11517-009-0485-5.
- Theurel, J., K. Desbrosses, T. Roux, and A. Savescu. 2018. “Physiological Consequences of Using an Upper Limb Exoskeleton During Manual Handling Tasks.” Applied Ergonomics 67: 211–217. doi:https://doi.org/10.1016/j.apergo.2017.10.008.
- U. S. Bureau of Labor Statistics. 2018. “Back Injuries Prominent in Work-Related Musculoskeletal Disorder Cases in 2016.” The Economics Daily.
- Weston, E. B., M. Alizadeh, G. G. Knapik, X. Wang, and W. S. Marras. 2018. “Biomechanical Evaluation of Exoskeleton Use on Loading of the Lumbar Spine.” Applied Ergonomics 68: 101–108. doi:https://doi.org/10.1016/j.apergo.2017.11.006.
- Xu, X., J. Lin, and R. W. McGorry. 2017. “An Entropy-Assisted Musculoskeletal Shoulder Model.” Journal of Electromyography & Kinesiology 33: 103–110. https://www.sciencedirect.com/science/article/pii/S1050641116301924#b0040
- Yang, G., A. M. Chany, J. Parakkat, D. Burr, and W. S. Marras. 2007. “The Effects of Work Experience, Lift Frequency and Exposure Duration on Low Back Muscle Oxygenation.” Clinical Biomechanics (Bristol Avon), 22 (1): 21–27. doi:https://doi.org/10.1016/j.clinbiomech.2006.07.005.
- Yin, P., L. Yang, S. Qu, and C. Wang. 2020. “Effects of a Passive Upper Extremity Exoskeleton for Overhead Tasks.” Journal of Electromyography and Kinesiology : official Journal of the International Society of Electrophysiological Kinesiology 55: 102478 doi:https://doi.org/10.1016/j.jelekin.2020.102478.
- Yu, G., T. Durduran, G. Lech, C. Zhou, B. Chance, E. Mohler, and A. Yodh. 2005. “Time-Dependent Blood Flow and Oxygenation in Human Skeletal Muscles Measured with Noninvasive Near-Infrared Diffuse Optical Spectroscopies.” Journal of Biomedical Optics 10 (2): 024027. doi:https://doi.org/10.1117/1.1884603.